Male disorders
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have comprehensive content from Goldman-Cecil Medicine for all three topics. Let me compile the full detailed clinical review.
Male Reproductive Disorders: A Detailed Clinical Review
Source: Goldman-Cecil Medicine (International Edition); Textbook of Family Medicine 9e
1. Male Hypogonadism (Androgen Deficiency)
Definition and Epidemiology
Male hypogonadism is diagnosed in men with consistent symptoms and signs and unequivocally low circulating testosterone levels. Most men with severe androgen deficiency have very low intratesticular testosterone and are infertile.
- Klinefelter syndrome (the most common genetic cause): ~5 per 10,000 men
- Iatrogenic causes (chemotherapy, testicular/pituitary radiotherapy) are the most common etiologies aside from age and obesity
- Obesity and aging together produce mixed testicular + hypothalamic-pituitary dysfunction
Classification
| Type | LH / FSH | Defect Location |
|---|---|---|
| Primary hypogonadism (hypergonadotropic) | ↑ LH, ↑ FSH | Testis |
| Secondary hypogonadism (hypogonadotropic) | ↓ or normal LH, ↓ FSH | Hypothalamus or pituitary |
| Combined | Mixed pattern | Age, obesity, systemic disease |
Causes
Primary (testicular) - Table 216-2:
- Congenital: Klinefelter syndrome (47,XXY and variants), testosterone biosynthetic enzyme defects, 5α-reductase deficiency, androgen resistance syndrome, myotonic dystrophy
- Developmental: Cryptorchidism
- Acquired: Orchitis (mumps, HIV), granulomatous disease (TB, leprosy), infiltrative disease (hemochromatosis, amyloidosis), trauma/torsion, irradiation, toxins (alcohol, heavy metals, DDT, insecticides)
- Drugs: Cytotoxic agents (alkylating agents), ketoconazole, abiraterone, cimetidine, flutamide, cyproterone, spironolactone
- Autoimmune testicular failure
- Systemic disease: Cirrhosis, chronic renal failure, sickle cell disease
Secondary (hypogonadotropic) - Table 216-3:
- Congenital/idiopathic: Isolated GnRH deficiency - Kallmann syndrome (with anosmia, 80% of cases) or without anosmia; Prader-Willi syndrome; Laurence-Moon-Biedl syndrome
- Acquired: Traumatic brain injury, pituitary/cranial surgery or irradiation, pituitary adenomas (prolactinoma - most common pituitary tumor in men, usually a macroadenoma >1 cm at presentation), other pituitary tumors, autoimmune hypophysitis (including checkpoint inhibitor-induced), hemochromatosis, alcohol abuse disorder, type 2 diabetes, HIV
Pathophysiology
- Primary: Testicular failure → low testosterone → loss of negative feedback → ↑ LH and FSH
- Secondary: Hypothalamic or pituitary failure → ↓ GnRH or gonadotropins → low LH/FSH → low testosterone
- Obesity → lower SHBG + decreased testosterone secretion → low total and free testosterone
- Androgen resistance states (androgen receptor defects, 5α-reductase deficiency) - testosterone is normal or elevated, but action is impaired
Clinical Manifestations
| Stage of Life | Presentation |
|---|---|
| Neonatal | Micropenis, undescended testes, ambiguous genitalia |
| Childhood/Adolescent | Incomplete or delayed puberty (most specific symptom) |
