Everything about dosage forms
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Searching the Web
pharmaceutical dosage forms classification types comprehensive overview
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the information needed for a comprehensive answer. Here is a thorough overview of dosage forms.
Dosage Forms — Complete Overview
A dosage form is the physical form in which a drug is manufactured and delivered to the patient. The choice of dosage form is determined by the drug's physicochemical properties (solubility, stability, molecular size), the desired route of administration, therapeutic goals (speed of onset, local vs. systemic effect), and patient factors (age, ability to swallow, adherence).
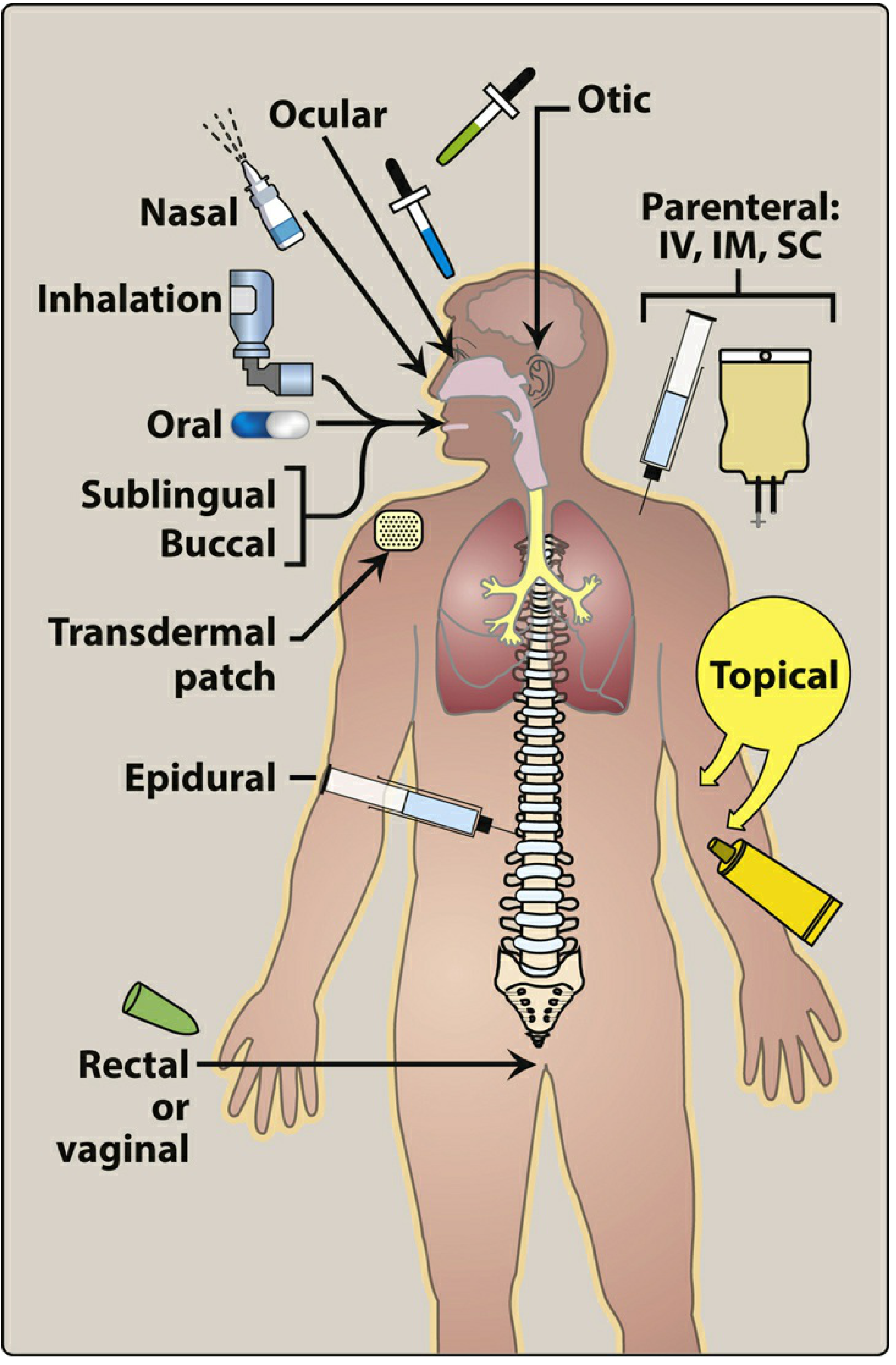
Classification of Dosage Forms
Dosage forms are broadly classified by the route of administration: enteral, parenteral, and topical/transdermal.
