Histopathology of squamous cell carcinoma
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Loading Image
Loading Image
Reading File
Reading File
I now have comprehensive information to write a detailed answer. Let me compile everything.
Histopathology of Squamous Cell Carcinoma (SCC)
Overview
SCC arises from atypical keratinocytes of the squamous epithelium. The defining histopathological event in invasive SCC is the growth of these atypical keratinocytes beyond the basement membrane into the underlying dermis (or stroma, depending on the site).
Hallmark Features (H&E Stain)
Fig. 112-6 - Well-differentiated SCC (H&E, x50): Atypical keratinocytes originating from the epidermis and infiltrating the dermis with minimal pleomorphism and prominent keratinization, including horn pearl formation.
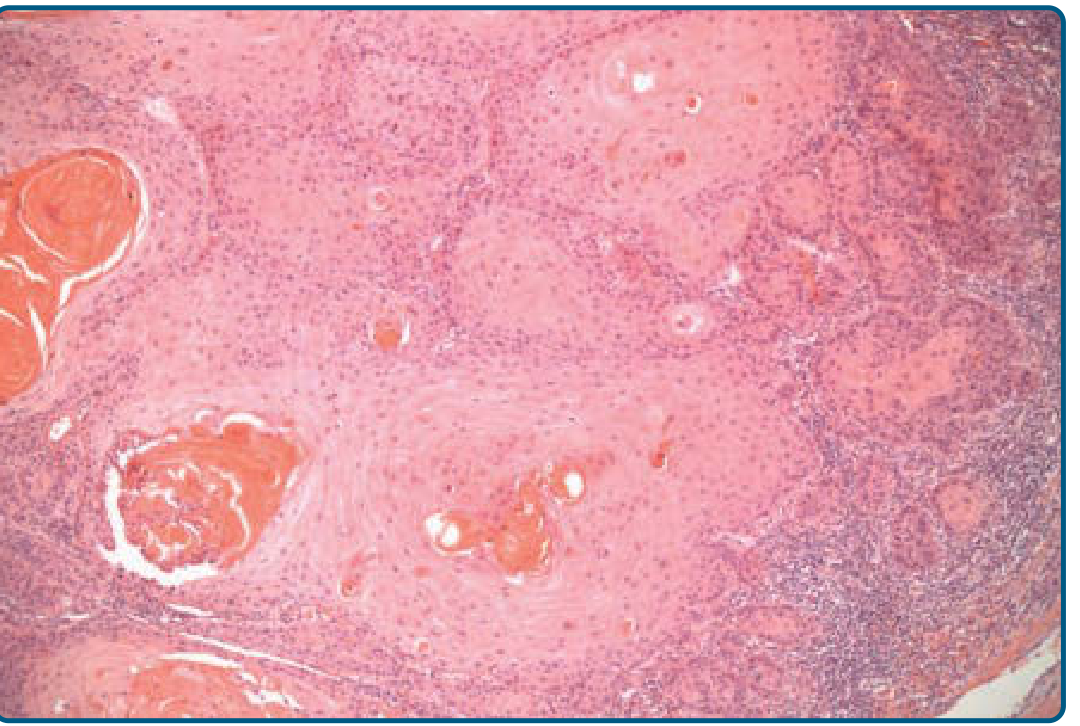
The key histological features are:
-
Keratinization - the most characteristic feature
- Keratin (horn) pearls: concentric whorls of keratinized squamous cells within the dermis/stroma - pathognomonic of well-differentiated SCC