| Adult | ↓ libido, erectile dysfunction, loss of body hair, gynecomastia, subfertility, hot flashes, loss of height |
| Nonspecific | ↓ energy and mood, poor concentration, ↑ abdominal fat, ↓ muscle mass |
Diagnosis
- Morning serum total testosterone (8-10 AM; normal 264-916 ng/dL in European/American men aged 19-39 yrs) - must be confirmed on at least 2 occasions
- LH and FSH: ↑ = primary; normal to low = secondary
- Prolactin: Measure if LH + testosterone are both low (to rule out prolactinoma)
- SHBG: Elevated in hyperthyroidism, liver disease, estrogen excess; low in hypothyroidism, obesity, PCOS, acromegaly
- Semen analysis: Assesses spermatogenesis
- MRI pituitary: If secondary hypogonadism suspected or prolactin elevated
- Bone mineral density (BMD)
- Genetic studies (karyotype for Klinefelter; Y microdeletion for azoospermia)
Key physical exam findings:
- Testicular volume <15 mL (orchidometer)
- Small, firm testes (Klinefelter)
- Anosmia (Kallmann syndrome)
- Gynecomastia, decreased facial/body hair, reduced muscle mass, micropenis
Treatment: Testosterone Replacement Therapy (TRT)
Indications: Confirmed symptomatic hypogonadism
Benefits: Improved libido/sexual function, increased muscle mass and strength, increased BMD, improved anemia, decreased body fat, improved mood
Risks: Fluid retention, gynecomastia, acne, polycythemia, ↓ HDL-cholesterol, sleep apnea, prostate disease (aggravates existing carcinoma), possible cardiovascular events (debated)
Contraindications: Prostate cancer, breast cancer, erythrocytosis, severe heart failure, active desire for fertility (TRT suppresses spermatogenesis)
Delivery systems (Table 216-6):
| Formulation | Route | Dose | Notes |
|---|---|---|---|
| Testosterone gel 1-2% | Transdermal | 50-100 mg/day (delivers 5-10 mg) | Most widely used in US; transfer risk to contacts |
| Intranasal testosterone gel | Intranasal | 3x/day | No transfer risk |
| Testosterone enanthate/cypionate | IM | 150-200 mg q2-3 weeks or 50-100 mg weekly SC | Weekly SC = more stable levels |
| Testosterone undecanoate | IM | 750 mg q10 weeks (US) | Preferred in many countries |
| Testosterone undecanoate | Oral | 158-396 mg twice daily with food | Avoids first-pass metabolism via lymphatics |
| Transbuccal (mucoadhesive) | Buccal | 30 mg twice daily | Direct systemic absorption |
Note: Modified 17α-alkylated androgens (e.g., methyltestosterone) are hepatotoxic and should not be used for TRT.
For hypogonadotropic hypogonadism + desired fertility: Use gonadotropins (hCG + FSH) or pulsatile GnRH rather than testosterone.
2. Male Infertility
Definition and Epidemiology
Infertility = failure to achieve pregnancy after ≥1 year of frequent unprotected intercourse. In the US and Europe, 1-year prevalence is ~15% of couples.
- Male factor alone: 25-30%
- Female factor alone: 30-35%
- Combined: 25-30%
- Unexplained: ~20%
Causes (Table 35-14 - Common Diagnoses)
| Category | Incidence |
|---|---|
| Idiopathic | 50-60% |
| Varicocele | 15-35% (most common identifiable cause) |
| Primary testicular failure (Klinefelter, Y deletions, cryptorchidism, orchitis, irradiation, drugs) | 10-20% |
| Genital tract obstruction (congenital absence of vas deferens, vasectomy, epididymal obstruction) | ~5% |