1. Enteral (via the GI tract)
A. Oral
The most common, convenient, and economical route. Oral preparations include:
| Form | Description | Key Features |
|---|---|---|
| Tablets | Compressed solid drug ± excipients | Easy to manufacture, stable, accurate dosing |
| Capsules | Drug enclosed in gelatin shell (hard or soft) | Masks taste/odor; can contain liquid fills |
| Enteric-coated tablets | Chemical coating that resists stomach acid | Protects acid-labile drugs (e.g., omeprazole); reduces gastric irritation (e.g., aspirin) |
| Extended-release (ER/XR/XL/SR/CR) | Special coatings or matrix controlling release | Slower absorption, prolonged action, fewer doses, reduced peaks and troughs; useful for short–half-life drugs (e.g., morphine ER → from 6× to 2× daily) |
| Chewable tablets | Designed to be chewed before swallowing | Useful in children and patients who cannot swallow |
| Effervescent tablets | Dissolve in water to form carbonated solution | Faster absorption, better palatability |
| Orally disintegrating tablets (ODT) | Dissolve on tongue without water | Useful in patients with dysphagia; improves adherence (e.g., risperidone ODT, olanzapine ODT) |
| Elixirs | Clear alcoholic solutions with dissolved drug | Drug uniformly distributed; no shaking required |
| Suspensions | Undissolved drug particles in liquid vehicle | Must be shaken thoroughly before each dose; uneven distribution → under/overdosing (clinical problem with phenytoin suspension) |
| Syrups | Concentrated aqueous sugar solution | Pleasant taste; useful in pediatrics |
| Emulsions | Oil-in-water or water-in-oil dispersions | For lipid-soluble drugs |
Oral route considerations:
- Subject to first-pass hepatic metabolism
- Low gastric pH inactivates some drugs
- Food can significantly affect absorption
- Patient compliance is essential
B. Sublingual / Buccal
- Sublingual: Drug placed under the tongue (e.g., nitroglycerin, buprenorphine)
- Buccal: Drug placed between the cheek and gum (e.g., asenapine sublingual tablets)
Advantages: Rapid absorption; bypasses first-pass metabolism; bypasses gastric pH inactivation; onset of action within minutes
Disadvantages: Limited to small doses; not suitable for all drugs; some drug may be inadvertently swallowed
C. Rectal
Forms: suppositories, enemas, foams
- ~50% of rectal venous drainage bypasses the portal circulation → reduces first-pass metabolism
- Useful when oral route is unavailable (vomiting, unconsciousness)
- Rectal absorption is often erratic and incomplete
- Many drugs irritate the rectal mucosa
- Clinical use: antiemetics (promethazine), antiepileptics (diazepam rectal gel), hydrocortisone enemas for ulcerative colitis
2. Parenteral (Injected — bypasses GI tract)
| Route | Abbreviation | Speed of Onset | Notes |
|---|---|---|---|
| Intravenous | IV | Immediate | 100% bioavailability; no absorption required; suitable for large volumes; can achieve immediate, precise blood levels |
| Intramuscular | IM | 10–30 min | Depot injections possible; bypasses GI and first-pass; most short-acting IM antipsychotics reach peak plasma level in 30–60 min with clinical effects within 15 min |
| Subcutaneous | SC/SQ | 15–30 min | Slower than IM; good for insulin, heparin, vaccines |
| Intrathecal / Intraventricular | IT | Rapid CNS effect | Bypasses blood-brain barrier; used when rapid CNS drug delivery is needed |
| Epidural | — | Minutes | Drug placed in epidural space (e.g., local anesthetics, opioids for pain) |
| Intra-articular | — | Local | Used for joints (e.g., corticosteroid injections) |
Parenteral forms include: solutions, suspensions, emulsions, and lyophilized (freeze-dried) powders for reconstitution.
Long-acting/depot injectables: Oil-based or microencapsulated formulations (e.g., long-acting depot antipsychotics like risperidone microspheres, paliperidone palmitate) that release drug slowly over weeks to months — primarily used to improve adherence in schizophrenia.
