Abg analysis.. Based on standard book and mention reference.. Make it simplified.. Neet pg and inicet 9riented.. Routine life example in complecated concept... Add related picture
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
I now have all the content needed. Let me write the comprehensive ABG guide:
ABG Analysis - Complete Guide for NEET PG / INICET
References: Harrison's Principles of Internal Medicine 22e (Ch. 58, DuBose) | Ganong's Review of Medical Physiology 26e | Symptom to Diagnosis: Evidence-Based Guide 4e | Roberts & Hedges' Clinical Procedures in Emergency Medicine | Barash Clinical Anesthesia 9e
PART 1: NORMAL VALUES - THE "PHONE NUMBER" to Memorize
| Parameter | Normal Value | Mnemonic |
|---|---|---|
| pH | 7.35 - 7.45 | "7.40 is perfect" |
| PaCO2 | 35 - 45 mmHg | "40 is perfect" |
| HCO3- | 22 - 26 mEq/L | "24 is perfect" |
| PaO2 | 80 - 100 mmHg | "90 is perfect" |
| SaO2 | 95 - 100% | - |
Quick recall trick: pH 7.4 | PaCO2 40 | HCO3 24 - just like 7-40-24
PART 2: THE HENDERSON-HASSELBALCH EQUATION (Why ABG Works)
pH = 6.1 + log [HCO3-] / (0.03 × PaCO2)
Simple version to remember:
pH depends on HCO3/PaCO2 ratio
- HCO3 = "Kidney controls this" (slow, days)
- PaCO2 = "Lungs control this" (fast, minutes)
Daily life analogy: Imagine your blood is like a swimming pool. The pH is the water quality. HCO3 is like the baking soda you add (base), and CO2 is like acid leaking in. Your lungs are the quick drain valve (fast, minutes), and kidneys are the slow filter system (days).
PART 3: THE 7-STEP ABG APPROACH (Most High-Yield for NEET PG)
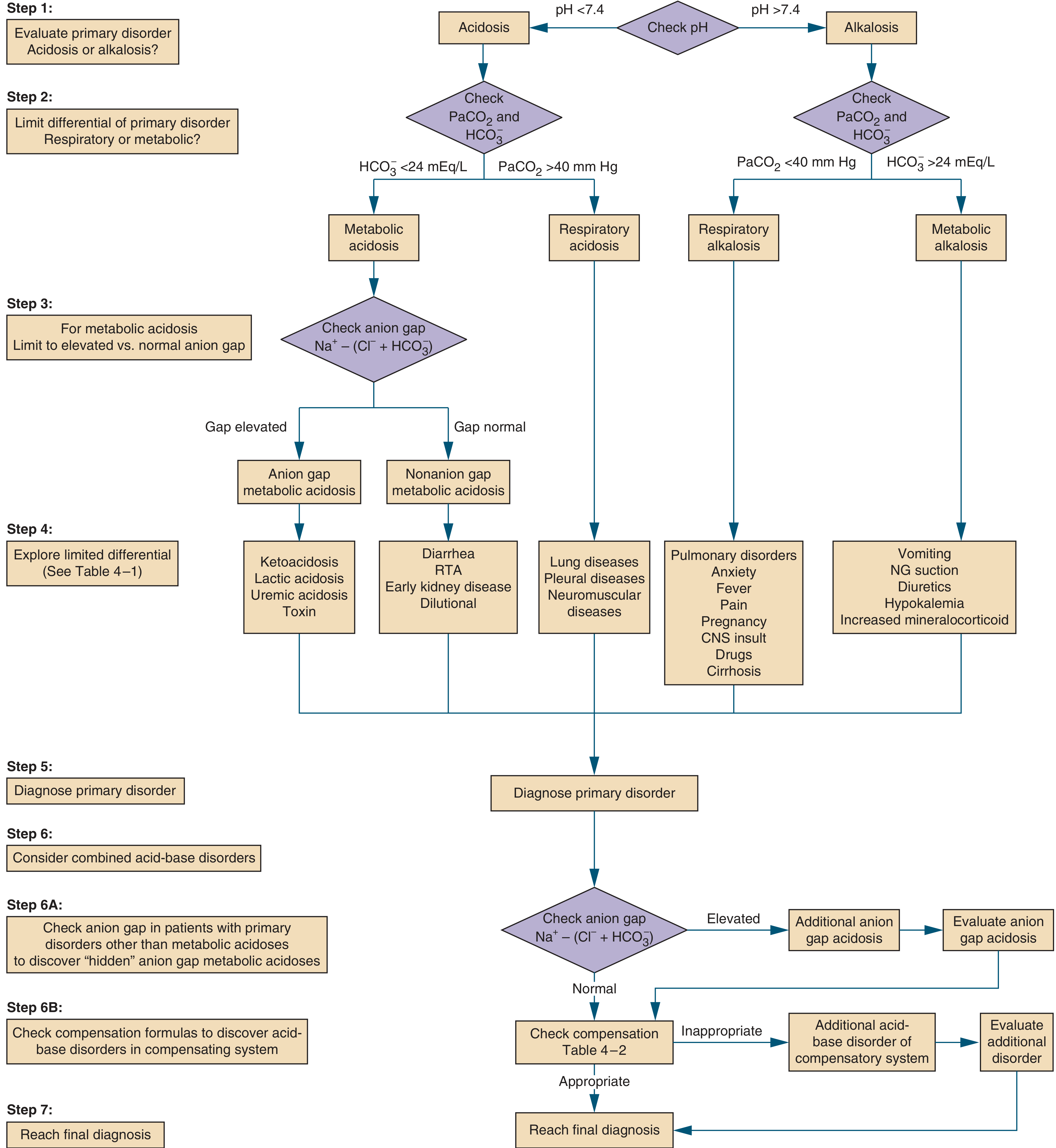
STEP 1: Is the patient Acidotic or Alkalotic?
- pH < 7.35 = Acidosis
- pH > 7.45 = Alkalosis
- pH 7.35-7.45 = Normal (but may still have mixed disorder!)
Exam tip: If pH is on the acidic side (< 7.4) even within normal range - underlying disorder is acidosis. If pH is on alkalotic side (> 7.4) - underlying disorder is alkalosis.
STEP 2: Is it Metabolic or Respiratory?
For Acidosis (pH < 7.35):
- PaCO2 HIGH (> 45) → Respiratory Acidosis (lungs retaining CO2)
