I now have excellent, comprehensive source material. Let me now compose the complete learning note. I have all the pharmacology from Lippincott, Adams & Victor, and Goodman & Gilman. Let me write the full note:
COMPLETE LEARNING NOTE: DRUG TREATMENT OF STROKE, HEADACHE & MIGRAINES
Sources: Lippincott Illustrated Reviews: Pharmacology | Adams and Victor's Principles of Neurology, 12th Ed. | Goodman & Gilman's Pharmacological Basis of Therapeutics | Bradley and Daroff's Neurology in Clinical Practice | Tintinalli's Emergency Medicine
PART A: STROKE - DRUG TREATMENT
SECTION 1: BIG PICTURE OVERVIEW - STROKE
What problem does stroke drug treatment solve?
Imagine your brain is the most powerful computer ever built. Every second, billions of electrical signals fire, allowing you to think, speak, move, and feel. This computer runs on one fuel: blood carrying oxygen and glucose.
Now imagine someone suddenly pinches off the power cable to one part of that computer. Within 4 minutes, that area begins to die. Within hours, the damage becomes permanent.
That is a stroke.
Drug treatment of stroke has ONE overwhelming goal: get blood flowing back to the dying brain tissue as fast as possible.
There are two types of stroke, and each requires a completely different approach:
| Type | What happens | What the drug must do |
|---|
| Ischemic stroke (85% of strokes) | A blood clot blocks an artery | Break the clot OR prevent more clots |
| Hemorrhagic stroke (15% of strokes) | A blood vessel bursts | Control bleeding, reduce pressure |
SECTION 2: BUILD THE FOUNDATION - STROKE
What normally happens in the brain's blood supply?
Your brain receives blood through two carotid arteries (front) and two vertebral arteries (back). These join at the base of the brain to form the Circle of Willis - a clever ring-road that provides alternative routes if one artery is blocked.
Normal blood flow:
- Brain uses 20% of the body's total oxygen despite being only 2% of body weight
- Cerebral blood flow = ~750 mL/min
- Brain has NO energy stores - it cannot survive even brief interruptions
What goes wrong in ischemic stroke?
Step-by-step pathway:
RISK FACTORS: Hypertension, diabetes, atrial fibrillation, smoking
↓
Atherosclerosis (fatty plaques build up inside artery walls)
↓
Plaque ruptures → Platelets rush to the site → Blood clot forms
↓
OR
Clot forms in heart (e.g., in atrial fibrillation) → travels to brain
↓
Artery blocked → Blood flow stops
↓
Ischemic penumbra: Area of dying tissue surrounds dead core
↓
Within minutes: Core infarction (dead tissue)
Within hours: Penumbra also dies if untreated
↓
Permanent neurological deficit
The Ischemic Penumbra - the most important concept in stroke treatment:
The penumbra (Latin: "partial shadow") is the area of brain tissue that is damaged but NOT yet dead after a stroke. It is still receiving some blood from collateral vessels. This tissue CAN be saved if you act quickly. The entire rationale for thrombolysis is to save the penumbra.
"Time is brain": Every minute a large stroke is untreated, approximately 1.9 million neurons die.
What goes wrong in hemorrhagic stroke?
Uncontrolled hypertension → Weakens small artery walls
↓
Aneurysm forms (balloon-like bulge) OR vessel ruptures directly
↓
Blood spills into brain tissue (intracerebral hemorrhage)
OR into the subarachnoid space (subarachnoid hemorrhage)
↓
Blood acts as toxin → Brain compression → Raised intracranial pressure
↓
Secondary brain injury
SECTION 3: DRUG CLASS FRAMEWORK - STROKE
PART 1: ACUTE ISCHEMIC STROKE TREATMENT
DRUG CLASS 1: THROMBOLYTICS (clot-busting drugs)
Definition
Thrombolytics are drugs that dissolve blood clots by activating the body's own clot-dissolving system.
Simple Analogy
Imagine a sink drain blocked by a big ball of hair. The thrombolytic drug is like a special chemical drain cleaner that dissolves the hair ball and restores water flow.
Mechanism of Action - Step by Step
Normal body: Plasminogen (inactive) → slowly converted to Plasmin (active)
Plasmin = the body's natural clot-dissolving enzyme
Plasmin cuts fibrin strands in the clot → clot dissolves
WITHOUT tPA: Conversion is too slow → clot stays → brain dies
WITH tPA:
tPA (tissue Plasminogen Activator) binds to fibrin in the clot
↓
tPA converts plasminogen → PLASMIN (rapidly)
↓
Plasmin cuts fibrin strands throughout the clot
↓
Clot breaks apart → blood flows again → brain tissue saved
The Main Drugs
| Drug | Type | Dose | Route | Key Feature |
|---|
| Alteplase (rt-PA) | Recombinant tPA | 0.9 mg/kg (max 90mg); 10% as IV bolus, rest over 60 min | IV | Gold standard; most evidence |
| Tenecteplase | Modified tPA | 0.25 mg/kg (max 25mg) | Single IV bolus | Higher fibrin specificity; longer half-life; easier to administer |
Time Window - THE MOST TESTED FACT
- Standard window: Within 4.5 hours of stroke onset
- The NINDS trial proved benefit within 3 hours
- The ECASS-3 trial extended this to 4.5 hours
- Recent meta-analyses (2025) suggest benefit may extend beyond 4.5 hours in selected patients with imaging-confirmed penumbra
The earlier you give it, the better. Treatment in the first 90 minutes is far more effective than treatment at 4 hours.
AHA/ASA Inclusion Criteria for IV Alteplase
| Criteria | Details |
|---|
| Age | ≥18 years |
| Onset of symptoms | <3 hours (standard); up to 4.5 hours (extended) |
| Diagnosis | Measurable acute ischemic stroke causing neurological deficit |
AHA/ASA Exclusion Criteria (Contraindications) - MUST MEMORIZE
| Absolute Contraindications | Why |
|---|
| Hemorrhagic stroke on CT | Adding tPA to existing bleeding = catastrophic |
| Prior intracranial hemorrhage | High risk of rebleeding |
| Active internal bleeding | Would worsen the bleeding |
| Severe uncontrolled hypertension (>185/110 mmHg) | Increases risk of hemorrhagic conversion |
| Intracranial surgery/trauma in past 3 months | Fresh surgical site would bleed |
| Recent (3 months) ischemic stroke or head trauma | |
| Platelet count <100,000 | Insufficient clot control after lysis |
| Blood glucose <50 or >400 mg/dL | Hypoglycemia mimics stroke; must be corrected first |
| Currently on anticoagulants with elevated INR (>1.7) | Already anticoagulated; adding tPA = bleeding |
Memory trick for contraindications: "BRAIN BLEED"
- Bleeding active
- Recent surgery (<3 months intracranial)
- Anticoagulants (INR >1.7, heparin with elevated aPTT)
- Intracranial hemorrhage (prior or current)
- Neuro deficit very mild or rapidly improving
- Blood pressure uncontrolled (>185/110)
- Low platelets (<100,000)
- Endocarditis (infective)
- Elevated glucose (<50 or >400)
- Duration unknown ("wake-up stroke" - unless imaging confirms penumbra)
Adverse Effects of Thrombolytics
| Adverse Effect | Mechanism | Frequency | Management |
|---|
| Symptomatic intracranial hemorrhage | Clot lysis opens up reperfused vessel that then bleeds | ~6% | Stop tPA; neurosurgical consult |
| Systemic bleeding | tPA acts throughout the body, not just in brain | Common | Avoid unnecessary punctures |
| Orolingual angioedema | Mechanism unknown; associated with ACE inhibitor use | Rare (~1-5%) | Steroids, antihistamines |
| Reperfusion injury | Sudden return of blood to ischemic tissue → oxidative damage | Can occur | Supportive |
Why does orolingual angioedema occur with tPA? tPA activates plasmin, which cleaves complement proteins and can also increase bradykinin. In patients already on ACE inhibitors (which also raise bradykinin), this effect is compounded, causing swelling of the lips, tongue, and oropharynx.
DRUG CLASS 2: ANTIPLATELET DRUGS
Definition
Antiplatelet drugs prevent platelets (tiny blood cell fragments) from clumping together to form clots.
Simple Analogy
Platelets are like tiny Velcro balls floating in blood. When a vessel is damaged, they stick to each other and to the vessel wall, forming a clot. Antiplatelet drugs are like covering those Velcro balls with a smooth coating so they can no longer stick together.
Why are they used in stroke?
In ischemic stroke caused by atherosclerosis or small vessel disease, platelets play a central role in forming the clot. Antiplatelet drugs are the cornerstone of:
- Acute ischemic stroke treatment (when tPA is not given)
- Secondary prevention (preventing future strokes)
- TIA (Transient Ischemic Attack) management
ASPIRIN (Acetylsalicylic Acid)
Mechanism:
Normal: COX-1 enzyme in platelets → Thromboxane A2 (TXA2) produced
TXA2 → Causes platelet aggregation + vasoconstriction
Aspirin → Irreversibly acetylates COX-1 → Permanently inactivates it
→ No TXA2 produced → Platelets cannot aggregate
Key point: Platelets cannot make new COX-1 (they have no nucleus). So one dose of aspirin disables a platelet for its ENTIRE lifespan (7-10 days).