| Hypogonadotropic hypogonadism (pituitary adenoma, hyperprolactinemia, idiopathic) | 3-4% |
| Other (sperm autoimmunity, drugs, toxins, systemic illness) | ~5% |
Pathobiology
- Testicular disorders = most frequent identifiable cause
- Epididymis = main site for sperm maturation; lumicrine factor disruptions may explain many cases
- Genetic causes (now diagnosable in up to 50% with exome/whole-genome sequencing):
- Chromosomal disorders and translocations
- Y chromosome microdeletions (up to 25% of infertile men; Yq11 region = azoospermia factor, AZF)
- AZFa and AZFb mutations → azoospermia
- AZFc mutations → oligozoospermia
- TEX11 gene mutations, STAG3, DMRT1 → meiotic arrest/azoospermia
- Ciliary dyskinesia, flagellar abnormalities, sperm head defects
Workup
Step 1: Thorough history (erectile function, STIs, medications, surgeries, prior fertility, drug/alcohol use, family genetic history) and physical examination
Step 2: Semen analysis (first and usually only test needed)
WHO Semen Analysis Reference Ranges (Lower 5th Percentile):
| Parameter | Lower Reference Limit |
|---|---|
| Volume | 1.4 mL |
| Sperm concentration | 16 million/mL |
| Total count | 39 million/ejaculate |
| Motility | 42% motile; 30% progressively motile |
| Morphology (strict criteria) | 4% normal forms |
| Vitality (live) | 54% |
| Leukocytes | <1 million/mL |
Step 3 (if semen analysis is abnormal x2): Serum testosterone, LH, FSH, prolactin
Extended tests: Sperm DNA fragmentation, sperm antibodies, semen biochemistry, genetic/chromosomal studies
Diagnostic Algorithm
The flowchart below (from Goldman-Cecil) shows the systematic approach to male infertility diagnosis and treatment:
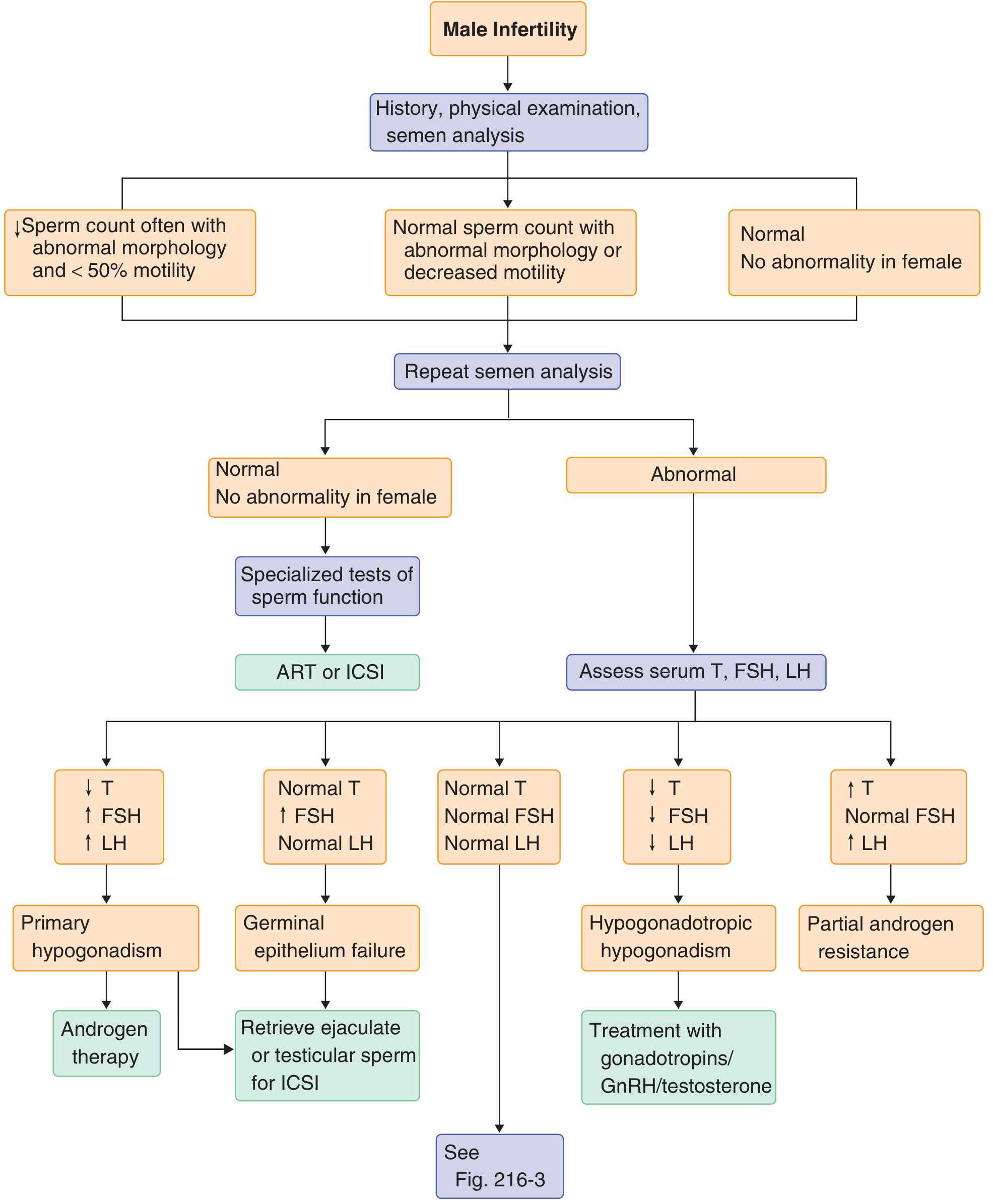
Key hormonal patterns in the algorithm:
- ↓T, ↑FSH, ↑LH → Primary hypogonadism → androgen therapy
- Normal T, ↑FSH, normal LH → Germinal epithelium failure → retrieve ejaculate/testicular sperm for ICSI
- ↓T, ↓FSH, ↓LH → Hypogonadotropic hypogonadism → gonadotropins/GnRH/testosterone
- ↑T, normal FSH, ↑LH → Partial androgen resistance
Management
- Treat underlying infection with antibiotics (if genital tract infection present)
- Varicocelectomy (for varicocele-associated infertility)
- Counseling about lifestyle and environmental factors (heat exposure, toxins)
- Gonadotropin therapy (hCG + FSH) for hypogonadotropic hypogonadism - highly effective
- ART/ICSI (intracytoplasmic sperm injection) for severe oligospermia or azoospermia
- Microsurgical testicular sperm extraction (micro-TESE) + ICSI for non-obstructive azoospermia - even successful in Klinefelter syndrome
- Empirical medical treatments (clomiphene citrate, aromatase inhibitors, recombinant FSH) - not generally recommended due to limited evidence, though high-dose FSH (700-1050 IU/week) can increase sperm concentration and motility
- Obstructive azoospermia (absent vas deferens, vasectomy reversal) - surgical reconstruction or sperm retrieval for ICSI
3. Erectile Dysfunction (ED)
Definition and Epidemiology
ED = inability to obtain rigidity sufficient to permit coitus of adequate duration to satisfy both partners.