3. Topical & Transdermal
A. Topical (local effect)
Applied directly to skin or mucous membranes for a local effect.
| Form | Description | Examples |
|---|---|---|
| Ointments | Greasy, oil-based (high lipid content) | Corticosteroid ointments for skin |
| Creams | Oil-in-water emulsions; less greasy | Antifungals, corticosteroids |
| Gels | Aqueous polymer base; non-greasy | Diclofenac gel, benzoyl peroxide |
| Lotions | Aqueous suspension/solution | Calamine lotion |
| Pastes | Thick ointments with high powder content | Zinc oxide paste |
| Sprays | Aerosolized topical preparations | Wound dressings |
| Ophthalmic drops/ointments | For eye conditions | Antibiotic eye drops |
| Otic drops | For ear conditions | Antibiotic/corticosteroid ear drops |
| Nasal sprays | For allergic rhinitis, nasal congestion | Fluticasone nasal spray (doses so low systemic adrenal suppression is negligible) |
| Vaginal creams/suppositories/tablets | Local vaginal effect | Miconazole vaginal suppository (antifungal) |
B. Transdermal (systemic effect via skin)
Drug is absorbed through the skin to achieve systemic blood levels.
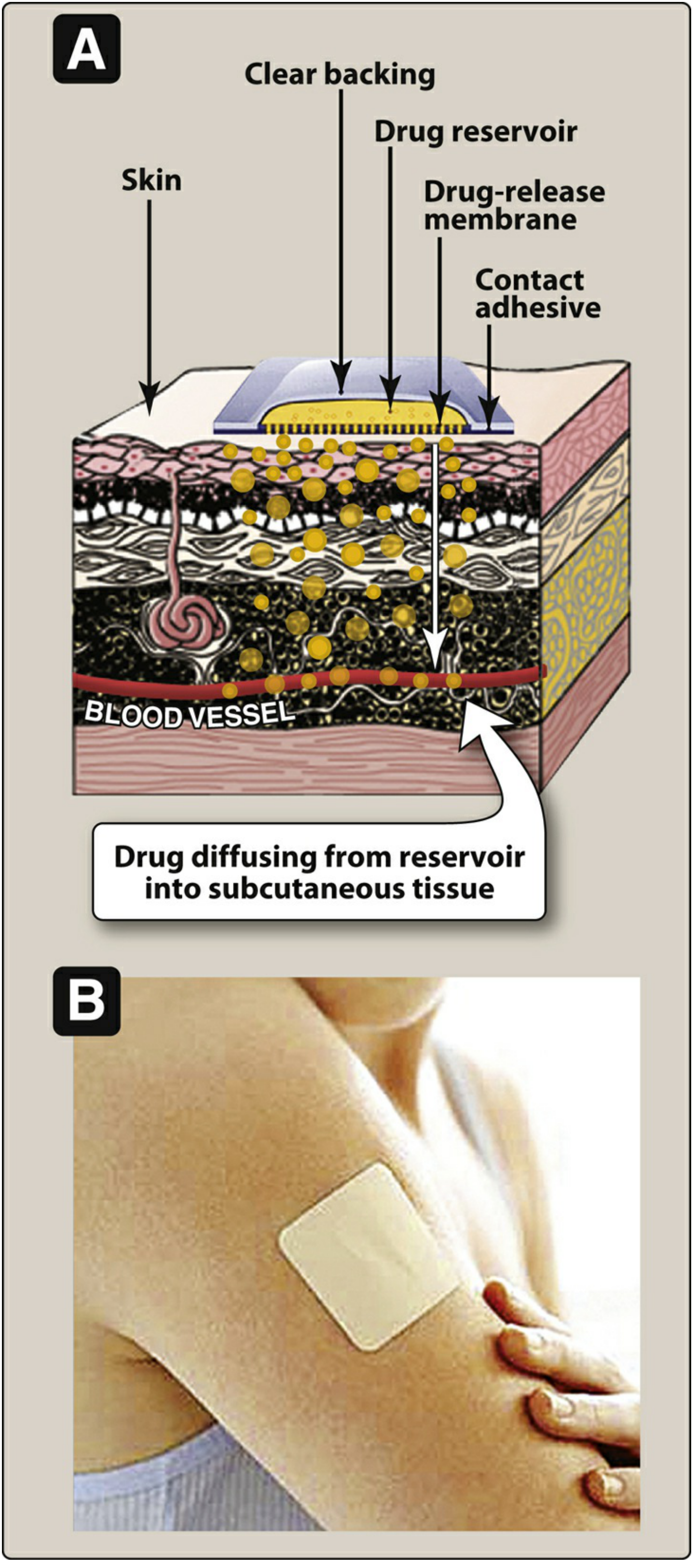
Mechanism: Drug reservoir → drug-release membrane → contact adhesive → diffusion through skin layers → blood vessels
Rate of absorption varies with:
- Skin thickness at application site
- Lipid solubility of the drug
Examples: Nicotine patch, fentanyl patch, nitroglycerin patch, estradiol patch, testosterone patch, scopolamine (motion sickness)
C. Inhalation
Forms: metered-dose inhalers (MDIs), dry powder inhalers (DPIs), nebulizers
- Drug delivered directly to the lungs → high local concentration at site of action
- Minimizes systemic side effects
- Used for asthma, COPD (bronchodilators: salbutamol, tiotropium; corticosteroids: budesonide, fluticasone, beclomethasone)
4. Special & Newer Dosage Forms
| Form | Description |
|---|---|
| Oral transmucosal | Drug incorporated into a lozenge (e.g., oral transmucosal fentanyl citrate — a solid dosage form on a stick; fentanyl is absorbed through oral mucosa) |
| Timed-release (circadian) tablets | Designed to mimic physiological drug release patterns (e.g., timed-release hydrocortisone that mimics the cortisol circadian rhythm for Addison disease and congenital adrenal hyperplasia; delayed-release prednisone for rheumatoid arthritis — taken at bedtime, releases in early morning when inflammation is highest) |