Doses in stroke:
- Acute ischemic stroke: 160-325 mg orally within 24-48 hours of onset (if tPA not given - must wait 24 hours after tPA)
- Secondary prevention: 75-100 mg daily (low dose - still blocks COX-1 irreversibly but with fewer GI side effects)
Adverse effects:
- GI bleeding/ulceration (reduce COX-1 in stomach = loss of protective mucus)
- Tinnitus at high doses
- Hypersensitivity (aspirin-exacerbated respiratory disease)
- Reye's syndrome in children (avoid in <16 years)
CLOPIDOGREL
Mechanism:
Normal: Platelets have ADP receptors (P2Y12 receptors)
ADP binds P2Y12 → Triggers platelet activation and aggregation
Clopidogrel → Pro-drug, activated by liver CYP2C19
Active metabolite → Irreversibly blocks P2Y12 receptor
→ ADP cannot activate platelets → No aggregation
Clinical uses in stroke:
- Alternative to aspirin in aspirin-intolerant patients
- Dual antiplatelet therapy (DAPT): Aspirin + clopidogrel for 21-90 days after minor ischemic stroke or high-risk TIA (based on POINT and CHANCE trials)
- Long-term secondary prevention
Important interactions:
- CYP2C19 inhibitors (omeprazole, fluoxetine) reduce activation → Reduced effect
- PPIs: Clinical significance debated, but pantoprazole preferred over omeprazole
Adverse effects:
- Bleeding (most important)
- Thrombotic thrombocytopenic purpura (TTP) - rare but severe
- Rash, diarrhea
DIPYRIDAMOLE
Mechanism:
Inhibits phosphodiesterase (PDE) → More cAMP in platelets
More cAMP → Inhibits platelet aggregation
ALSO blocks adenosine uptake → More adenosine → Vasodilation
Clinical use: Usually combined with aspirin (Aggrenox = aspirin 25mg + modified-release dipyridamole 200mg). Used for secondary prevention of stroke/TIA.
Adverse effects: Headache (most common, due to vasodilation), flushing, dizziness, GI upset
TICAGRELOR
Mechanism: Reversibly blocks P2Y12 receptor (unlike clopidogrel which is irreversible). Does NOT require metabolic activation. Has more rapid onset.
Clinical use: Sometimes used with aspirin for high-risk TIA or minor stroke (THALES trial evidence). Twice-daily dosing required (due to reversible binding).
DRUG CLASS 3: ANTICOAGULANTS (for stroke prevention in atrial fibrillation)
Why atrial fibrillation (AF) causes stroke
In AF, the upper chambers of the heart quiver chaotically instead of beating regularly. Blood pools and stagnates in a pouch called the left atrial appendage (LAA). Stagnant blood forms clots. These clots can break off and travel to the brain, causing a cardioembolic stroke - typically large and devastating.
Anticoagulants are used to PREVENT this type of stroke. They do NOT treat acute stroke but are vital for long-term prevention.
WARFARIN
Mechanism:
Factors II, VII, IX, X (clotting factors) require Vitamin K for activation
Vitamin K → Carboxylation of clotting factors → They become functional
Warfarin → Inhibits Vitamin K epoxide reductase
→ Vitamin K cannot be recycled
→ Clotting factors cannot be carboxylated
→ Coagulation cascade blocked
Monitoring: INR (target 2.0-3.0 in AF)
Onset: Delayed 2-3 days (must deplete existing clotting factors)
Half-life: ~40 hours
Interactions (extensive):
- Inhibitors (raise INR - increased bleeding): amiodarone, fluconazole, metronidazole, statins
- Inducers (lower INR - increased clotting): rifampicin, carbamazepine, St. John's Wort
- Vitamin K in diet lowers INR
Reversal: Fresh frozen plasma (immediate) + Vitamin K (slower)
DIRECT ORAL ANTICOAGULANTS (DOACs)
These are newer drugs that directly block specific clotting factors. They have largely replaced warfarin for stroke prevention in non-valvular AF because they:
- Do not require regular monitoring
- Have fewer drug and food interactions
- Have fixed dosing
- Have similar or better efficacy and safety compared to warfarin
| Drug | Target | Dose (in AF) | Key Feature |
|---|
| Dabigatran | Factor IIa (thrombin) - DIRECT THROMBIN INHIBITOR | 150 mg twice daily | Only DOAC with specific antidote: Idarucizumab |
| Rivaroxaban | Factor Xa | 20 mg once daily | Once daily dosing |
| Apixaban | Factor Xa | 5 mg twice daily | Least renal clearance; preferred in CKD |
| Edoxaban | Factor Xa | 60 mg once daily | Once daily |
Reversal agent for Factor Xa inhibitors: Andexanet alfa
DRUG CLASS 4: ANTIHYPERTENSIVES IN STROKE
In acute stroke - a counterintuitive approach
In acute ischemic stroke, you generally do NOT aggressively lower blood pressure.
Why? In a stroke, the autoregulation of cerebral blood flow is disrupted. The brain becomes "pressure-passive" - blood flow to the penumbra depends directly on the blood pressure. Lowering blood pressure too aggressively can starve the penumbra of blood, converting it from potentially salvageable tissue to infarcted tissue.
Guidelines:
- If patient is receiving tPA: Lower BP to <185/110 mmHg BEFORE giving tPA, then maintain <180/105 mmHg after
- If NOT receiving tPA: Generally allow BP up to 220/120 mmHg for the first 24-48 hours. Only treat if BP exceeds this, or if there is end-organ damage
In hemorrhagic stroke: More aggressive BP lowering is appropriate (target systolic ~140 mmHg) to reduce ongoing bleeding.
For long-term secondary prevention (after any stroke): Aggressive BP control is the single most effective intervention. Agents used include ACE inhibitors (perindopril) + diuretics (indapamide) - based on the PROGRESS trial.
DRUG CLASS 5: STATINS in Stroke
Definition and mechanism
Statins (HMG-CoA reductase inhibitors) lower LDL cholesterol, but their benefits in stroke extend beyond cholesterol lowering (pleiotropic effects: anti-inflammatory, stabilize plaques, improve endothelial function).
Key drug: Atorvastatin 80 mg - High-intensity statin after ischemic stroke (SPARCL trial)
Contraindication: Do NOT use in hemorrhagic stroke - high-intensity statins may slightly increase the risk of hemorrhagic stroke recurrence.
DRUG CLASS 6: NEUROPROTECTION
The sad truth: Despite decades of research, NO neuroprotective drug has yet proven effective in human stroke trials. Hundreds of drugs that protected brain cells in animal studies have failed in human trials.
Current management focuses on:
- Restoring blood flow (thrombolysis, thrombectomy)
- Controlling glucose (both hypo- and hyperglycemia worsen outcomes)
- Controlling fever (fever increases metabolic demand on ischemic brain)
- Managing blood pressure appropriately
STROKE SECONDARY PREVENTION SUMMARY TABLE
| Stroke Type | First-Line Prevention |
|---|
| Large artery atherosclerosis | Antiplatelet (aspirin or clopidogrel) + High-dose statin + BP control |
| Cardioembolic (AF) | Anticoagulation (DOAC preferred over warfarin) |
| Small vessel (lacunar) | Antiplatelet + BP control |
| Cryptogenic stroke | Antiplatelet; investigate for PFO |
| After minor stroke/TIA | DAPT (aspirin + clopidogrel) for 21-90 days, then monotherapy |
PART B: HEADACHE AND MIGRAINE - DRUG TREATMENT
SECTION 1: BIG PICTURE OVERVIEW - MIGRAINE
What problem does migraine drug treatment solve?
A migraine is not just a bad headache. It is a complex neurological disorder that causes severe, debilitating, often one-sided head pain with nausea, vomiting, and extreme sensitivity to light and sound. The person cannot function.
At its root, a migraine is a problem of the trigeminal nerve and blood vessels of the brain acting abnormally - causing inflammation and pain signals that are overwhelming in their intensity.
Drug treatment of migraine aims to solve two separate problems:
- Stop the attack that is already happening (acute/abortive treatment)
- Prevent future attacks from happening (prophylactic treatment)
SECTION 2: BUILD THE FOUNDATION - MIGRAINE
What is a migraine? Let's build the complete picture.
Types of headache - brief overview
| Type | Key Feature |
|---|
| Tension-type (most common) | Bilateral, pressing/tightening band-like pain; mild-moderate; no nausea |
| Migraine | Unilateral, pulsating, moderate-severe; nausea/vomiting; photophobia/phonophobia |
| Cluster headache | Unilateral, severe, periorbital; autonomic features (tearing, rhinorrhea); occurs in clusters |
| Medication overuse headache | Daily headache from overuse of analgesics |
The phases of a migraine attack
A classic migraine with aura has 4 phases:
PHASE 1: PRODROME (hours to days before)
"Warning phase" - mood changes, fatigue, food cravings, yawning
↓
PHASE 2: AURA (20-60 minutes, in ~30% of migraineurs)
Visual: Zigzag lines (fortification spectra), scotoma (blind spots)
Sensory: Tingling, numbness
Speech: Aphasia
These represent cortical spreading depression (see below)
↓
PHASE 3: HEADACHE (4-72 hours)
Unilateral, pulsating, moderate-severe
Worsened by activity
Nausea, vomiting, photophobia, phonophobia
↓
PHASE 4: POSTDROME ("migraine hangover")
Fatigue, difficulty concentrating, mood changes
The Pathophysiology of Migraine - Step by Step
This is the key to understanding WHY each drug works.