- 10-15% of all adult American men
- 52% of men aged 40-70 years have some degree of ED (Massachusetts Male Aging Study)
- Higher prevalence in type 2 diabetes mellitus and after radical prostatectomy
- Strongly associated with lower urinary tract symptoms/BPH and cardiovascular disease (shared risk factors)
Pathobiology and Causes
Categories of etiology:
| Category | Mechanism/Examples |
|---|---|
| Vasculogenic (most common) | Endothelial dysfunction, atherosclerosis; impaired penile vasodilatory capacity |
| Neurogenic | Decreased non-adrenergic, noncholinergic (NANC) nerve activity; ↓ nitric oxide (NO) production → ↓ cavernous smooth muscle relaxation → ↓ filling of cavernous sinusoids |
| Endocrine | Testosterone deficiency, hyperprolactinemia, hypo/hyperthyroidism |
| Psychological | Anxiety, depression, relationship dysfunction |
| Iatrogenic | Post-radical prostatectomy (nerve damage) |
| Drug-related | Antihypertensives (β-blockers, thiazides), antidepressants (SSRIs, TCAs), antipsychotics, antiandrogens, opioids, alcohol |
| Systemic illness | Renal failure, liver cirrhosis, chronic illness |
| Aging | Decline in endothelial function despite normal testosterone |
ED shares cardiovascular risk factors (smoking, obesity, metabolic syndrome, hyperlipidemia, type 2 DM) and mild ED should prompt cardiovascular assessment.
Diagnosis
- Detailed medical and sexual history (including partner when possible)
- Physical exam: Genitourinary, cardiovascular, endocrine (gynecomastia), neurologic, prostate exam
- Laboratory: Morning serum testosterone, PSA (if indicated), fasting glucose/HbA1c, cholesterol
- Specific diagnostic tests (penile Doppler, nocturnal penile tumescence) are rarely required in routine practice
Common drugs causing ED (Table 216-9):
- Antihypertensives (β-blockers, thiazides, clonidine)
- Antidepressants (SSRIs, TCAs)
- Antipsychotics
- Antiandrogens (finasteride, spironolactone, ketoconazole)
- Opioids, alcohol, recreational drugs
Treatment
The treatment algorithm is stepwise:
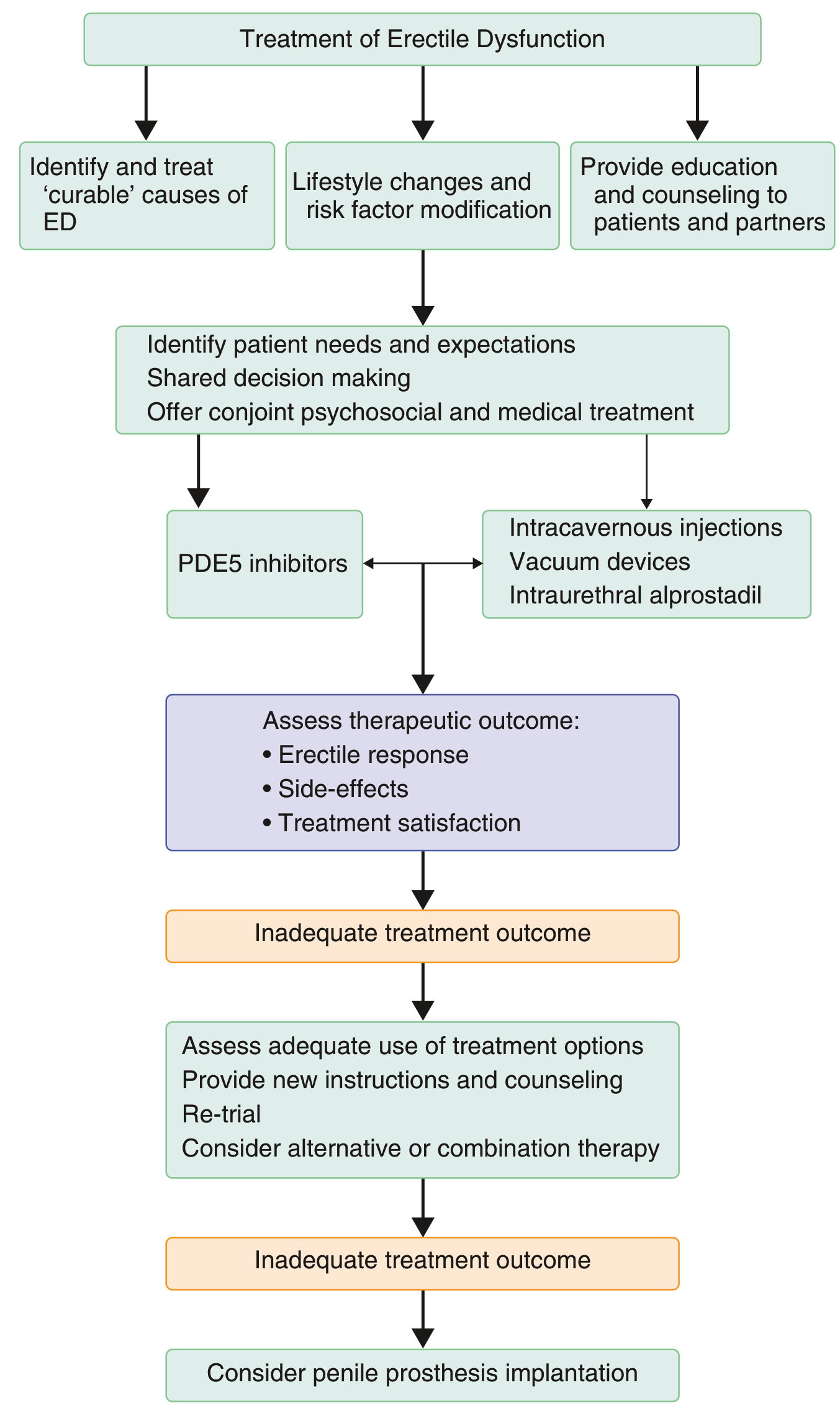
Step 1 - Address underlying causes and lifestyle:
- Treat reversible causes (correct hypogonadism, stop offending drugs, control diabetes, manage cardiovascular risk)
- Lifestyle modification: weight loss, exercise, smoking cessation, alcohol reduction
- Education and counseling to patient and partner
Step 2 (First-line) - Oral PDE5 inhibitors:
- Sildenafil, vardenafil, tadalafil - all effective in ~60% of men