- HCO3 LOW (< 22) → Metabolic Acidosis (kidneys losing buffer)
For Alkalosis (pH > 7.45):
- PaCO2 LOW (< 35) → Respiratory Alkalosis (lungs blowing off CO2)
- HCO3 HIGH (> 26) → Metabolic Alkalosis (too much buffer)
Memory table:
| Disorder | pH | PaCO2 | HCO3 |
|---|---|---|---|
| Respiratory Acidosis | ↓ | ↑ | ↑ (compensatory) |
| Respiratory Alkalosis | ↑ | ↓ | ↓ (compensatory) |
| Metabolic Acidosis | ↓ | ↓ (compensatory) | ↓ |
| Metabolic Alkalosis | ↑ | ↑ (compensatory) | ↑ |
Golden Rule: The primary disorder and its cause always move in the SAME direction. CO2 and pH move OPPOSITE. HCO3 and pH move SAME direction.
STEP 3: Calculate Anion Gap (for Metabolic Acidosis)
Formula:
AG = Na+ - (Cl- + HCO3-)
Normal = 8-12 mEq/L (most commonly cited as 12 ± 4)
Daily life analogy: Imagine your blood is a balance sheet. Na+ is your total income. Cl- and HCO3- are your known expenses. The anion gap is the "unexplained spending" - the money that's gone somewhere you can't account for (hidden acids!).
High Anion Gap Metabolic Acidosis - Mnemonic: "A MUD PILE CAT" (from Roberts & Hedges)
| Letter | Cause |
|---|---|
| A | Aspirin (salicylate) overdose |
| M | Methanol, Metformin |
| U | Uremia (kidney failure) |
| D | Diabetic ketoacidosis |
| P | Paraldehyde, Phenformin |
| I | Isoniazid, Iron |
| L | Lactic acidosis |
| E | Ethylene glycol (antifreeze) |
| C | Carbon monoxide, Cyanide |
| A | Alcoholic ketoacidosis |
| T | Toluene |
Normal Anion Gap (Hyperchloremic) Metabolic Acidosis - Mnemonic: "USED CARP" or think Diarrhea/RTA
| Cause | Mechanism |
|---|---|
| Diarrhea | Losing HCO3 in stool |
| RTA (Renal Tubular Acidosis) | Kidney can't excrete H+ |
| Early CKD | Mild loss of H+ secretion |
| Dilutional | Large volume NS infusion |
| Carbonic anhydrase inhibitors (acetazolamide) | Blocks HCO3 reabsorption |
| Addison's disease | Aldosterone deficiency |
Key concept: High AG = hidden acid accumulating (the body is making acids). Normal AG = bicarbonate is being lost (through gut or kidney) and Cl- rises to compensate - that's why it's called "hyperchloremic."