1. Cortical Spreading Depression (CSD) - explains the aura
Trigger (stress, hormones, certain foods, sleep changes)
↓
Wave of intense neuronal firing sweeps slowly across the cortex
↓
Followed by a wave of suppressed neuronal activity
This wave travels at ~3-5 mm/min
↓
As the wave crosses visual cortex → Visual aura (zigzag lines, scotomas)
As it crosses sensory cortex → Tingling, numbness
↓
CSD triggers activation of the trigeminal nerve
2. Trigeminovascular Activation - explains the headache
This is the most important pathway for drug therapy:
CSD (or direct trigger) activates the TRIGEMINAL NERVE (cranial nerve V)
↓
Trigeminal nerve fibers surround intracranial blood vessels
↓
Activated trigeminal nerve RELEASES neuropeptides:
- CGRP (Calcitonin Gene-Related Peptide) ← KEY TARGET FOR NEW DRUGS
- Substance P
- Neurokinin A
↓
These neuropeptides cause:
1. VASODILATION of intracranial blood vessels (why pain is pulsating)
2. NEUROGENIC INFLAMMATION of the vessel walls
3. Pain signals sent via trigeminal ganglion → THALAMUS → CORTEX
↓
Brain perceives PAIN
↓
Central sensitization develops:
Trigeminal nucleus becomes hypersensitive
Explains allodynia (even brushing hair causes pain)
The role of serotonin (5-HT)
During aura: Platelet serotonin (5-HT) is released
↓
Blood serotonin RISES → Vasoconstriction (explains aura)
↓
Serotonin is metabolized rapidly
↓
Blood serotonin FALLS → Vasodilation (explains headache phase)
This is why serotonin agonists (triptans) work: By activating 5-HT receptors, they mimic the high-serotonin state, causing vasoconstriction and stopping the headache.
SECTION 3: DRUG CLASS FRAMEWORK - MIGRAINE
ACUTE (ABORTIVE) TREATMENT
The goal is to STOP the attack that is currently happening.
DRUG CLASS 1: TRIPTANS (5-HT1B/1D Agonists)
The most important class for acute migraine - FIRST LINE for moderate-severe attacks
Definition
Triptans are selective serotonin receptor agonists that act on 5-HT1B and 5-HT1D receptors (and to some extent 5-HT1F receptors) to abort migraine attacks.
Simple Analogy
Imagine the trigeminal nerve as a fire hose spraying inflammatory chemicals all over the brain's blood vessels, causing pain. Triptans are like turning off the tap - they switch off the trigeminal nerve and constrict the dilated vessels, stopping the spray.
Mechanism of Action - Complete Explanation
Triptans → Agonists at 5-HT1B receptors on cranial blood vessels
→ Vasoconstriction of dilated intracranial vessels
→ Less pulsation = less pain
Triptans → Agonists at 5-HT1D receptors on trigeminal nerve terminals
→ INHIBIT release of CGRP, Substance P, and other neuropeptides
→ Less neurogenic inflammation
→ Pain signals blocked at source
COMBINED EFFECT:
1. Constrict dilated blood vessels → Stop pulsating pain
2. Block inflammatory neuropeptide release → Reduce inflammation
3. Block pain signal transmission → Reduce perception of pain
The Individual Triptans
| Drug | Route | Onset | Half-life | Special Feature |
|---|
| Sumatriptan (prototype) | SC, Oral, Nasal | SC: 20 min; Oral: 1-2 hr | 2 hours | First triptan; SC fastest onset |
| Zolmitriptan | Oral, Nasal | 30-60 min | 2-3 hr | Good for nausea-dominant attacks (nasal/oral) |
| Rizatriptan | Oral | 30-60 min | 2-3 hr | Rapid onset oral |
| Naratriptan | Oral | 1-3 hr | 6 hr | Slower onset, lower recurrence; well tolerated |
| Almotriptan | Oral | 1-2 hr | 3-4 hr | Fewer chest symptoms |
| Eletriptan | Oral | 1-2 hr | 4-5 hr | Higher potency, longer duration |
| Frovatriptan | Oral | 2-4 hr | >24 hours | LONGEST half-life; used in menstrual migraine prophylaxis |
Exam pearl: Frovatriptan has the longest half-life among triptans (>24 hours). Sumatriptan was the FIRST triptan. SC sumatriptan has the FASTEST onset (~20 minutes).
Clinical Use
- When to give: At onset of headache (NOT during aura - wait for headache to begin)
- Efficacy: 70% of patients respond; abort or significantly reduce severity
- If first dose fails: Can try again after 2 hours OR try a different triptan (individual responses vary)
- Recurrence: Headache returns in 24-48 hours in many patients. Second dose usually effective.
Adverse Effects
| Effect | Mechanism |
|---|
| Chest tightness/pressure ("triptan sensations") | 5-HT1B-mediated coronary vasoconstriction |
| Neck/jaw pressure, paresthesias | Peripheral vasoconstriction |
| Elevation of blood pressure | Vasoconstriction |
| Dizziness, malaise | CNS effects |
Contraindications - CRITICAL
| Contraindication | Why |
|---|
| Coronary artery disease / angina | Triptans can cause coronary vasospasm → MI |
| Uncontrolled hypertension | Additional pressor effect |
| History of stroke or TIA | Vasoconstriction risk in already-compromised vessels |
| Hemiplegic or basilar migraine | Risk of worsening neurological deficit |
| Peripheral vascular disease | Vasoconstriction already compromised circulation |
| Ergot use within 24 hours | Combined vasospasm → life-threatening ischemia |
| MAO inhibitors within 2 weeks | Serotonin syndrome; also reduces triptan metabolism |
| Pregnancy | Insufficient safety data (sumatriptan most data) |
Drug Interactions
- MAO inhibitors (especially phenelzine, moclobemide): MAO metabolizes sumatriptan. MAOIs → reduced metabolism → sumatriptan toxicity. Contraindicated within 2 weeks.
- Ergot alkaloids: Combined vasospasm
- SSRIs/SNRIs: Theoretically serotonin syndrome (mild, but monitor)
- Lithium: Potential serotonin syndrome
DRUG CLASS 2: ERGOT ALKALOIDS
Origin and Definition
Ergot alkaloids come from the fungus Claviceps purpurea that grows on rye grains. They have complex pharmacology: partial agonist/antagonist activity at 5-HT, alpha-adrenergic, and dopamine receptors.
Simple Analogy
Ergot alkaloids are like an "old, imprecise Swiss Army knife" - they do a lot of things, some helpful (constrict the right vessels), some harmful (constrict too many vessels). Triptans are a "precision surgical tool" that does one job well.
Drugs
| Drug | Route | Notes |
|---|
| Ergotamine tartrate | Sublingual, oral (+caffeine), suppository | Used early in attack; oral with caffeine improves absorption |
| Dihydroergotamine (DHE) | IV, IM, Intranasal | Efficacy similar to sumatriptan; used for severe/refractory migraine |
Mechanism
5-HT1 receptor agonism → Vasoconstriction of intracranial vessels (primary)
Alpha-adrenergic agonism → Peripheral vasoconstriction (cause of side effects)
Dopamine receptor effects → Nausea/vomiting
Why caffeine is combined with ergotamine: Caffeine increases GI absorption of ergotamine by ~30%, causing faster onset. Caffeine itself is a mild cerebral vasoconstrictor.
Adverse Effects
| Effect | Mechanism |
|---|
| Nausea, vomiting | Dopamine receptor activation |
| Peripheral vasoconstriction | Alpha-adrenergic agonism |
| Ergotism (rare, chronic use): gangrene of fingers/toes | Severe peripheral vasospasm |
| Medication overuse headache (MOH) | Dependence with daily use |
| Retroperitoneal/pleuropulmonary fibrosis (with methysergide - historical) | 5-HT2 agonism causing fibrosis |
Contraindications
- Pregnancy (oxytocic effect → uterine contractions → fetal harm)
- Angina, CAD, uncontrolled hypertension
- Peripheral vascular disease
- Severe hepatic/renal impairment
- Within 24 hours of triptans
- Hemiplegic/basilar migraine
Note: The European Medicines Agency has recommended ergot derivatives no longer be used to treat migraine due to their unfavorable side effect profile. They have largely been replaced by triptans.
DRUG CLASS 3: DITANS (5-HT1F Agonists)
Definition
Ditans are a new class of selective 5-HT1F receptor agonists that treat acute migraine WITHOUT causing vasoconstriction.
Drug: Lasmiditan
Mechanism:
5-HT1F receptors are present on trigeminal nerve terminals
Activation → Inhibits release of inflammatory neuropeptides
→ Reduces pain signal transmission
KEY DIFFERENCE FROM TRIPTANS:
5-HT1F receptors are NOT present on blood vessels
Therefore: NO vasoconstriction → Safe in cardiovascular disease
Clinical use: Acute migraine in patients who CANNOT take triptans due to cardiovascular contraindications.