- Mechanism: inhibit PDE5 → ↑ cGMP → sustained NO-mediated cavernous smooth muscle relaxation
- Absolute contraindication: Nitrates (risk of severe hypotension)
- Also caution with α-blockers (orthostatic hypotension)
- Less effective in: diabetes, post-radical prostatectomy, spinal cord injuries (but may still help)
Alternative first-line (can be offered alongside PDE5i):
- Vacuum erection devices
- Intraurethral alprostadil (prostaglandin E2 suppository, 125-1000 μg) - effective in 30-66%
- Psychosexual counseling
Step 3 (Second-line) - Intracavernosal injection:
- Alprostadil (prostaglandin E1) alone or combined with papaverine and phentolamine ("trimix")
- Injected with 27-30 gauge needle; side effects: pain, cavernosal fibrosis
- Botulinum neurotoxin (single injection) effective in ~40-50% of PDE5i-refractory patients
Emerging therapies:
- L-arginine + low-intensity shockwave therapy + PDE5i combination
- Dulaglutide (GLP-1 agonist) shown to reduce moderate-severe ED in men with type 2 DM and cardiovascular disease
Step 4 (Third-line) - Penile prosthesis implantation:
- Semi-rigid (malleable) or inflatable devices
- For men who prefer a permanent solution or are refractory to other treatments
- Long-term patient and partner satisfaction is high with proper selection
- Complications: corporal perforation, urethral injury, infection, hematoma; mechanical failure in 10-20% of inflatable devices by 10 years
Summary: Key Distinguishing Features
| Feature | Primary Hypogonadism | Secondary Hypogonadism | Male Infertility | Erectile Dysfunction |
|---|---|---|---|---|
| LH/FSH | ↑↑ | ↓ or normal | Variable | Usually normal |
| Testosterone | ↓ | ↓ | Variable | Often normal |
| Testes | Small, firm | Small, soft | Variable | Normal size |
| Classic cause | Klinefelter | Kallmann/prolactinoma | Varicocele (most common) | Vascular/DM/drugs |
| First-line Tx | Testosterone replacement | Gonadotropins or testosterone | Varicocelectomy/ART | PDE5 inhibitors |
- Goldman-Cecil Medicine International Edition, Vol. 2, Ch. 216 (pp. 2536-2544)
- Textbook of Family Medicine 9e, Ch. 35 (pp. 916-990)
Sleep apnea
Reading File
Finding Sources
Finding Sources
Searching PubMed
"sleep apnea" AND ("CPAP" OR "treatment")
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have a comprehensive set of data from Murray & Nadel (pulmonary/OSA authority), Goldman-Cecil, Guyton physiology, and Braunwald cardiology. I have enough to write a thorough clinical review with the diagnostic and treatment flowcharts. Let me compile the full answer.