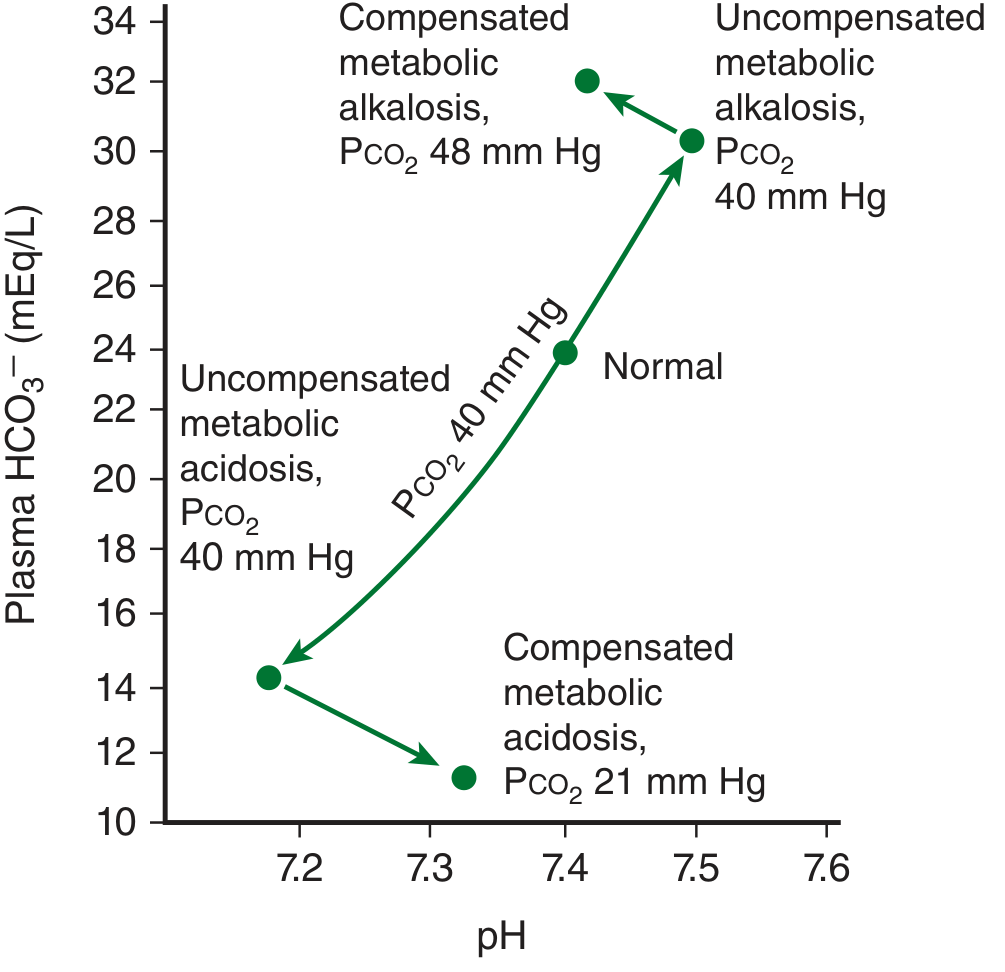
STEP 4: Check Compensation (Most Important for MCQs!)
Compensation never fully corrects pH. It only moves pH toward normal, not to normal. (Exception: chronic respiratory alkalosis can normalize pH.)
Compensation Formulas (HIGH YIELD - NEET PG)
1. Metabolic Acidosis (Winter's Formula) - (Harrison's 22e, Table 58-1)
Expected PaCO2 = (1.5 × HCO3) + 8 ± 2
OR: PaCO2 falls 1.25 mmHg per 1 mEq/L fall in HCO3
Memory trick: "1.5 × bicarb + 8" - like 1.5 liters water + 8 cups coffee = the Winters recipe!