- Individual cell dyskeratosis: single cells with bright eosinophilic cytoplasm undergoing premature/abnormal keratinization
- Parakeratosis (nuclei retained in cornified layer)
-
Intercellular bridges (desmosomes): visible between adjacent tumor cells, confirming squamous lineage
-
Cytological atypia:
- Large, pleomorphic nuclei
- Prominent nucleoli (often more than one large purple nucleolus per cell - see arrows in Fig. 2.17C)
- Abundant eosinophilic cytoplasm
- Increased nuclear-to-cytoplasmic ratio
-
Mitotic figures: often numerous, including abnormal mitoses
-
Invasion: tumor nests and tongues of epithelium with jagged, irregular borders extending into the stroma
-
Stromal response: desmoplastic reaction, inflammatory infiltrate at the tumor-stroma interface
Histopathological image (high power)
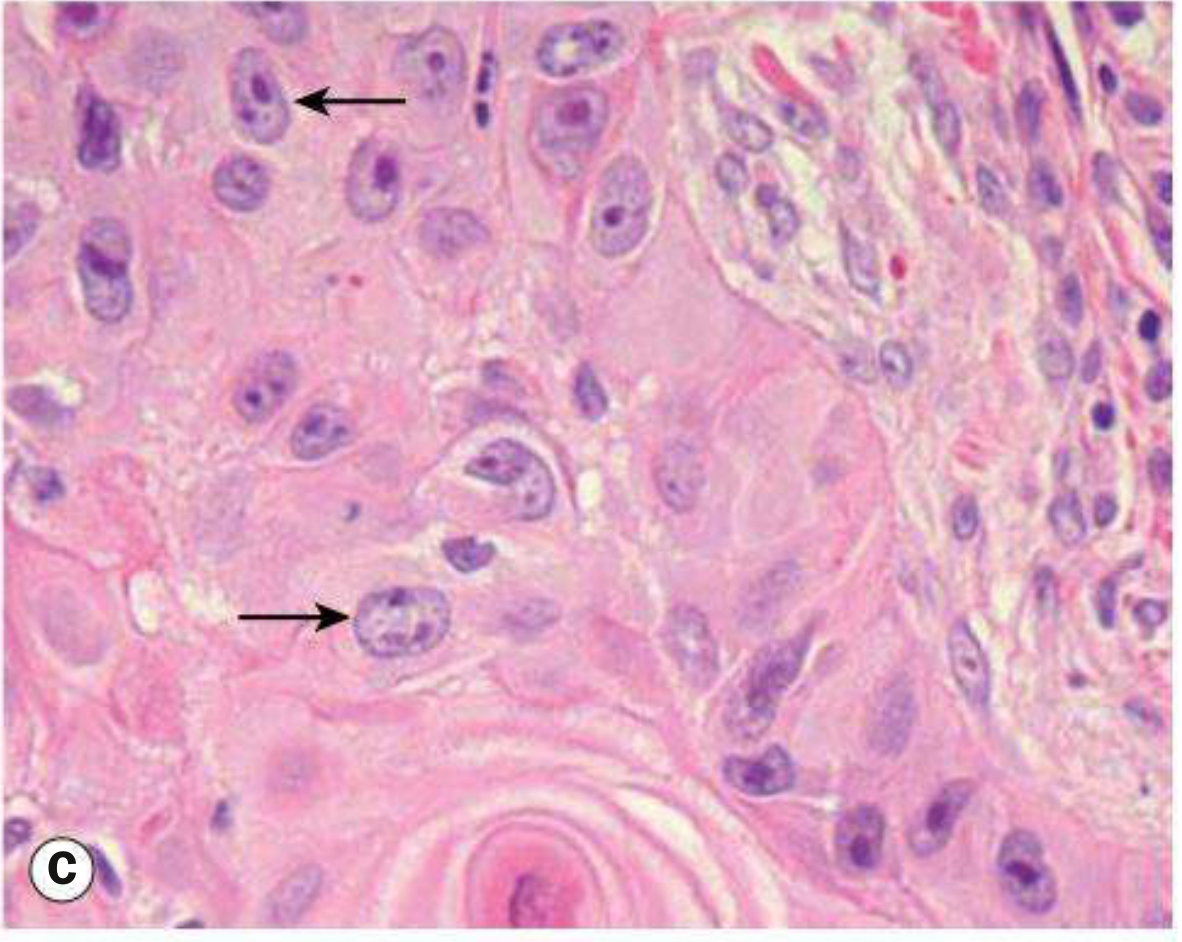
Fig. 2.17C (Kanski's Ophthalmology): Acanthotic squamous epithelium with eosinophilic islands of dysplastic squamous epithelium within the dermis. Large nuclei with more than one large purple nucleolus are indicated by arrows. A keratin pearl is visible at the bottom.