| Rapidly dissolving tablets | Disintegrate on the tongue; useful for patients with dysphagia or who "cheek" tablets (e.g., clozapine, olanzapine, aripiprazole ODT) |
| Implants/pellets | Subcutaneous implants for slow, sustained release over months |
| Liposomal preparations | Drug encapsulated in phospholipid vesicles; targets specific tissues; reduces toxicity (e.g., liposomal doxorubicin) |
Pediatric Dosage Form Considerations
(Katzung's Basic and Clinical Pharmacology)
- Most pediatric drugs are given as elixirs or suspensions
- Elixirs are alcoholic solutions → drug molecules evenly dissolved → no shaking required
- Suspensions contain undissolved particles → must be shaken before each dose
- Inadequate shaking of phenytoin suspension → underdosing early and toxicity late in therapy
- Calibrated medicine spoons or oral syringes should replace household teaspoons (measured volume varies 2.5–7.8 mL)
- Palatability is critical for adherence in children — bitter formulations may need flavored additives
- Dosing errors (10-fold decimal point errors) are a serious risk when doses are weight-calculated
Summary Comparison Table
| Property | Oral | IM | IV | Transdermal | Inhalation | Rectal |
|---|---|---|---|---|---|---|
| Onset | 30–90 min | 10–30 min | Immediate | Hours | Minutes | Variable |
| First-pass metabolism | Yes | No | No | No | Minimal | Partial bypass |
| Bioavailability | Variable | ~100% | 100% | Variable | High (locally) | Erratic |
| Patient self-administration | Easy | Difficult | Difficult | Easy | Requires training | Possible |
| Suitable for unconscious patient | No | Yes | Yes | Yes | No | Yes |
Sources:
- Lippincott Illustrated Reviews: Pharmacology, Chapters 1 (Routes of Administration)
- Katzung's Basic and Clinical Pharmacology, 16th Edition, Chapters on Pediatric Pharmacology and Corticosteroids
- Kaplan & Sadock's Comprehensive Textbook of Psychiatry (Antipsychotic Dosage Forms)
What about ampules viles , pessaries etc
Finding Sources
Finding Sources
Searching the Web
ampoules vials pessaries lozenges linctus pharmaceutical dosage forms pharmaceutical science
Finding Sources
Reading File
Finding Sources
Finding Sources
Loading Image
Finding Sources
I now have enough textbook content plus my comprehensive pharmaceutical knowledge to give a thorough answer. Here it is:
Additional Dosage Forms: Ampoules, Vials, Pessaries & More
1. Ampoules (Ampules)
An ampoule is a small, hermetically sealed glass container (typically 1–25 mL) that holds a sterile solution or powder for parenteral (injectable) use.
