Also read anatomy of the lacrimal system and cornea and diseases
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have extensive content. Let me compile the comprehensive answer.
Anatomy of the Lacrimal System, Cornea, and Corneal Diseases
PART 1: LACRIMAL DRAINAGE SYSTEM
Source: Kanski's Clinical Ophthalmology, 10th Edition
Anatomy
The lacrimal drainage system consists of five key structures:
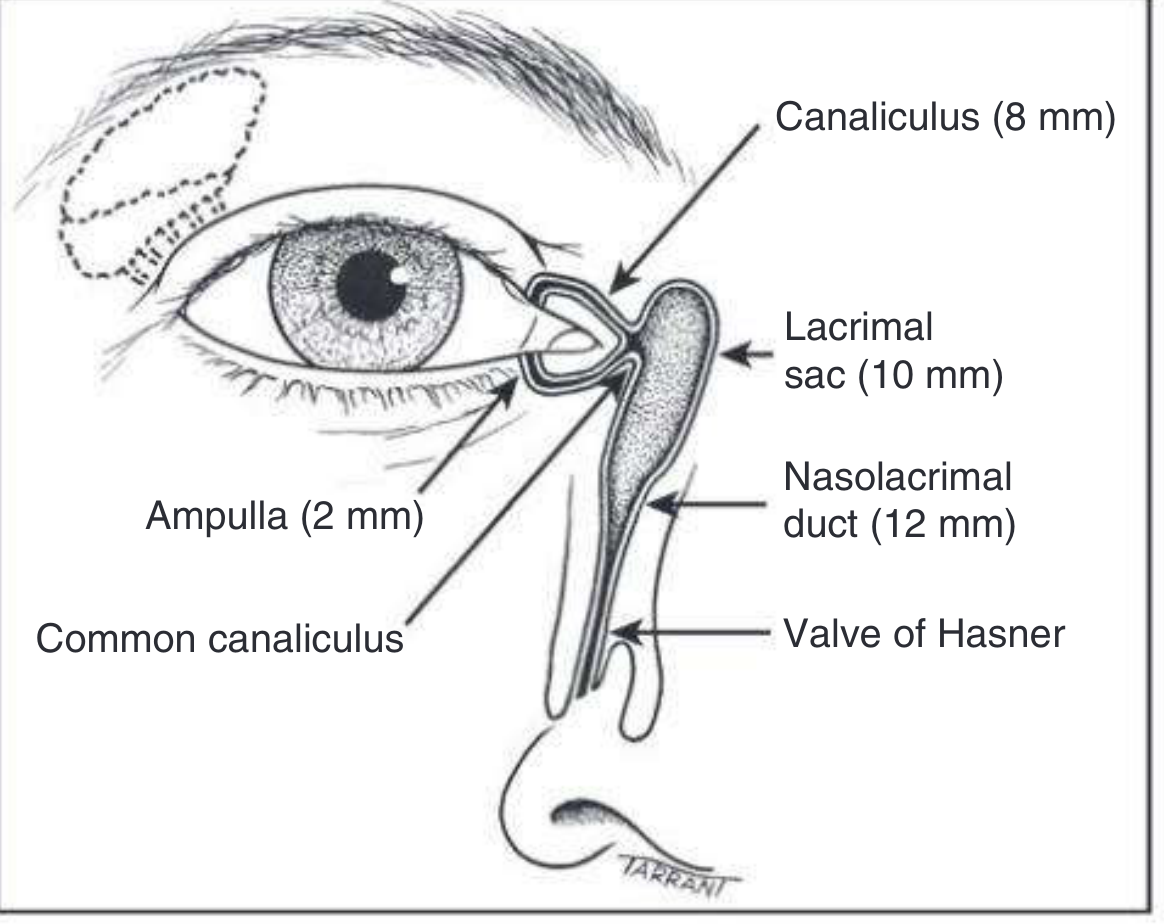
1. The Puncta
- Located at the posterior edge of the lid margin, at the junction of the lash-bearing lateral five-sixths (pars ciliaris) and the medial non-ciliated one-sixth (pars lacrimalis).
- The punctum and vertical canaliculus are part of the tarsal plate.
- Normally the puncta face slightly posteriorly and can be inspected by everting the medial lids.
2. The Canaliculi
- Each canaliculus passes vertically from the lid margin for about 2 mm (the ampulla), then turns medially and runs horizontally for ~8 mm to reach the lacrimal sac.
- The horizontal canaliculus is surrounded by the palpebral part of the orbicularis oculi muscle (Horner muscle).