- If actual PaCO2 < expected → additional respiratory alkalosis
- If actual PaCO2 > expected → additional respiratory acidosis
2. Metabolic Alkalosis (Harrison's 22e)
Expected PaCO2 = 0.75 × HCO3 + 0 (or rises 0.75 mmHg per 1 mEq/L rise in HCO3)
(Lungs hypoventilate to retain CO2 and bring pH down)
3. Respiratory Acidosis (Roberts & Hedges)
Acute: HCO3 rises 1 mEq/L per 10 mmHg rise in PaCO2
Chronic: HCO3 rises 4 mEq/L per 10 mmHg rise in PaCO2
Daily life analogy: Acute = you just held your breath for 10 seconds. Chronic = COPD patient who has been retaining CO2 for months. Kidneys have had time to compensate fully in chronic.
4. Respiratory Alkalosis (Harrison's 22e)
Acute: HCO3 falls 2 mEq/L per 10 mmHg fall in PaCO2
Chronic: HCO3 falls 5 mEq/L per 10 mmHg fall in PaCO2
Summary table (MEMORIZE THIS):
| Primary Disorder | Expected Compensation | Key Formula |
|---|---|---|
| Metabolic Acidosis | PaCO2 ↓ | PaCO2 = 1.5(HCO3) + 8 ± 2 |
| Metabolic Alkalosis | PaCO2 ↑ | PaCO2 rises 0.7 per 1↑ HCO3 |
| Resp. Acidosis (Acute) | HCO3 ↑ | +1 per 10 mmHg ↑CO2 |
| Resp. Acidosis (Chronic) | HCO3 ↑↑ | +4 per 10 mmHg ↑CO2 |
| Resp. Alkalosis (Acute) | HCO3 ↓ | -2 per 10 mmHg ↓CO2 |
| Resp. Alkalosis (Chronic) | HCO3 ↓↓ | -5 per 10 mmHg ↓CO2 |
STEP 5: Delta-Delta Ratio (Δ/Δ) - Detecting Mixed Disorders
When to use: Only in HIGH ANION GAP metabolic acidosis
Δ/Δ = (Observed AG - Normal AG) / (Normal HCO3 - Observed HCO3)
= (AG - 12) / (24 - HCO3)
Interpretation (Barash Clinical Anesthesia 9e):
| Δ/Δ Ratio | Interpretation |
|---|---|
| < 1 | Mixed High AG + Normal AG metabolic acidosis |
| 1 - 2 | Pure high anion gap metabolic acidosis |
| > 2 | High AG metabolic acidosis + Metabolic alkalosis |
Daily life analogy: Think of the Delta-Delta like checking if there is a hidden problem behind a visible one. Example: A diabetic with DKA (visible problem = high AG acidosis) but who has also been vomiting for days (hidden problem = metabolic alkalosis from vomit loss). The Δ/Δ > 2 exposes this hidden alkalosis.
PART 4: THE 4 SIMPLE DISORDERS - Causes & Clinical Features
1. Respiratory Acidosis
= Hypoventilation = CO2 buildup
Causes (CNS to lung to chest wall):
| Category | Examples |
|---|---|
| CNS depression | Opioids, sedatives, CNS lesions |
| Neuromuscular | Guillain-Barre, Myasthenia gravis, Poliomyelitis |
| Chest wall | Kyphoscoliosis, flail chest |
| Airway | COPD (most common chronic), severe asthma, foreign body |
| Parenchymal | Severe pneumonia, ARDS |
Daily life analogy: Respiratory acidosis = someone sitting on your chest. You can't breathe out CO2. CO2 builds up. Blood gets acidic.
Clinical features: Confusion, drowsiness, headache (CO2 vasodilates cerebral vessels), papilledema in chronic cases, asterixis ("CO2 narcosis")
2. Respiratory Alkalosis
= Hyperventilation = CO2 blown off
Causes mnemonic: "PHAT FCDAP"
| Cause | Example |
|---|---|
| Pulmonary | PE, pneumonia, pulmonary edema |
| Hypoxia | High altitude, severe anemia |
| Anxiety | Panic attack (most common in young women) |
| Toxins | Salicylates (early), progesterone, nicotine |
| Fever | Any infection |
| CNS | Stroke, meningitis |
| Drugs | Amphetamines |
| Autonomic | Pain, shock |
| Pregnancy | Progesterone stimulates respiratory center |
Daily life analogy: Respiratory alkalosis = anxious student breathing rapidly before an exam. You breathe so fast, you blow out too much CO2. Blood pH rises. You feel tingling in fingertips (from Ca2+ binding more tightly to albumin in alkalosis → hypocalcemia symptoms).