Key characteristics:
- Made from neutral (borosilicate) glass to prevent chemical interaction with the drug
- Sealed by melting the glass neck — the seal is broken open just before use (snap-off or score-and-break type)
- Single-dose only — once opened, the entire contents must be used; cannot be re-sealed
- No preservatives needed (used immediately after opening)
- Protects light-sensitive or air-sensitive drugs (complete hermetic seal)
- The contents are withdrawn using a filter needle to prevent glass particle contamination
Examples: Morphine sulfate ampoules, atropine ampoules, adrenaline (epinephrine) ampoules, diazepam ampoules, vitamins B and C for IV infusion
Ampoule vs. Vial — key difference: Ampoules are single-dose, glass-only, hermetically sealed; vials are sealed with a rubber stopper and can be single- or multi-dose.
2. Vials
A vial is a small glass or plastic bottle sealed with a rubber stopper (septum) and metal crimp cap, through which a needle is inserted to withdraw doses.
Types:
| Type | Description |
|---|---|
| Single-dose vial (SDV) | Contains one dose; no preservative added; discard after single use |
| Multi-dose vial (MDV) | Contains multiple doses; contains a preservative (e.g., benzalkonium chloride, thimerosal) to prevent microbial contamination after repeated needle punctures |
| Lyophilized (freeze-dried) vials | Contain a powder that must be reconstituted with a diluent (sterile water or saline) before use; used for unstable drugs (e.g., antibiotics, biologics, vaccines) |
Contents can be:
- Aqueous solution ready to inject
- Powder for reconstitution
- Concentrated solution for dilution before IV infusion
Examples: Insulin vials (multi-dose), vancomycin powder vials, heparin multi-dose vials, vaccines (e.g., influenza multi-dose vials), monoclonal antibodies (single-dose vials)
Storage considerations: Multi-dose vials must be stored correctly (often refrigerated) and discarded after a defined period once opened (typically 28 days per CDC guidelines).
3. Pessaries (Vaginal Pessaries)
The word "pessary" has two distinct meanings in medicine:
A. Pharmaceutical Pessary (Vaginal Suppository)
A solid dosage form designed for insertion into the vagina, where it dissolves or melts at body temperature to release drug for a local effect.
- Shape: torpedo-shaped, ovoid, or globular
- Base: typically cocoa butter, polyethylene glycol (PEG), or gelatin
- Mechanism: melts at 37°C → releases drug → absorbed by vaginal mucosa
Uses and examples:
| Drug | Indication |
|---|---|
| Clotrimazole 100/200/500 mg pessary | Vulvovaginal candidiasis |
| Miconazole 100/200/1200 mg pessary | Vulvovaginal candidiasis |
| Metronidazole pessary | Bacterial vaginosis, trichomoniasis |
| Progesterone pessary (e.g., Cyclogest) | Luteal phase support in IVF; threatened miscarriage |
| Dinoprostone (prostaglandin E2) pessary | Cervical ripening / induction of labour |
| Clindamycin pessary | Bacterial vaginosis |
B. Mechanical/Orthopaedic Pessary (Device)
A silicone or rubber device inserted into the vagina to provide mechanical support for pelvic organ prolapse (POP) or stress urinary incontinence — not a drug delivery form.
Types: ring, Gellhorn, donut, cube, Hodge, Shaatz, incontinence dish, inflatable ball, and more (23+ shapes).

Fitting: ~75% of women with prolapse can be successfully fitted. Material is usually silicone (non-allergenic, does not absorb odors).
4. Lozenges / Troches / Pastilles
Solid preparations designed to dissolve slowly in the mouth for local oropharyngeal effect or transmucosal absorption.
| Form | Description | Examples |
|---|---|---|
| Lozenge | Hard, candy-like; dissolves slowly in the mouth | Nicotine polacrilex lozenge (smoking cessation); throat lozenges (benzocaine, menthol) |
| Troche | Medicated lozenge; dissolves in the mouth; drug released locally | Clotrimazole 10 mg troche (oropharyngeal candidiasis — topical effect only) |
| Pastille | Soft, gelatin or glycerin-based; dissolves in mouth | Antiseptic throat pastilles |
| Oral transmucosal lozenge ("lollipop") | Drug on a stick; significant buccal/sublingual absorption | Oral transmucosal fentanyl citrate (OTFC) — rapid analgesia for breakthrough cancer pain |
Oral transmucosal fentanyl citrate is a solid dosage form: fentanyl incorporated into a sweetened lozenge on a stick; a portion is absorbed directly through the oral mucosa for rapid onset — Katzung's & Tintinalli's Emergency Medicine
5. Linctus
A viscous (thick) liquid oral preparation, usually sweet and syrupy, designed to be sipped slowly without being diluted with water. The viscosity prolongs contact with the throat mucosa.