Adverse effects:
- Dizziness, somnolence (most common - crosses blood-brain barrier more than triptans)
- Driving impairment - patients must NOT drive for 8 hours after taking lasmiditan
- Potential for abuse (classified as Schedule V controlled substance)
DRUG CLASS 4: CGRP RECEPTOR ANTAGONISTS (Gepants)
The newest and most exciting class - explain CGRP first
CGRP = Calcitonin Gene-Related Peptide
- A neuropeptide released from trigeminal nerve terminals during migraine
- Causes marked vasodilation and neurogenic inflammation
- CGRP levels are elevated during acute migraine attacks
- CGRP is the most potent vasodilator in the brain
The problem with triptans: They constrict blood vessels by activating 5-HT receptors. This is effective but potentially dangerous in CAD patients.
The beauty of gepants: They block CGRP receptors WITHOUT causing vasoconstriction. They block the inflammation without constricting anything.
Migraine attack → Trigeminal nerve releases CGRP
↓
CGRP binds to CGRP receptors on vessel walls and neurons
↓
Gepant blocks this binding
↓
No vasodilation, no neurogenic inflammation
→ No/less migraine pain
Acute Gepants
| Drug | Use | Notes |
|---|
| Ubrogepant | Acute migraine | CYP3A4 substrate; contraindicated with strong CYP3A4 inhibitors |
| Rimegepant | Acute AND prevention | Unique dual indication |
Preventive Gepants
| Drug | Use | Notes |
|---|
| Rimegepant | Prevention (every other day) + acute | |
| Atogepant | Prevention (daily oral) | No acute use |
Adverse effects: Nausea, somnolence - low incidence. No cardiovascular concerns.
Safe in cardiovascular disease - a major advantage over triptans.
DRUG CLASS 5: ANALGESICS (Non-Specific)
For mild-moderate attacks or as adjuncts
| Drug | Dose | Notes |
|---|
| Aspirin | 900-1000 mg | First-line for mild migraine; cheap, effective |
| Ibuprofen | 400-600 mg | Effective, well-tolerated |
| Naproxen | 500-1000 mg | Available in combination with sumatriptan (Treximet) |
| Diclofenac potassium | 50 mg | Fast-dissolving formulation; fast onset |
| Acetaminophen/Paracetamol | 1000 mg | Less effective as monotherapy for migraine |
IMPORTANT WARNING: Medication Overuse Headache (MOH)
- Using analgesics, triptans, or ergots MORE than 10-15 days per month
- Leads to a chronic daily headache that is WORSE than the original migraine
- The treatment becomes the cause of headache
- Treatment: Gradually withdraw the offending drug (withdrawal headache initially worsens before improving)
- Sometimes called "rebound headache"
DRUG CLASS 6: ANTIEMETICS
Nausea and vomiting are major components of migraine AND also impair oral drug absorption (gastric stasis in migraine means tablets sit in stomach unabsorbed).
| Drug | Mechanism | Role |
|---|
| Prochlorperazine | D2 antagonist | Antiemetic + analgesic effect; can abort migraine |
| Metoclopramide | D2 antagonist + prokinetic | Antiemetic + improves gastric motility → Better drug absorption |
| Domperidone | D2 antagonist (peripheral) | Antiemetic; does not cross BBB; fewer CNS effects |
| Ondansetron | 5-HT3 antagonist | Less evidence for migraine specifically |
Metoclopramide is useful in migraine not only for nausea but also because it enhances gastric emptying, improving absorption of co-administered oral drugs (aspirin, triptans).
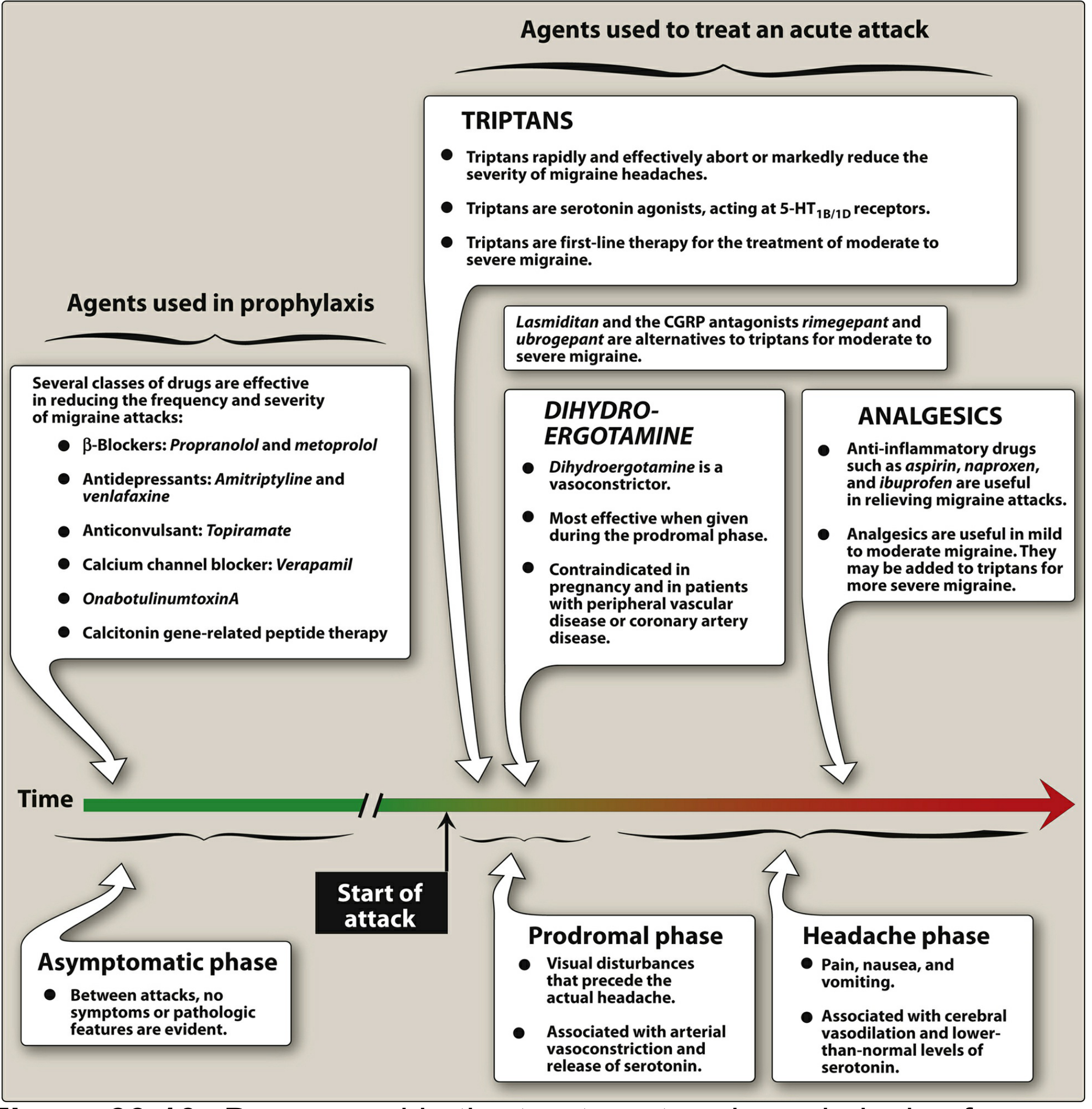
MIGRAINE FLOWCHART FROM LIPPINCOTT
Figure: Drugs used in the treatment and prophylaxis of migraine (Lippincott Illustrated Reviews: Pharmacology)
ACUTE MIGRAINE TREATMENT STRATEGY
ASSESS SEVERITY
MILD-MODERATE attack:
→ NSAIDs (ibuprofen 400-600 mg or aspirin 900 mg) ± antiemetic
→ If inadequate response: Move to triptans
MODERATE-SEVERE attack:
→ Triptan (oral, nasal, or SC sumatriptan) = FIRST LINE
If cardiovascular contraindications:
→ Lasmiditan (ditan) or Gepant (rimegepant/ubrogepant)
REFRACTORY/STATUS MIGRAINOSUS (>72 hours):
→ DHE (dihydroergotamine) IV
→ Prochlorperazine/Metoclopramide IV
→ Ketorolac IV
→ Steroids (dexamethasone IV) to prevent recurrence
→ Valproate IV
→ IV fluids
WITH NAUSEA/VOMITING:
→ Add antiemetic (metoclopramide or prochlorperazine)
→ Consider non-oral triptan (SC or nasal)
PROPHYLACTIC (PREVENTIVE) TREATMENT OF MIGRAINE
When to use prophylaxis?
Indicators for preventive therapy:
- ≥2 migraine attacks per month significantly impairing quality of life
- Attacks lasting >48 hours
- Acute medications failing or overused
- Hemiplegic, basilar, or prolonged aura migraine
- Patient preference
Target: Reduce frequency by ≥50% and reduce severity
PREVENTIVE DRUG CLASS 1: BETA-BLOCKERS
Drugs: Propranolol (most evidence), Metoprolol, Atenolol, Nadolol
Mechanism (not fully established):
Block beta-adrenergic receptors
→ Reduce vasomotor reactivity (stabilize blood vessel tone)
→ Modulate cortical excitability
→ Reduce adrenergic activation of migraine triggers
→ Possible interaction with serotonin receptors
Propranolol: 40-160 mg/day in divided doses. First-line preventive agent.
Contraindications: Asthma, heart block, severe bradycardia, peripheral vascular disease, depression (propranolol crosses BBB - can worsen depression).