Grading (Degree of Differentiation)
| Grade | Features |
|---|---|
| G1 - Well differentiated | Minimal pleomorphism; prominent keratinization; keratin pearls abundant; intercellular bridges visible; few mitoses |
| G2 - Moderately differentiated | Intermediate features; keratinization present but less prominent; more mitoses |
| G3 - Poorly differentiated | High-grade atypia; frequent mitoses; sparse or absent keratinization; intercellular bridges hard to find |
| G4 - Undifferentiated | No squamous features; requires immunohistochemistry (p40, cytokeratins) to confirm diagnosis |
Carcinoma In Situ (SCC in Situ / Bowen's Disease)
Before invasion, the dysplastic changes are confined to the full thickness of the epidermis with an intact basement membrane. This is called:
- Carcinoma in situ - dysplastic cells throughout the epidermis
- Bowen's disease - a specific form of intraepidermal SCC
Once the basement membrane is breached, the lesion is classified as invasive SCC.
Histopathological Variants
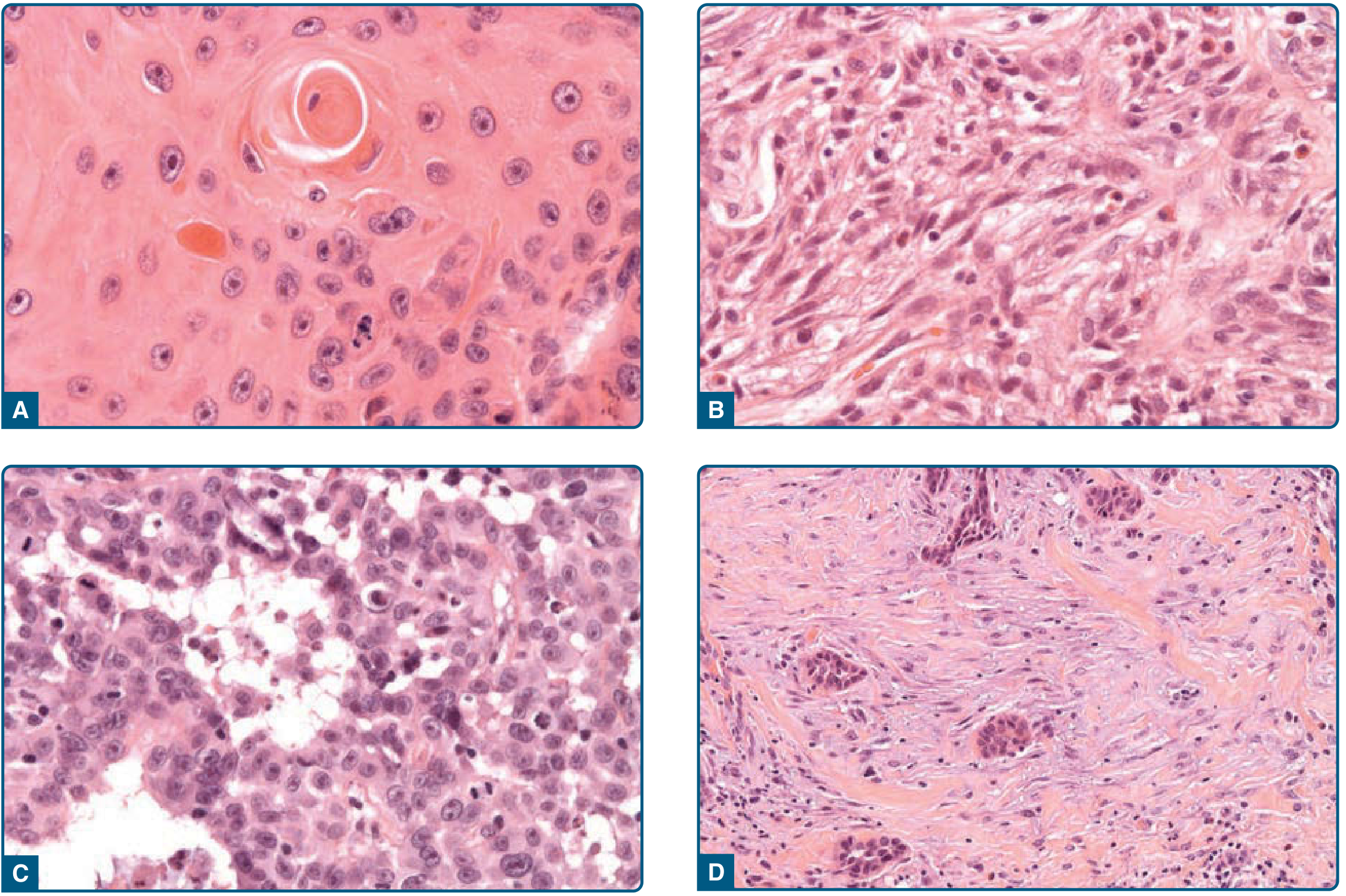
1. Common (Classic) SCC
The typical picture described above with infiltrating atypical keratinocytes and variable keratinization.