- The superior and inferior canaliculi usually unite (>90% of cases) to form the common canaliculus, which opens into the lateral wall of the lacrimal sac.
- A small mucosal flap - the Rosenmüller valve - overhangs the junction of the common canaliculus and the lacrimal sac (the internal punctum), preventing reflux of tears into the canaliculi.
3. The Lacrimal Sac
- 10-12 mm long, lying in the lacrimal fossa between the anterior and posterior lacrimal crests.
- The lacrimal bone and the frontal process of the maxilla separate the lacrimal sac from the middle meatus of the nasal cavity.
- In a dacryocystorhinostomy (DCR), an anastomosis is created between the sac and the nasal mucosa to bypass nasolacrimal duct obstruction.
4. The Nasolacrimal Duct
- 12-18 mm long, the inferior continuation of the lacrimal sac.
- Descends, angling slightly laterally and posteriorly, to open into the inferior nasal meatus, lateral to and below the inferior turbinate.
- The opening is partially covered by a mucosal fold - the valve of Hasner.
Physiology of Tear Drainage
Tears secreted by the main and accessory lacrimal glands flow across the ocular surface. Drainage proceeds as follows:
- Tears flow along the upper and lower marginal strips, pooling in the lacus lacrimalis medial to the lower puncta, then entering the canaliculi by capillarity and suction.
- With each blink, the pretarsal orbicularis oculi muscle compresses the ampullae, shortens and compresses the horizontal canaliculi, and moves the puncta medially - resisting reflux. Simultaneously, contraction of the lacrimal part of the orbicularis creates positive pressure that forces tears down the nasolacrimal duct into the nose (mediated by helically arranged connective tissue fibres around the lacrimal sac).
- When the eyes open, the canaliculi and sac expand, creating negative pressure that draws tears from the canaliculi into the sac.
Common Lacrimal Diseases
| Condition | Key Features |
|---|---|
| Conjunctivochalasis | Redundant conjunctival folds occlude the puncta |
| Punctal stenosis | Primary (idiopathic) or secondary (drug-induced, infection, inflammation) |
| Canalicular obstruction | May require complex surgical repair; caused by trauma, infection, drugs |
| Nasolacrimal duct obstruction | Most common cause of epiphora; treated by DCR |
| Dacryolithiasis | Calcified concretions within the lacrimal sac |
| Chronic canaliculitis | Often caused by Actinomyces israelii; presents with red, swollen punctum |
| Acute dacryocystitis | Painful swelling over the lacrimal sac; usually S. aureus or Streptococcus |
| Chronic dacryocystitis | Mucoid/mucopurulent reflux on pressure over sac; treated by DCR |
| Congenital NLD obstruction | Failure of valve of Hasner to open; resolves spontaneously in 90% by 1 year |
| Congenital dacryocele | Distended lacrimal sac at birth from obstruction at both ends |
PART 2: CORNEA - ANATOMY
Sources: Kanski's Clinical Ophthalmology, 10th Ed.; Robbins & Kumar Basic Pathology
Structure and Layers
The cornea and its overlying tear film make up the major refractive surface of the eye. Its shape significantly influences refractive power (the basis of LASIK surgery for myopia and hyperopia).
The cornea has 5 layers (from anterior to posterior):
| Layer | Key Features |
|---|---|
| Epithelium | 5-6 cell layers of non-keratinized stratified squamous epithelium; rests on a basement membrane; regenerates rapidly |
| Bowman layer | Acellular condensed collagen just beneath the epithelial basement membrane; does not regenerate if damaged |
| Stroma | ~90% of corneal thickness; collagen lamellae arranged in precise orthogonal pattern for transparency; avascular; contains keratocytes (fibroblasts) |
| Descemet membrane | Specialized basement membrane of the endothelium; thickens with age |
| Endothelium | Single layer of cells derived from neural crest; lines the posterior surface; pumps fluid out of stroma to maintain clarity; does not regenerate in humans |
Key properties:
- The stroma lacks blood vessels and lymphatics - this contributes to corneal transparency and the high success rate of corneal transplantation (immune privilege).
- The corneal endothelium is derived from neural crest and is not related to vascular endothelium.
PART 3: CORNEAL DISEASES
1. Keratitis and Corneal Ulceration
Kanski's + Robbins & Kumar
Pathogens causing keratitis include: bacterial, fungal, viral (especially HSV and VZV), and protozoal (Acanthamoeba).