PREVENTIVE DRUG CLASS 2: ANTIEPILEPTICS (Anticonvulsants)
Drugs: Topiramate, Valproate (Divalproex sodium)
Topiramate
Mechanism:
- Blocks voltage-gated sodium channels
- Enhances GABA activity (inhibitory neurotransmitter)
- Blocks kainate/AMPA glutamate receptors (reduces cortical excitability)
- Reduces CSD
Dose: 25-100 mg/day
Unique adverse effect: Weight loss (useful in obese migraineurs), cognitive slowing ("dopamax"), kidney stones (carbonic anhydrase inhibition), oligohydrosis
CONTRAINDICATED IN PREGNANCY - teratogenic (cleft palate)
Valproate/Divalproex
Mechanism:
- Enhances GABA activity
- Stabilizes voltage-gated sodium channels
- Reduces glutamate excitability
- Inhibits CSD
Dose: 500-1500 mg/day
Adverse effects: Weight gain, hair loss, tremor, teratogen (neural tube defects)
CONTRAINDICATED IN PREGNANCY
PREVENTIVE DRUG CLASS 3: ANTIDEPRESSANTS
Drugs: Amitriptyline (first-line), Venlafaxine
Amitriptyline (TCA - Tricyclic Antidepressant)
Mechanism in migraine prevention:
- Blocks reuptake of serotonin AND norepinephrine
- Also blocks histamine H1 receptors
- Downregulates 5-HT receptors with chronic use
- Independent of antidepressant effect (works at lower doses for migraine)
Dose for migraine: 10-75 mg at bedtime (much lower than antidepressant doses)
Adverse effects: Sedation (use at bedtime), anticholinergic (dry mouth, constipation, urinary retention), weight gain, QTc prolongation
Venlafaxine (SNRI)
- Better tolerated than amitriptyline
- Fewer anticholinergic effects
- Effective for both migraine AND comorbid depression/anxiety
PREVENTIVE DRUG CLASS 4: CALCIUM CHANNEL BLOCKERS
Drug: Verapamil
Use: Primarily for cluster headache prevention; also migraine.
Mechanism: Reduces neuronal excitability by blocking calcium-dependent processes; reduces vasomotor instability.
Adverse effects: Constipation, bradycardia, AV block, edema.
PREVENTIVE DRUG CLASS 5: ANTI-CGRP MONOCLONAL ANTIBODIES
The most exciting advance in migraine prevention in decades
These are monthly (or quarterly) injectable antibodies that target either:
- CGRP itself (the neuropeptide)
- The CGRP receptor
Fremanezumab } Target CGRP itself → prevent it from binding to receptor
Galcanezumab }
Eptinezumab }
Erenumab → Targets CGRP RECEPTOR → blocks CGRP from binding
| Drug | Target | Dosing |
|---|
| Erenumab | CGRP receptor | Monthly SC injection |
| Galcanezumab | CGRP ligand | Monthly SC injection |
| Fremanezumab | CGRP ligand | Monthly or quarterly SC injection |
| Eptinezumab | CGRP ligand | Quarterly IV infusion |
Why are these revolutionary?
- Specifically designed for migraine (not repurposed from another condition)
- Excellent safety profile (no hepatotoxicity, no CNS effects)
- Once monthly or quarterly dosing
- 50-75% of patients achieve ≥50% reduction in migraine days
Adverse effects: Injection site reactions, constipation (erenumab), nasopharyngitis. No major organ toxicity.
PREVENTIVE DRUG CLASS 6: ONABOTULINUMTOXIN A (BOTOX)
Use: FDA-approved specifically for chronic migraine (≥15 headache days/month, of which ≥8 are migraine)
Mechanism:
Botulinum toxin type A → Injected into multiple head and neck muscles
→ Cleaves SNAP-25 protein in nerve terminals
→ Prevents vesicle fusion
→ Blocks release of acetylcholine AND neuropeptides including CGRP
→ Reduces peripheral sensitization of trigeminal nerve
→ Reduces migraine frequency
Dose: 155-195 units injected across 31-39 sites every 12 weeks
Not for episodic migraine
MIGRAINE PREVENTION - COMPARISON TABLE
| Drug | Mechanism | Evidence | Side Effects | When to Choose |
|---|
| Propranolol | Beta-blocker | Best evidence | Fatigue, bradycardia, depression | First-line; hypertension comorbidity |
| Topiramate | Anticonvulsant | Strong | Cognitive, weight loss, stones | Useful if weight is a concern |
| Valproate | Anticonvulsant | Strong | Weight gain, teratogen | Not in women of childbearing age |
| Amitriptyline | TCA | Good | Sedation, anticholinergic | Insomnia or depression comorbidity |
| Venlafaxine | SNRI | Good | Nausea, hypertension | Depression/anxiety comorbidity |
| Verapamil | CCB | Moderate | Constipation, bradycardia | Cluster headache also |
| Anti-CGRP mAbs | CGRP antagonism | Excellent | Injection site reactions | Failed 2-3 preventives; high burden |
| OnabotulinumtoxinA | Prevents neuropeptide release | Strong | Injection pain, ptosis | Chronic migraine only |
CLUSTER HEADACHE - DRUG TREATMENT
Overview
Cluster headache: Severely painful, unilateral periorbital headache lasting 15 min-3 hours, with autonomic features (ipsilateral lacrimation, nasal congestion, ptosis, miosis). Occurs in "clusters" - multiple attacks per day for weeks to months, then remission.
Acute Treatment of Cluster Headache
| Treatment | Why it works | Notes |
|---|
| 100% Oxygen (7-15 L/min via non-rebreather for 15-20 min) | Vasoconstrictive + direct neuronal effect | First-line; no systemic side effects |
| Sumatriptan SC 6 mg | Triptan = fast vasoconstriction | Fastest onset via SC route; first-line drug |
| Zolmitriptan nasal spray | Triptan | Alternative to SC sumatriptan |
| DHE (dihydroergotamine) IN/IV | Vasoconstriction | For refractory attacks |
Prevention of Cluster Headache
| Drug | Mechanism | Notes |
|---|
| Verapamil (first-line) | CCB | 240-960 mg/day; monitor ECG |
| Lithium | Modulates circadian rhythms | For chronic cluster; requires monitoring |
| Oral/IV corticosteroids | Anti-inflammatory; breaks cluster | Short-term bridging until preventive works |
| Topiramate | CNS stabilization | Second-line |
| Melatonin | Circadian modulation | Adjunct |
TENSION-TYPE HEADACHE TREATMENT
Acute Treatment
| Drug | Notes |
|---|
| NSAIDs (ibuprofen 400-800 mg, aspirin 500-1000 mg) | First-line |
| Acetaminophen 1000 mg | First-line |
| Caffeine combinations | Enhance analgesic effect |
| Avoid opioids | Risk of MOH; ineffective for headache mechanisms |
Prevention of Tension Headache
| Drug | Notes |
|---|
| Amitriptyline | First-line preventive; 25-75 mg at night |
| Mirtazapine | Second-line |
| Venlafaxine | Second-line |
SECTION 4: TEACH USING ANALOGIES
Analogy Collection
1. The Triptan Analogy:
"Imagine the brain's blood vessels are pipes, and during a migraine, these pipes swell up and vibrate against each other, causing pain. Triptans are like a specialized plumber's tool that squeezes those pipes back to normal size AND plugs the leaking joints that are spraying inflammatory chemicals. Two actions, one drug."
2. CGRP and Gepants:
"CGRP is like a fire alarm that goes off in the brain during migraine, causing chaos (vasodilation, inflammation, pain). Triptans silence the alarm by constricting everything - but this risks damaging the pipes. Gepants are a smarter system that disconnects just the alarm wire, leaving the pipes untouched. Same silence, safer method."
3. Thrombolysis in Stroke:
"A stroke is like a river dam (blood clot) blocking the flow of water (blood) to a city (brain). tPA is like sending an emergency team with explosives to blast the dam open. You have a narrow time window - if you wait too long, the city's infrastructure (brain cells) is already too damaged to benefit from restored water supply."
4. Migraine Prophylaxis:
"Preventing migraine with propranolol is like turning down the volume on a speaker system. The music (migraine trigger) is still there, but the speaker (brain's sensitivity) is less reactive, so the music never reaches ear-splitting levels."
5. The Penumbra:
"After a stroke, there is a 'dead zone' in the centre of the stroke area, and around it a 'twilight zone' (penumbra) - tissue that is sick but alive. tPA is the treatment that can rescue the twilight zone. Every minute of delay means more twilight zone slides into the dead zone permanently."
6. Medication Overuse Headache:
"MOH is like borrowing money to pay off debt. You get short-term relief, but the interest (rebound headache) keeps growing until you're in deeper trouble than when you started."
7. Anticoagulation in AF for Stroke Prevention:
"In atrial fibrillation, the heart is like a washing machine spinning erratically. Clothes (blood clots) bunch up in corners. Anticoagulants are like a laundry additive that prevents clothes from bunching - but too much and they all fall apart (bleeding)."
SECTION 5: STEP-BY-STEP CLINICAL REASONING
Clinical Scenario 1: Acute Ischemic Stroke
Patient: 65-year-old man, sudden left-sided weakness + speech difficulty, 2.5 hours ago. BP 160/95. CT brain shows no hemorrhage.
Clinical Reasoning:
Q1: Is this ischemic or hemorrhagic?