2. Spindle-Cell SCC
- Spindled morphology of atypical keratinocytes
- Lacks keratinization - can mimic sarcoma, melanoma, atypical fibroxanthoma
- Requires cytokeratin immunohistochemistry for confirmation
- Arises in sun-exposed skin of elderly patients or post-radiation
3. Acantholytic (Adenoid) SCC
- Extensive acantholysis (loss of cell-cell adhesion) of tumor keratinocytes
- Creates pseudoglandular (tubular/alveolar) spaces within the tumor
- Can mimic adenocarcinoma
- Higher metastatic potential (~19% metastatic rate)
- Comprises <5% of all SCCs
4. Verrucous SCC
- Well-differentiated variant with pushing (non-infiltrative) borders
- Deep downward proliferations of monomorphic, light eosinophilic keratinocytes with small nuclei
- Superficially resembles verruca: parakeratosis, acanthosis, prominent stratum granulosum
- Minimal nuclear atypia; keratin pearls and individual cell dyskeratosis are absent
- Low metastatic potential
5. Desmoplastic SCC
- Infiltrative growth with abundant mucinous or sclerotic stroma surrounding tumor cells
- Tumor cells may appear deceptively bland
- High rates of perineural invasion - considered high-risk
Standard Histopathology Report for SCC
Per Fitzpatrick's Dermatology, a complete report should include:
| Parameter | Details |
|---|---|
| Histologic subtype | Common / Verrucous / Desmoplastic / Acantholytic / Spindle-cell |
| Grading | G1 (well) / G2 (moderate) / G3 (poor) / G4 (undifferentiated) |
| Maximum tumor thickness | In mm |
| Clark level | >IV or <IV |
| Perineural invasion | Yes / No |
| Vascular/lymphatic invasion | Yes / No |
| Margin status | Complete excision, minimum lateral and deep margin in mm |
Immunohistochemistry
When morphological features are ambiguous (especially in poorly differentiated or spindle-cell SCC):
- Cytokeratins (CK5/6, AE1/AE3) - positive in SCC
- p40 / p63 - squamous differentiation markers; key for confirming lung SCC
- EMA - may be positive
Site-Specific Notes
- Lung SCC: Centrally located (segmental/subsegmental bronchi); characterized by keratinization and/or intercellular bridges; preceded by squamous metaplasia → dysplasia → carcinoma in situ sequence; p40 is the most specific IHC marker (Robbins Pathologic Basis of Disease)
- Skin: Most common on sun-exposed areas; precursor lesions include actinic keratosis
- Ocular surface/eyelid: Composed of variably sized groups of atypical epithelial cells with prominent nuclei and abundant eosinophilic cytoplasm; well-differentiated forms show keratin pearls and intercellular bridges (Kanski's Ophthalmology)
Sources: Fitzpatrick's Dermatology (8e), Ch. 112; Kanski's Clinical Ophthalmology (10e), Ch. 2; Robbins & Cotran Pathologic Basis of Disease (10e), Ch. 15
This is a shared conversation. Sign in to Orris to start your own chat.