Sleep Apnea: Detailed Clinical Review
Sources: Murray & Nadel's Textbook of Respiratory Medicine; Goldman-Cecil Medicine; Guyton & Hall Medical Physiology; Braunwald's Heart Disease
1. Definitions and Classification
Sleep-disordered breathing (SDB) encompasses discrete episodes of absent or reduced breathing during sleep. The three main types:
| Type | Mechanism | Key Feature on PSG |
|---|---|---|
| Obstructive Sleep Apnea (OSA) | Upper airway collapse despite continued respiratory effort | Paradoxical thoracoabdominal motion during events |
| Central Sleep Apnea (CSA) | Transient loss of CNS respiratory drive output | No respiratory effort during events |
| Mixed apnea | Begins as central, becomes obstructive | ~15% of all apneas |
Key definitions:
- Apnea: Cessation of breathing ≥10 seconds
- Hypopnea: Reduction in airflow (not complete cessation) associated with ≥3-4% O₂ desaturation and/or microarousal
- RERA (respiratory effort-related arousal): Mild upper airway narrowing with inspiratory flow flattening, not meeting hypopnea criteria, but terminating with microarousal
- AHI (apnea-hypopnea index): Number of apneas + hypopneas per hour of sleep
OSA Severity Classification (AASM)
| Severity | AHI |
|---|---|
| Normal | < 5 events/hr |
| Mild | 5-14 events/hr |
| Moderate | 15-29 events/hr |
| Severe | ≥ 30 events/hr |
2. Epidemiology
- OSA is highly prevalent - among the most common sleep disorders seen by pulmonologists
- Affects 300-500 apneic episodes per night in severe cases, with O₂ saturation dropping to ≤60%
- More common in men than women, but substantially under-recognized in women
- Prevalence increases with age, obesity, and male sex
- Women with untreated OSA have 3.5x greater risk of dying from cardiovascular disease (CVD) - normalized with appropriate CPAP treatment (Braunwald)
3. Pathogenesis
Upper Airway Collapse - The Core Mechanism
During sleep, pharyngeal dilator muscle activity decreases. In OSA patients, the upper airway collapses completely because:
- Reduced upper airway dimensions - retrognathic mandible, increased tongue/lateral wall volume, increased airway length
- High airway collapsibility (Pcrit) - measured as critical closing pressure:
- Normal: Pcrit < -10 cm H₂O
- Nonapneic snoring: Pcrit -10 to -5 cm H₂O
- Obstructive hypopnea: Pcrit -5 to 0 cm H₂O
- Obstructive apnea: Pcrit > 0 cm H₂O
- Impaired neuromuscular compensation - reduced genioglossus and other dilator muscle responses during sleep
- Fluid shift - rostral redistribution of fluid from legs to neck during recumbency (especially in heart failure, venous insufficiency)
- Reduced lung volume in recumbency - less caudal tracheal traction → reduced upper airway patency
- Airway inflammation and edema - from chronic intermittent snoring trauma and nocturnal fluid accumulation
Sequence During an Apneic Episode
- Upper airway collapses → airflow ceases