CT brain = no hemorrhage → Ischemic stroke
Q2: Is thrombolysis indicated?
- Time window: 2.5 hours (within 4.5 hours) ✓
- CT = no hemorrhage ✓
- Neurological deficit present ✓
- BP = 160/95 - acceptable (need <185/110 before tPA) ✓
- No major contraindications described ✓
→ YES. Give IV alteplase.
Q3: Should we lower blood pressure first?
BP = 160/95. This is below the 185/110 threshold. No need to aggressively lower. Proceed with tPA.
Q4: Is there large vessel occlusion warranting thrombectomy?
Arrange CT angiography. If proximal MCA/ICA occlusion found → mechanical thrombectomy (preferably with tPA).
Q5: What happens after the acute phase?
- Antiplatelet (aspirin) started 24 hours after tPA
- Investigate for cause: ECG (AF?), echo, carotid doppler
- If AF found → anticoagulation (DOAC) for secondary prevention
- Statin therapy (atorvastatin 40-80 mg)
- Blood pressure management
- Physiotherapy, speech therapy, occupational therapy
Clinical Scenario 2: Acute Severe Migraine in ER
Patient: 32-year-old woman, severe right-sided pounding headache x 6 hours, nausea and vomiting, photophobia. Previous similar episodes. Currently cannot keep medications down.
Clinical Reasoning:
Q1: Is this migraine or something more dangerous?
- Sudden worst headache of life → Subarachnoid hemorrhage (do CT/LP)
- With fever + neck stiffness → Meningitis
- This patient has a previous history of similar attacks → Likely migraine but ALWAYS rule out emergency
Q2: She's vomiting - what route for medication?
Oral medications not appropriate. Need IV/IM/SC/intranasal route.
Q3: What treatments to give?
- IV/IM Metoclopramide (controls vomiting, enhances drug absorption, has mild analgesic effect)
- IV Ketorolac (parenteral NSAID - bypasses gut)
- SC or IM Sumatriptan (if no CV contraindications)
- IV fluids (if dehydrated)
- Dark, quiet room
Q4: If still refractory (>72 hours = status migrainosus)?
- IV Dexamethasone (reduces recurrence, breaks cycle)
- IV Valproate
- IV DHE (dihydroergotamine)
- Consider admission
Q5: What about prevention (she's having 3 attacks/month)?
- Consider preventive therapy
- Options: Propranolol (no asthma/bradycardia), topiramate, amitriptyline, anti-CGRP monoclonal antibody if previous preventives failed
- Discuss lifestyle triggers: sleep, hydration, stress
Clinical Scenario 3: Stroke Prevention in AF Patient
Patient: 72-year-old woman, non-valvular AF, BP controlled, CrCl 45 mL/min, no previous stroke.
Q1: Does she need anticoagulation?
CHA₂DS₂-VASc score: Age >75 (2), Female (1) = Score ≥2 → Anticoagulation indicated.
Q2: Warfarin or DOAC?
DOACs preferred. But CrCl = 45 mL/min (reduced renal function).
- Apixaban: 5 mg twice daily (least renal clearance, safest in CKD) - PREFERRED
- Dabigatran: 75 mg twice daily (if CrCl 15-30 mL/min; avoid if CrCl <15) - CAUTION
- Rivaroxaban: Reduce dose to 15 mg once daily with evening meal
Q3: She's on aspirin for "heart protection" - should she continue?
In AF, aspirin is INFERIOR to anticoagulation for stroke prevention and does NOT meaningfully protect against embolic stroke. Anticoagulation REPLACES aspirin in AF for stroke prevention. Adding aspirin to anticoagulation only increases bleeding risk.
SECTION 6: MEMORY TOOLS
MNEMONICS
1. Migraine Triptans - "SAFE NRZ" (7 Triptans)
- Sumatriptan (prototype, SC fastest)
- Almotriptan
- Frovatriptan (Furthest half-life - >24 hours)
- Eletriptan (Excellent potency)
- Naratriptan (Nice & slow onset, less recurrence)
- Rizatriptan (Rapid oral onset)
- Zolmitriptan (Zaps via nasal or oral)
2. Migraine Prophylaxis - "BACk to CALM"
- Beta-blockers (propranolol)
- Amitriptyline (TCA)
- Calcium channel blockers (verapamil)
- CGRP antibodies (erenumab, galcanezumab, fremanezumab, eptinezumab)
- Anticonvulsants (topiramate, valproate)
- Lasmiditan (actually acute, but remember for exams)
- Monoclonal antibodies (CGRP)
3. Triptan Contraindications - "CASH HUG"
- Coronary artery disease
- Angiospastic conditions
- Stroke/TIA history
- Hemiplegic/basilar migraine
- Hypertension (uncontrolled)
- Used ergots (<24 hours ago)
- Give no MAOIs (<2 weeks ago)
4. tPA Contraindications in Stroke - "BRAIN BLEED" (see Section 3 above)
5. Phases of Migraine - "PAHP" (Pain After Half a Phase)
- Prodrome
- Aura
- Headache
- Postdrome
6. DOACs for Stroke in AF - "DARE"
- Dabigatran (Direct thrombin inhibitor = Factor IIa)
- Apixaban (Anti-Xa, least renal)
- Rivaroxaban (anti-Xa, once daily)
- Edoxaban (anti-Xa, once daily)
7. Remember CGRP antibodies - "FREE Eggs"
- Fremanezumab (targets CGRP ligand)
- Eptinezumab (targets CGRP ligand)
- Erenumab (targets CGRP Receptor)
- (Gal)canezumab (Gal + "can" easy to remember as "targets CGRP can/ligand")
8. Why TRIPTANS work - "VIR"
- Vasoconstriction (5-HT1B on vessels)
- Inhibit neuropeptide release (5-HT1D on trigeminal terminals)
- Reduce pain transmission centrally
VISUAL MEMORY TRICKS
The Migraine Serotonin See-Saw
AURA PHASE HEADACHE PHASE
Serotonin HIGH ←────→ Serotonin LOW
Vasoconstriction Vasodilation
Visual symptoms Pulsating pain
TRIPTANS: Mimic HIGH serotonin → Vasoconstriction → Abort headache
The Stroke Time Chart
0 min ─────── 90 min ──────── 3 hr ────────── 4.5 hr ──────────→ Time
BEST window Good window Extended window (selected patients)
for tPA for tPA Brain imaging guided
"Every 30 minutes delay = 30% worse outcome"
tPA Dose Calculator Memory
tPA dose = 0.9 mg/kg (max 90 mg)
10% given as BOLUS over 1 minute
90% given as INFUSION over 60 minutes
Memory: "0.9/10/90" - 0.9 mg/kg, 10% bolus, 90% infusion over 60 min
COMPARISON TABLES
Triptan vs. Ergot vs. Ditan vs. Gepant
| Property | Triptan | Ergot | Ditan (Lasmiditan) | Gepant |
|---|
| Receptor | 5-HT1B/1D | 5-HT1, Alpha, Dopamine | 5-HT1F | CGRP receptor |
| Vasoconstriction | YES | YES (more) | NO | NO |
| CV safe? | Caution | Caution (more) | YES | YES |
| Controlled substance? | No | No | Yes (Schedule V) | No |
| Driving impairment | Minor | Minor | Significant (8 hrs) | No |
| Medication class | Specific | Specific | Specific | Specific |
Acute vs. Preventive Migraine Treatment
| Category | Goal | Timing | Examples |
|---|
| Acute (Abortive) | Stop current attack | During attack | Triptans, NSAIDs, Ergots, Gepants, Ditans |
| Prophylactic (Preventive) | Reduce future attacks | Daily, ongoing | Beta-blockers, anticonvulsants, TCAs, CGRP mAbs, Botox |
SECTION 7: EXAMINER'S CORNER
Most Tested Facts in Pharmacology Examinations
STROKE PHARMACOLOGY - HIGH YIELD
- tPA mechanism: Converts plasminogen → plasmin → fibrinolysis
- tPA time window: 4.5 hours (extended); standard 3 hours (NINDS trial)
- tPA dose: 0.9 mg/kg (max 90 mg); 10% bolus + 90% over 60 min
- tPA main risk: Symptomatic intracranial hemorrhage (~6%)
- BP threshold for tPA: Must be <185/110 before giving
- When to give aspirin after tPA: Wait 24 hours
- Aspirin in acute stroke: 160-325 mg (if no tPA)
- Clopidogrel mechanism: Irreversibly blocks P2Y12 (ADP receptor)
- DOACs vs. Warfarin in AF stroke prevention: DOACs preferred
- Dabigatran reversal: Idarucizumab (specific antidote)
- CGRP antibodies for stroke prevention: NOT used (they're for migraine)
- Why not lower BP in acute ischemic stroke: Loss of autoregulation; penumbra dependent on MAP
MIGRAINE PHARMACOLOGY - HIGH YIELD
- Triptans mechanism: 5-HT1B/1D agonists
- Sumatriptan: First triptan; fastest SC onset (20 min); t½ 2 hours
- Frovatriptan: Longest half-life (>24 hours) - used for menstrual migraine
- Triptan contraindications: CAD, uncontrolled HTN, hemiplegic migraine, prior stroke, pregnancy, MAOIs, ergots
- Ergot + triptan interaction: Both vasoconstrictors; wait 24 hours between them
- CGRP mechanism: Released from trigeminal nerve; causes vasodilation and neurogenic inflammation
- Gepants: CGRP receptor antagonists; no vasoconstriction; safe in CV disease
- Lasmiditan: 5-HT1F agonist; no vasoconstriction; causes driving impairment
- First-line migraine prevention: Propranolol (beta-blocker)
- Topiramate adverse effects: Cognitive slowing, weight loss, kidney stones, teratogen
- MOH (medication overuse headache): Caused by >10-15 days/month of acute medications
- Botox indication: Chronic migraine ONLY (≥15 headache days/month)
- Antiemetics in migraine: Metoclopramide (improves absorption + antiemetic)
- CGRP mAbs: Erenumab targets receptor; others target ligand
Most Likely Essay Questions
- "Describe the pharmacological management of acute ischemic stroke."