Pathophysiology: Dissolution of the corneal stroma is accelerated by activation of collagenases within corneal epithelium and stromal fibroblasts (keratocytes). Exudate from iris and ciliary body vessels leaking into the anterior chamber may form a hypopyon (visible pus level) - though the hypopyon seldom contains organisms and represents a vascular response to acute inflammation.
Herpes simplex keratitis (chronic form): May be associated with a granulomatous reaction involving the Descemet membrane.
Signs of active keratitis:
- Epithelial defect with fluorescein staining
- Stromal infiltrate/opacity
- Hypopyon
- Ciliary injection
2. Keratoconus
Kanski's Clinical Ophthalmology, 10th Ed.; Robbins & Kumar Basic Pathology
Definition: A progressive disorder in which central or paracentral corneal stromal thinning occurs, accompanied by apical protrusion and irregular astigmatism.
Epidemiology:
- Prevalence: 0.1-0.2% (incidence ~1 in 2000)
- Men slightly more affected than women
- Presentation commonly in the teens or twenties
- ~50% of normal fellow eyes progress to KC within 16 years
- Eventually bilateral in almost all cases
Risk factors and associations:
- Allergy, asthma, eczema, persistent eye rubbing
- Systemic: Down syndrome, Ehlers-Danlos syndrome, Marfan syndrome, osteogenesis imperfecta
- Ocular: vernal keratoconjunctivitis, Leber congenital amaurosis, retinitis pigmentosa
Grading (by keratometry):
- Mild: <48 D
- Moderate: 48-54 D
- Severe: >54 D
Clinical Signs:
- "Oil droplet" red reflex on direct ophthalmoscopy at 0.5 m distance
- Irregular "scissoring" reflex on retinoscopy
- Vogt striae - fine vertical lines in the deep stroma
- Fleischer ring - iron deposits at the base of the cone (visible with cobalt blue light)
- Munson sign - V-shaped distortion of the lower lid on downgaze
- Rizzuti sign - conical reflection on the nasal cornea when light is directed from the temporal side
Histology (Robbins): Thinning of the cornea with breaks in the Bowman layer are the hallmarks.
Complication - Acute Hydrops:
- Descemet membrane ruptures, allowing aqueous humor to flood the corneal stroma
- Sudden severe vision loss
- May be followed by corneal scarring
Treatment:
- Spectacles or rigid contact lenses (RGP) for mild-moderate
- Corneal collagen cross-linking (CXL) to halt progression
- Intrastromal corneal ring segments (ICRS) for moderate disease
- Penetrating keratoplasty (PKP) or deep anterior lamellar keratoplasty (DALK) for advanced/contact-lens-intolerant cases
3. Fuchs Endothelial Dystrophy
Robbins & Kumar Basic Pathology
- Results from loss of corneal endothelial cells, leading to edema and thickening of the stroma.
- One of the principal indications for corneal transplantation in the United States.
- Major manifestations: stromal edema and bullous keratopathy (blistering of the epithelium).
- Treated by Descemet membrane endothelial keratoplasty (DMEK) or DSAEK.
4. Xerophthalmia (Vitamin A Deficiency)
Kanski's Clinical Ophthalmology
WHO Grading:
- XN = night blindness
- X1A = conjunctival xerosis; X1B = Bitot spots
- X2 = corneal xerosis
- X3A/X3B = corneal ulceration (<1/3 or >1/3 of cornea)
- XS = corneal scar; XF = xerophthalmic fundus
Keratomalacia (sterile corneal melting by liquefactive necrosis) is an indicator of very severe vitamin A deficiency - treated as a medical emergency due to risk of death in infants. Treatment: oral vitamin A 200,000 IU (oil-based) or IM 100,000 IU (aqueous-based).
5. Dry Eye / Keratoconjunctivitis Sicca
Kanski's Clinical Ophthalmology
Corneal complications of severe dry eye include:
- Punctate epithelial erosions (stain with fluorescein)
- Filamentary keratitis - strands of mucus/debris attached to corneal surface (stain with rose Bengal)
- Mucous plaques
- In severe cases: epithelial breakdown, corneal melting, perforation, bacterial keratitis
Investigations measure:
- Tear film break-up time (BUT) - stability
- Schirmer test - aqueous production
- Rose Bengal / lissamine green staining - epithelial surface damage
Key Sources:
- Kanski's Clinical Ophthalmology: A Systematic Approach, 10th Edition - Chapters 3 (Lacrimal drainage), 5 (Dry eye / cornea), 7 (Corneal ectasia/diseases)
- Robbins & Kumar Basic Pathology - Chapter on Eye Pathology (Cornea section)
This is a shared conversation. Sign in to Orris to start your own chat.