- O₂ falls, CO₂ rises progressively
- Increasing and increasingly forceful ventilatory effort (visible on PSG as paradoxical thoracoabdominal movement)
- Critical hypoxemia/hypercapnia threshold triggers arousal
- Arousal restores dilator muscle tone → airway reopens → loud snort/gasp
- Cycle repeats - 300-500 times nightly in severe cases
- Blood pressure surges at end of each apnea - can reach 240/130 mmHg transiently
Central Sleep Apnea Mechanism
- Transient abolition of CNS drive to respiratory muscles
- Causes: brainstem damage (stroke), heart failure (Cheyne-Stokes), opioids, high-loop gain respiratory instability
- Patients are extremely sensitive to sedatives/narcotics
- Treatment: Respiratory stimulants (limited), CPAP, BPAP, or ASV (adaptive servo-ventilation)
4. Risk Factors / Predisposing Factors
| Category | Examples |
|---|---|
| Obesity | Most important modifiable risk factor; fat deposition in pharyngeal soft tissues and neck compression |
| Upper airway anatomic abnormalities | Retrognathia, micrognathia, nasal obstruction, macroglossia, enlarged tonsils/adenoids, high arched palate |
| Gravity/body position | Supine position worsens OSA in up to 50% (positional OSA) |
| Genetic factors | Craniofacial structure, airway collapsibility heritability |
| Endocrine disturbances | Hypothyroidism, acromegaly (macroglossia, enlarged soft palate), PCOS |
| Smoking | Airway inflammation and edema |
| Alcohol and sedative drugs | Reduce dilator muscle tone, suppress arousal threshold |
| Male sex | Greater fat distribution in neck; hormonal differences |
| Aging | Reduced muscle tone, structural changes |
| Pregnancy | Hormonal edema, weight gain, supine position |
5. Clinical Presentation
Nocturnal Symptoms
- Loud snoring (universal in OSA; preceded by labored breathing)
- Witnessed apneas (partner reports breathing pauses)
- Choking or gasping arousals
- Nocturia
- Restless, fragmented sleep
- Diaphoresis
Daytime Symptoms
- Excessive daytime sleepiness (hallmark - measured with Epworth Sleepiness Scale)
- Morning headaches (CO₂ retention)
- Cognitive impairment - poor memory, concentration, executive function
- Mood disturbance (depression, irritability)
- Fatigue unrelieved by sleep
Epworth Sleepiness Scale (ESS)
Patients rate likelihood of dozing (0-3) in 8 situations: sitting and reading, watching TV, sitting inactive in public, as a passenger in a car, lying down in afternoon, sitting and talking, sitting after lunch, in a car in traffic. Score ≥10 = abnormal daytime sleepiness.
6. Polysomnography (PSG) - The Diagnostic Gold Standard
PSG records multiple physiological parameters simultaneously:
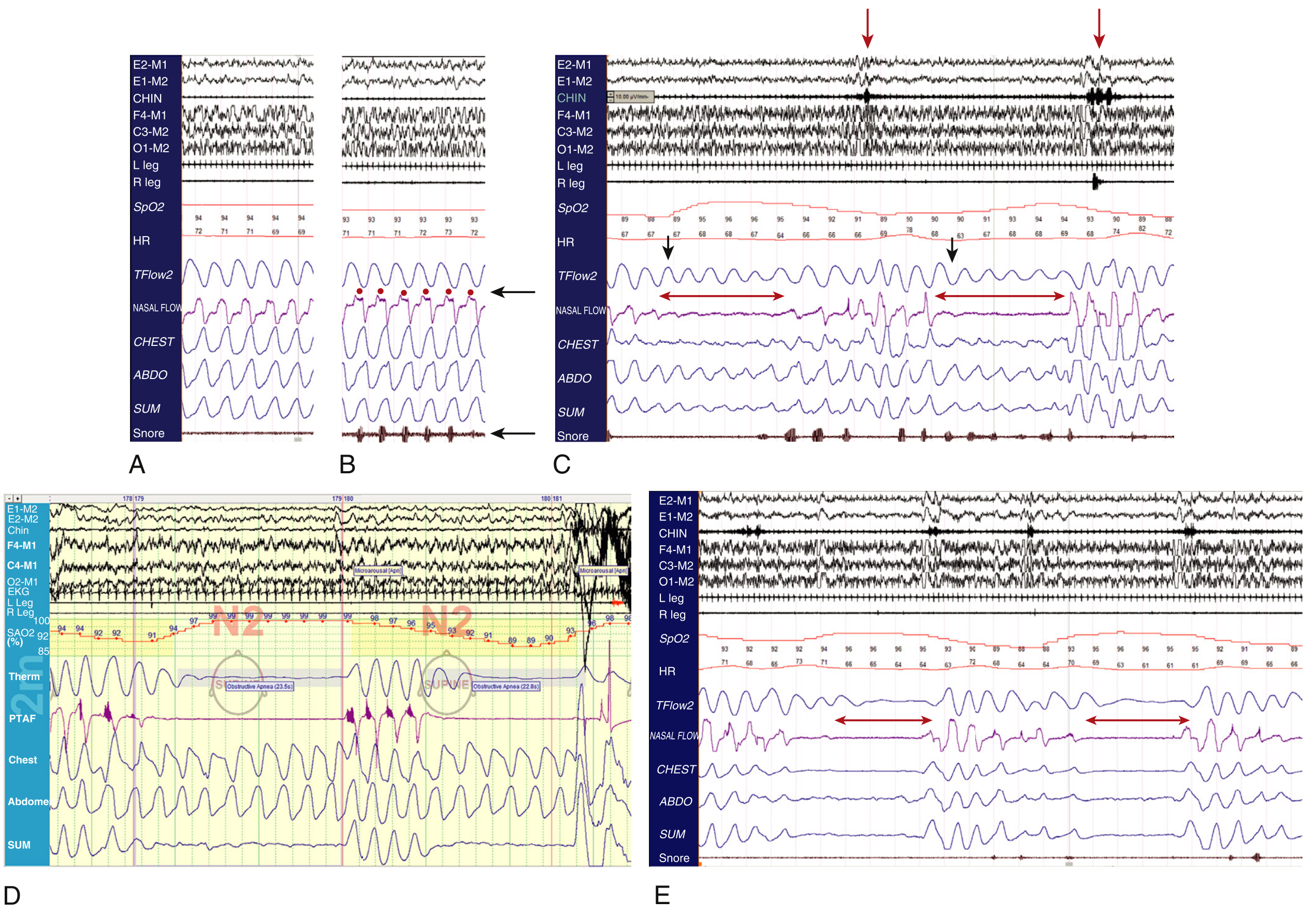
Panels: (A) Normal breathing; (B) Simple snoring with inspiratory flow flattening; (C) Obstructive hypopneas - persistent flow on thermistor but absent on nasal pressure; (D) Obstructive apneas - absent flow on both channels with paradoxical chest/abdominal motion; (E) Central apneas - absent flow with absent effort on chest and abdomen channels.