- "Classify drugs used in migraine. Describe the mechanism of action, clinical uses, and adverse effects of triptans."
- "Discuss the role of anticoagulants in stroke prevention. Compare DOACs with warfarin."
- "Write an essay on the drug treatment of migraine - both acute and prophylactic."
- "Describe the pathophysiology of migraine and explain how drugs act on these mechanisms."
Most Likely Short Notes
- Triptans
- CGRP antagonists in migraine
- Thrombolysis in stroke (tPA)
- Antiplatelet drugs in stroke
- Migraine prophylaxis
- Medication overuse headache
- Cluster headache management
- DOACs vs. warfarin
Most Likely Viva Questions
- "What is the mechanism of triptans? Why are they contraindicated in heart disease?"
- "A 70-year-old has a stroke - what is your immediate pharmacological management?"
- "What is CGRP and why is it important in migraine?"
- "Why can't you give aspirin immediately after tPA in stroke?"
- "Explain medication overuse headache."
- "What is the time window for thrombolysis and why?"
- "Which triptan has the longest half-life? Why is this clinically relevant?"
- "Why is clopidogrel used with aspirin after TIA? What is DAPT?"
Most Likely MCQs
- Drug of choice for acute severe migraine: Sumatriptan (SC)
- First triptan discovered: Sumatriptan
- Triptan with longest half-life: Frovatriptan
- Mechanism of triptans: 5-HT1B/1D agonists
- tPA time window (standard): 3 hours (NINDS); extended to 4.5 hours
- Reversal of dabigatran: Idarucizumab
- First-line migraine prophylaxis: Propranolol
- CGRP antibody targeting the receptor (not ligand): Erenumab
- Gepants mechanism: CGRP receptor antagonism
- Drug approved for chronic migraine prevention by injection: OnabotulinumtoxinA
- Most common adverse effect of triptans: Chest tightness/triptan sensations
- Antiemetic that ALSO improves gastric emptying in migraine: Metoclopramide
- Drug causing "driving impairment" as major side effect in migraine: Lasmiditan
- Which migraine preventive should NOT be used in pregnancy: Topiramate AND valproate
- BP target before giving tPA: <185/110 mmHg
Common Traps Students Fall Into
- "Give aspirin immediately after tPA" - WRONG. Wait 24 hours (increased hemorrhage risk)
- "Triptans can be given during aura" - PARTIALLY WRONG. SC triptans are ineffective during aura; wait for headache onset
- "All triptans are contraindicated in pregnancy" - Technically yes, but sumatriptan has most safety data; this is a nuanced point
- "Ergot + triptan can be given together" - WRONG. Dangerous vasospasm; need 24-hour gap
- "Warfarin is better than DOACs" - WRONG for non-valvular AF; DOACs are preferred
- "Lower blood pressure aggressively in acute ischemic stroke" - WRONG. Only if >220/120 or before tPA
- "Gepants cause vasoconstriction like triptans" - WRONG. Gepants block CGRP receptor; no vasoconstriction
- "All beta-blockers work for migraine" - Not all: Atenolol and metoprolol have some evidence; propranolol best evidence. Pindolol (partial agonist) does NOT work
- "Medication overuse headache only from opioids" - WRONG. NSAIDs, triptans, ergots all cause MOH if overused
- "Frovatriptan's long half-life makes it best for acute attacks" - Partially. Slow onset means it's not ideal for aborting attacks; mainly used for menstrual migraine prevention
SECTION 9: HIGH-YIELD REVISION SHEET
ONE-PAGE RAPID REVIEW: STROKE PHARMACOLOGY
ISCHEMIC STROKE - ACUTE:
━━━━━━━━━━━━━━━━━━━━━━━━
✓ tPA (Alteplase): 0.9 mg/kg, max 90 mg, within 4.5 hours
- 10% bolus + 90% over 60 min
- Main risk: Hemorrhagic transformation (6%)
- BP must be <185/110 before giving
- Wait 24 hours before aspirin
✓ Tenecteplase: Single bolus; higher fibrin specificity
✓ If tPA not given: Aspirin 160-325 mg within 24-48 hrs
SECONDARY PREVENTION:
━━━━━━━━━━━━━━━━━━━━━
✓ Aspirin 75-100 mg daily (antiplatelet)
✓ Clopidogrel (P2Y12 blocker) - alternative or combination
✓ DAPT (aspirin + clopidogrel x 21-90 days) after TIA/minor stroke
✓ Dipyridamole + aspirin (Aggrenox) - alternative
✓ Atorvastatin 80 mg (high-intensity statin)
✓ ACE inhibitor + diuretic for BP (PROGRESS trial)
✓ AF → DOAC (apixaban preferred in CKD)
HEMORRHAGIC STROKE:
━━━━━━━━━━━━━━━━━━━
✓ NO tPA, NO anticoagulation acutely
✓ Control BP (systolic target ~140)
✓ Reverse anticoagulation if on it
ONE-PAGE RAPID REVIEW: MIGRAINE PHARMACOLOGY
ACUTE MIGRAINE TREATMENT:
━━━━━━━━━━━━━━━━━━━━━━━━━
Mild-Moderate:
✓ NSAIDs (ibuprofen 400-600 mg, aspirin 900-1000 mg)
✓ Paracetamol 1000 mg
✓ + Metoclopramide (antiemetic + improves absorption)
Moderate-Severe (FIRST LINE):
✓ TRIPTANS: 5-HT1B/1D agonists
- Sumatriptan (SC fastest = 20 min; oral/nasal also available)
- 7 triptans: SAFE NRZ
- Frovatriptan = LONGEST t½ (>24 h)
- CONTRAINDICATED: CAD, uncontrolled HTN, stroke hx, hemiplegic migraine
If CV contraindication to triptans:
✓ Lasmiditan (5-HT1F; no vasoconstriction; driving impairment)
✓ Gepants: Rimegepant/Ubrogepant (CGRP receptor antagonists; no vasoconstriction)
Refractory:
✓ DHE IV/IN, Prochlorperazine IV, Ketorolac IV, Dexamethasone IV
AVOID: Ergot + triptan within 24 hours (vasospasm)
MIGRAINE PROPHYLAXIS (≥2 attacks/month):
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
First-line:
✓ Propranolol (beta-blocker): 40-160 mg/day
✓ Topiramate (anticonvulsant): 25-100 mg/day [CI: pregnancy]
✓ Amitriptyline (TCA): 10-75 mg at night
✓ Valproate: [CI: pregnancy, women of childbearing age]
Newer options:
✓ Anti-CGRP mAbs: Erenumab (vs. receptor), Galcanezumab/Fremanezumab/Eptinezumab (vs. ligand)
✓ Gepants: Atogepant (prevention), Rimegepant (prevention + acute)
✓ OnabotulinumtoxinA: ONLY for CHRONIC migraine
CLUSTER HEADACHE ACUTE:
━━━━━━━━━━━━━━━━━━━━━━━
✓ 100% O₂ 15 L/min (15-20 min)
✓ Sumatriptan SC 6 mg
Prevention: Verapamil (first-line)
KEY DRUG MECHANISMS:
━━━━━━━━━━━━━━━━━━━━
• Triptans → 5-HT1B/1D agonist → vasoconstrict + block CGRP/SP release
• Lasmiditan → 5-HT1F agonist → block pain, NO vasoconstriction
• Gepants → CGRP receptor block → no vasodilation, no inflammation
• CGRP mAbs → block CGRP ligand or receptor monthly/quarterly
• Ergots → 5-HT1 + alpha agonist → vasoconstrict (more side effects)
• Propranolol → reduces vasomotor reactivity + cortical excitability
• Topiramate → Na channel block + GABA enhancement + glutamate block
• Botox → blocks SNAP-25 → prevents neuropeptide release from nerve terminals
MUST-KNOW COMPARISONS:
━━━━━━━━━━━━━━━━━━━━━━
• First triptan: Sumatriptan
• Fastest onset triptan: Sumatriptan SC (20 min)
• Longest t½ triptan: Frovatriptan (>24 h)
• Triptan for menstrual migraine prevention: Frovatriptan
• Safe in CV disease: Lasmiditan, Gepants
• Causes driving impairment: Lasmiditan (8 hours)
• Controlled substance among anti-migraine: Lasmiditan (Schedule V)
• MOH: >10-15 days/month of acute meds → chronic daily headache
• Botox: ONLY chronic migraine (≥15 headache days/month)
SECTION 10: SELF-ASSESSMENT - 10 SHORT-ANSWER QUESTIONS
Q1. A 58-year-old man presents with acute left hemiplegia and aphasia, onset 2 hours ago. CT shows no hemorrhage. BP = 190/100 mmHg. Should tPA be given? If so, what must be done first?