Clinical features: Tetany, perioral tingling, Chvostek's/Trousseau's sign (hypocalcemia), carpopedal spasm, dizziness
3. Metabolic Acidosis
= Too much acid OR lost too much HCO3
Key sign: Kussmaul breathing - deep, labored, rapid breathing (compensating for metabolic acidosis by blowing off CO2)
Daily life analogy: Kussmaul breathing = a car engine overheating. The cooling fan (lungs) goes on overdrive to cool the engine (remove CO2 = remove acid).
Two types (decide by AG):
- High AG = acid ADDED to blood (see A MUD PILE CAT above)
- Normal AG = HCO3 LOST from body (diarrhea, RTA)
Clinical features of acidosis: Hyperkalemia (H+ enters cells, K+ exits), decreased cardiac contractility, Kussmaul breathing, confusion, osteoporosis (chronic)
Hyperkalemia in acidosis explained: Imagine K+ and H+ are tenants sharing an apartment (the cell). When too many H+ ions arrive (acidosis), some K+ tenants get kicked out into the blood. Hence hyperkalemia in acidosis, hypokalemia in alkalosis.
4. Metabolic Alkalosis
= Too much HCO3 OR lost too much acid
Causes:
| Saline-Responsive (Urine Cl < 20) | Saline-Resistant (Urine Cl > 20) |
|---|---|
| Vomiting/NG suction | Primary hyperaldosteronism |
| Diuretics (thiazide, loop) | Cushing's syndrome |
| Post-hypercapnic state | Hypokalemia (severe) |
| Contraction alkalosis | Bartter/Gitelman syndrome |
Vomiting causes alkalosis - you lose HCl from stomach. Losing acid = blood becomes alkaline.
Clinical features: Hypokalemia, hypocalcemia, weakness, cramps, arrhythmias, tetany
PART 5: MIXED ACID-BASE DISORDERS (Harrison's 22e, Ch. 58)
A mixed disorder = two or more primary disorders happening at the same time.
| Mixed Disorder | Clinical Example |
|---|---|
| Metabolic acidosis + Respiratory alkalosis | Sepsis, aspirin overdose, liver failure |
| Metabolic acidosis + Respiratory acidosis | Severe pneumonia, pulmonary edema + shock |
| Metabolic alkalosis + Respiratory alkalosis | Liver disease on diuretics, pregnancy with vomiting |
| Metabolic alkalosis + Respiratory acidosis | COPD on diuretics (most classic NEET PG scenario) |
| High AG + Normal AG acidosis (mixed metabolic) | Diarrhea + DKA |
| High AG acidosis + Metabolic alkalosis | Uremia + vomiting |
How to detect: If compensation is inappropriate (too much or too little), there is a mixed disorder. Use the Δ/Δ ratio for metabolic acidosis.
PART 6: CLASSIC NEET PG / INICET VIGNETTES
Vignette 1
A 30-year-old diabetic patient comes with vomiting and weakness. ABG: pH 7.15, PaCO2 20, HCO3 6. Na 138, Cl 100.
Steps:
- pH 7.15 - Acidosis
- HCO3 6 (low) - Primary Metabolic Acidosis
- AG = 138 - (100+6) = 32 → High AG Metabolic Acidosis → DKA likely
- Expected PaCO2 (Winter's) = 1.5(6) + 8 = 17 ± 2 → Actual PaCO2 = 20 → slightly higher than expected → additional Respiratory Acidosis component
- Final: DKA with mixed metabolic + mild respiratory acidosis (Case adapted from Symptom to Diagnosis 4e)
Vignette 2
COPD patient on diuretics. ABG: pH 7.42, HCO3 42, PaCO2 67, Cl 88.
Classic COPD + diuretics pattern (Harrison's 22e):
- Both PaCO2 and HCO3 are elevated (abnormal in opposite directions)
- pH is near normal - looks "normal" but is NOT
- This is Metabolic Alkalosis + Respiratory Acidosis (mixed)
- COPD causes chronic respiratory acidosis → compensatory high HCO3; diuretics cause additional metabolic alkalosis
Vignette 3
Young woman hyperventilating due to anxiety. ABG: pH 7.56, PaCO2 24, HCO3 21.