- Used for coughs and sore throats
- Slow sipping allows drug to coat the pharyngeal mucosa
- Often contains glycerol, honey, or sugar base
- Examples: Simple linctus (glycerol base, demulcent), pholcodine linctus (cough suppressant), codeine linctus (cough suppressant/analgesic)
6. Gargle / Mouthwash
Gargle: Aqueous solution held in the throat while exhaling through it to coat pharyngeal mucosa.
Mouthwash: Liquid swished around the mouth and spat out.
- Used for local antiseptic, anti-inflammatory, or anaesthetic effects in the mouth and throat
- Examples: Chlorhexidine mouthwash (antiseptic), benzydamine gargle (anti-inflammatory/analgesic), lidocaine "laryngeal gargle" via endoscope during bronchoscopy, alcohol-free antibacterial mouthwash for oral piercings
7. Other Less-Discussed Dosage Forms
| Form | Description | Examples |
|---|---|---|
| Implants / Pellets | Small solid cylinders implanted subcutaneously for prolonged, sustained drug release over months to years | Hormonal implants (etonogestrel — Nexplanon®), testosterone pellets |
| Intrauterine devices (IUDs) | Placed inside the uterine cavity; releases drug locally over years | Levonorgestrel IUD (Mirena®) — progestogen released locally for contraception/menorrhagia |
| Ear drops (Otic drops) | Sterile solutions/suspensions instilled into the ear canal | Antibiotic + steroid combination drops (ciprofloxacin/dexamethasone) |
| Eye drops / Ophthalmic solutions | Sterile preparations applied to the conjunctival sac | Timolol (glaucoma), chloramphenicol (conjunctivitis) |
| Eye ointments | Sterile, greasy ophthalmic preparations | Tetracycline eye ointment |
| Nasal drops / sprays | Instilled or sprayed into nasal cavity | Xylometazoline (decongestant), budesonide (rhinitis) |
| Dusting powders | Fine powder applied to skin | Antifungal powder (miconazole powder), talc |
| Medicated plasters | Drug-impregnated adhesive strips | Salicylic acid plasters (warts), lidocaine plasters (neuropathic pain) |
| Aerosol inhalers (MDI) | Pressurized metered-dose inhaler | Salbutamol, beclomethasone |
| Enemas | Liquid/foam instilled into the rectum | Hydrocortisone enema (ulcerative colitis), sodium phosphate enema (constipation) |
| Intravenous infusion bags | Large-volume parenteral solutions | Normal saline, dextrose, total parenteral nutrition (TPN) |
Quick Reference Summary
DOSAGE FORM CONTAINERS:
├── Ampoule — glass, hermetically sealed, single-dose, no preservative
├── Vial — rubber-stoppered, single or multi-dose, may contain preservative
│ └── Lyophilized vial — powder + diluent for reconstitution
│
VAGINAL/LOCAL:
├── Pharmaceutical pessary — solid, dissolves vaginally (drug delivery)
├── Mechanical pessary — silicone device for prolapse (not drug delivery)
│
ORAL MUCOSAL:
├── Lozenge / Troche / Pastille — slow oral dissolution
├── OTFC lozenge ("lollipop") — transmucosal systemic absorption
│
LIQUID ORAL:
├── Linctus — viscous, sipped slowly, coats throat
├── Gargle — aqueous, held in throat
├── Mouthwash — swished and expectorated
│
SUSTAINED RELEASE (NOVEL):
├── Implant / Pellet — subcutaneous, months–years duration
├── IUD — intrauterine, local hormonal release
Sources:
- Lippincott Illustrated Reviews: Pharmacology (Routes and forms)
- Pfenninger and Fowler's Procedures for Primary Care, 3rd ed. (Pessary fitting)
- Tintinalli's Emergency Medicine (OTFC lozenge)
- Goodman & Gilman's The Pharmacological Basis of Therapeutics (Troches)
- Katzung's Basic and Clinical Pharmacology, 16th ed. (Pediatric and special dosage forms)
Currarino syndrome
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.