Answer: Yes, tPA is indicated (ischemic stroke within 4.5-hour window). HOWEVER, BP must first be lowered to <185/110 mmHg before administering tPA (use IV labetalol or nicardipine). Once BP is controlled, give alteplase 0.9 mg/kg (max 90 mg) - 10% as IV bolus, remainder over 60 minutes. After tPA, maintain BP <180/105 mmHg. Do NOT give aspirin for at least 24 hours.
Q2. Explain why triptans are contraindicated in patients with coronary artery disease.
Answer: Triptans are 5-HT1B/1D receptor agonists. 5-HT1B receptors are present not only on intracranial blood vessels but also on coronary arteries. Activation of 5-HT1B receptors in coronary arteries causes vasoconstriction. In a patient with CAD, the coronary arteries are already narrowed by atherosclerosis. Triptan-induced coronary vasospasm can further reduce coronary blood flow, potentially causing angina, myocardial infarction, or arrhythmias. The chest tightness reported by migraine patients on triptans is partly due to this effect.
Q3. What is the mechanism of action of clopidogrel, and why does it require CYP2C19 for activity?
Answer: Clopidogrel is a prodrug that requires hepatic activation by the enzyme CYP2C19 to form its active metabolite. The active metabolite irreversibly blocks the P2Y12 (ADP) receptor on platelet surfaces. Normally, ADP binding to P2Y12 activates platelets and promotes aggregation. By irreversibly blocking this receptor, clopidogrel prevents ADP-mediated platelet activation for the entire lifespan of the platelet (7-10 days). Patients who are CYP2C19 poor metabolizers (genetic polymorphism) or who take CYP2C19 inhibitors (e.g., omeprazole) will have reduced activation of clopidogrel and therefore reduced antiplatelet effect.
Q4. What is CGRP, and what is its role in migraine pathophysiology?
Answer: CGRP (Calcitonin Gene-Related Peptide) is a neuropeptide released from the nerve terminals of the trigeminal nerve during a migraine attack. It is one of the most potent vasodilators in the brain. During migraine, activation of the trigeminovascular system causes release of CGRP, which binds to CGRP receptors on cranial blood vessel walls, causing marked vasodilation and neurogenic inflammation. This contributes to the pulsating, severe headache. CGRP levels are measurably elevated in blood/CSF during acute migraine. Blocking CGRP (gepants) or the CGRP receptor (erenumab) reduces migraine frequency and severity without causing vasoconstriction, making these agents safe in patients with cardiovascular disease.
Q5. A 35-year-old woman has 4 migraine attacks per month lasting 24-36 hours each, despite acute triptan use. She is trying to conceive. What prophylactic agent would you choose and why?
Answer: This patient needs prophylaxis (≥2 attacks/month with significant disability). However, she is trying to conceive, which eliminates several agents:
- Topiramate - teratogenic (cleft palate); AVOID
- Valproate - teratogenic (neural tube defects); AVOID
- Amitriptyline - relatively safer but use caution
- Best choice: Propranolol - beta-blocker; most evidence for migraine prevention; generally considered safest in pregnancy planning (though review if she becomes pregnant); no major teratogenic risk; dose 40-160 mg/day
Anti-CGRP antibodies are not recommended in pregnancy (insufficient data). Propranolol is the safest first-line preventive in a woman wishing to conceive.
Q6. Compare lasmiditan with sumatriptan - mechanism, advantages, and disadvantages.
Answer:
| Feature | Sumatriptan | Lasmiditan |
|---|
| Receptor | 5-HT1B/1D agonist | 5-HT1F agonist |
| Vasoconstriction | YES (cranial and coronary) | NO |
| CV safety | Contraindicated in CAD | Safe in CAD |
| BBB penetration | Low | High (more CNS effects) |
| CNS effects | Minimal | Significant: dizziness, somnolence |
| Driving | Minor impairment | Significant (do not drive for 8 hours) |
| Controlled substance | No | Yes (Schedule V) |
| Route | SC, oral, nasal | Oral only |
Advantage of lasmiditan: Safe in patients with cardiovascular contraindications to triptans.
Disadvantage: CNS effects, driving impairment, controlled substance status, oral only.
Q7. What is medication overuse headache (MOH)? How is it treated?
Answer: MOH (also called rebound headache or analgesic overuse headache) develops when acute headache medications are used excessively - typically >10 days/month for triptans, ergots, or opioids, or >15 days/month for simple analgesics (NSAIDs, paracetamol). The brain becomes sensitized to lack of medication and begins generating headaches to drive more drug-taking. This creates a cycle: headache → medication → relief → headache. The headache becomes chronic (>15 days/month) and loses the characteristics of the original primary headache type.
Treatment:
- Identify and withdraw the offending drug (ALL overused acute medications)
- Withdrawal causes a temporary worsening of headache (withdrawal headache) lasting 2-10 days
- Bridging therapy during withdrawal: Steroids (prednisone), naproxen (if not the overused drug), antiemetics
- Start prophylactic therapy to prevent return to frequent use
- Patient education about MOH - prevent recurrence
Q8. An elderly woman with non-valvular AF and CKD (CrCl 30 mL/min) needs stroke prevention. Which anticoagulant would you choose?
Answer: Apixaban is the preferred DOAC in this scenario. Among DOACs:
- Apixaban has the LEAST renal elimination (~27% renal clearance) - safest in CKD
- Rivaroxaban is 35% renally eliminated; dose reduction needed
- Dabigatran is ~80% renally eliminated - AVOID in severe CKD (CrCl <15 mL/min, caution 15-30)
- Edoxaban is 50% renally eliminated
Dose: Apixaban 5 mg twice daily (reduce to 2.5 mg twice daily if ≥2 of: age ≥80, weight ≤60 kg, creatinine ≥1.5 mg/dL). This patient: CrCl 30 suggests significant renal impairment - check whether dose reduction criteria are met. Warfarin remains an option with careful INR monitoring if DOACs are unavailable.
Q9. Why is aspirin given INSTEAD OF anticoagulants for secondary prevention in most non-cardioembolic strokes (atherosclerotic/lacunar)?
Answer: In strokes caused by large artery atherosclerosis or small vessel disease (lacunar), the primary mechanism is platelet-rich (white) clot formation at the site of atherosclerotic plaque. Antiplatelet drugs (aspirin, clopidogrel) are highly effective against platelet-driven thrombosis.
Anticoagulants (warfarin, DOACs) are designed primarily for fibrin-rich (red) clots, which form in conditions of blood stasis (atrial fibrillation, mechanical heart valves). In non-cardioembolic stroke:
- Anticoagulants do NOT provide additional benefit over antiplatelets
- Anticoagulants carry a significant risk of intracranial hemorrhage
- The WARSS trial showed warfarin was NOT superior to aspirin for non-cardioembolic stroke secondary prevention
Therefore: Anticoagulants are reserved for cardioembolic stroke (AF, mechanical valves), while antiplatelets are used for all other ischemic stroke types.
Q10. List the 4 anti-CGRP monoclonal antibodies used in migraine prevention. Which one targets the receptor (rather than the ligand)?
Answer:
| Drug | Target | Dosing |
|---|
| Erenumab | CGRP Receptor | Monthly SC |
| Galcanezumab | CGRP Ligand | Monthly SC |
| Fremanezumab | CGRP Ligand | Monthly or quarterly SC |
| Eptinezumab | CGRP Ligand | Quarterly IV |
Erenumab is the only anti-CGRP monoclonal antibody that targets the CGRP receptor. All others (galcanezumab, fremanezumab, eptinezumab) target the CGRP ligand (the CGRP peptide itself), preventing it from reaching the receptor.
Memory trick: Erenumab targets the Exit door (receptor). The others block the Key (ligand).
FINAL NOTE TO THE STUDENT
These three topics - stroke, headache, and migraine - test your ability to integrate pharmacology with pathophysiology and clinical reasoning. The examiner wants to see that you understand WHY each drug works, not just WHAT it does.
The most important themes to master are:
-
Stroke: The time-critical use of tPA, why you cannot lower BP aggressively, the distinction between antiplatelet and anticoagulant indications, and the DOACs.
-
Migraine: The trigeminovascular theory, the CGRP pathway, why triptans work (and why they're contraindicated in vascular disease), the new drug classes (ditans, gepants, CGRP mAbs), and the full range of preventive agents.
-
Integration: A patient with migraine AND heart disease needs a different treatment pathway than a healthy patient. A stroke patient ON anticoagulants needs different tPA considerations. These real-world integrations are what examiners test in essays and vivas.
Master the mechanisms, master the reasoning, and the facts will follow naturally.
Sources: Lippincott Illustrated Reviews: Pharmacology (pp. 1322-1324) | Adams and Victor's Principles of Neurology, 12th Ed. (pp. 820-821) | Goodman & Gilman's Pharmacological Basis of Therapeutics (p. 313) | Bradley and Daroff's Neurology in Clinical Practice | Tintinalli's Emergency Medicine
Recent evidence: Thrombolysis beyond 4.5 hours - meta-analysis (Stroke, 2025, PMID: 39882605); IV thrombolysis in minor stroke - meta-analysis (Neurology, 2025, PMID: 40674672)