- pH 7.56 - Alkalosis
- PaCO2 24 (low) - Primary Respiratory Alkalosis
- Check compensation: Acute RAlk → HCO3 falls 2 mEq/L per 10 mmHg fall in PaCO2
- PaCO2 fell from 40 to 24 = fall of 16 mmHg
- Expected HCO3 fall = (16/10) × 2 = 3.2 → HCO3 should be ~21 ✓ (appropriate compensation)
- This is Pure Respiratory Alkalosis (appropriate acute compensation)
PART 7: QUICK MEMORY AIDS
pH Direction Rule
The primary disorder is the one whose change MATCHES the pH direction.
- pH down → acidosis → is PaCO2 up OR HCO3 down? That one is PRIMARY.
"ROME" mnemonic
- Respiratory = Opposite (pH and CO2 go opposite)
- Metabolic = Equal (pH and HCO3 go same direction)
Physiologic Compensation Logic
| "The lungs are fast" | "The kidneys are slow" |
|---|---|
| Compensate in minutes | Compensate in 3-5 days |
| CO2 is controlled by breathing | HCO3 is controlled by kidneys |
| Respiratory compensation for metabolic disorders | Metabolic compensation for respiratory disorders |
Urine Anion Gap (for Normal AG metabolic acidosis)
Urine AG = Urine Na+ + Urine K+ - Urine Cl-
Negative urine AG → Diarrhea (GI loss of HCO3)
Positive urine AG → RTA (kidney can't excrete NH4+/H+)
PART 8: ONE-LINE HIGH-YIELD FACTS FOR MCQs
- Aspirin overdose = early respiratory alkalosis (stimulates respiratory center), late metabolic acidosis
- Methanol/Ethylene glycol = high AG metabolic acidosis + elevated osmolal gap
- Vomiting = metabolic alkalosis (lose HCl) with hypokalemia and hypochloremia; saline-responsive
- Diarrhea = normal AG metabolic acidosis; NEGATIVE urine anion gap
- RTA Type 1 (distal) = normal AG acidosis, urine pH > 5.5, nephrocalcinosis, POSITIVE urine AG
- RTA Type 2 (proximal) = normal AG acidosis, urine pH < 5.5, Fanconi syndrome
- RTA Type 4 = hypoaldosteronism, hyperkalemia + normal AG acidosis (most common RTA)
- Pregnancy = mild respiratory alkalosis (progesterone stimulates breathing; compensated chronically)
- COPD = chronic respiratory acidosis (compensated); do NOT over-correct during mechanical ventilation
- Kussmaul breathing = deep labored breathing in metabolic acidosis (e.g., DKA)
- pH < 6.8 or > 7.8 = incompatible with life
- Compensation NEVER overcorrects pH (except chronic respiratory alkalosis)
- Loop/thiazide diuretics = metabolic alkalosis (lose H+ and Cl-)
- Acetazolamide = normal AG metabolic acidosis (blocks carbonic anhydrase)
- Hyperaldosteronism = metabolic alkalosis + hypokalemia; saline-RESISTANT
References:
- Harrison's Principles of Internal Medicine 22e, Ch. 58 (DuBose) - Acidosis and Alkalosis
- Ganong's Review of Medical Physiology 26e, Ch. 35 - Respiratory and Renal Compensation
- Symptom to Diagnosis: Evidence-Based Guide 4e, Ch. 4 - Stepwise ABG approach
- Roberts & Hedges' Clinical Procedures in Emergency Medicine - Acid-Base Balance, A MUD PILE CAT mnemonic
- Barash Clinical Anesthesia 9e, Ch. 16 - Delta-Delta ratio, ABG interpretation
- Tintinalli's Emergency Medicine - Arterial Blood Gas Analysis
Yes
Glad it was helpful! Is there a specific part of the ABG guide you'd like me to expand on — like more MCQ practice vignettes, deeper dive into RTA types, mixed disorders, or any particular topic for NEET PG/INICET prep?
First of all make concept then mcq
Asking for Preferences
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
Generate a comprehensive ABG concept guide in DOCX/PDF
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.