Channels recorded: EEG, EOG (eye movements), chin EMG, EKG, leg EMG, SpO₂, heart rate, airflow (thermistor + nasal pressure), thoracic and abdominal effort belts, snore microphone.
Diagnostic Testing Options
| Test | AHI | Coverage | Notes |
|---|---|---|---|
| In-lab polysomnography (PSG) | Full AHI | All channels | Gold standard; attended; best for complex/comorbid patients |
| Home sleep apnea testing (HSAT) | Respiratory event index (REI) | Reduced channels (usually no EEG) | Convenient; may underestimate severity |
| Questionnaires (STOP-BANG, Berlin) | Screening only | - | High sensitivity, low specificity |
STOP-BANG Score (≥3 high risk for OSA):
- Snoring, Tiredness, Observed apneas, Pressure (hypertension), BMI >35, Age >50, Neck >40 cm, Gender (male)
7. Consequences and Complications
Neurocognitive
- Excessive daytime sleepiness → increased motor vehicle accidents (2-7x baseline risk)
- Impaired attention, memory, executive function
- Increased depression and anxiety
Cardiovascular (Major)
- Systemic hypertension - OSA is the most common secondary cause of resistant hypertension
- Coronary artery disease - 2-3x increased risk
- Stroke - independent risk factor
- Atrial fibrillation - increased risk; OSA worsens AF recurrence after cardioversion
- Pulmonary hypertension (in severe/untreated OSA)
- Heart failure - both cause and consequence; CSA with Cheyne-Stokes breathing is common in HF
- Transient BP surges to 240/130 mmHg during apneic episodes → endothelial damage
- Increased sympathetic nervous system activity, oxidative stress, systemic inflammation
Metabolic
- Insulin resistance and type 2 diabetes (independent association)
- Obesity (bidirectional - worsens OSA, OSA worsens metabolic dysregulation)
- Non-alcoholic fatty liver disease
Other
- Nocturia (increased ANP release due to intrathoracic pressure swings)
- Erectile dysfunction (hypoxia + sympathetic activation)
- Gastroesophageal reflux (negative intrathoracic pressure)
- Pulmonary hypertension (right heart strain in severe untreated OSA)
8. Diagnosis - Approach
- History and physical exam - sleep history, BMI, neck circumference, oropharyngeal exam (Mallampati score, tonsillar size, palate), nasal patency
- Screening questionnaire - STOP-BANG or Epworth Sleepiness Scale
- Objective sleep testing before starting any therapy (to guide treatment selection)
- Home sleep apnea test (HSAT) for uncomplicated suspected OSA
- In-lab PSG for complex presentations (suspicion of CSA, hypoventilation, parasomnias, heart failure, neuromuscular disease, prior inconclusive HSAT)
- Laboratory tests: TSH (hypothyroidism), fasting glucose, consider morning cortisol if central hypoventilation
9. Treatment
The selection algorithm is shown below:
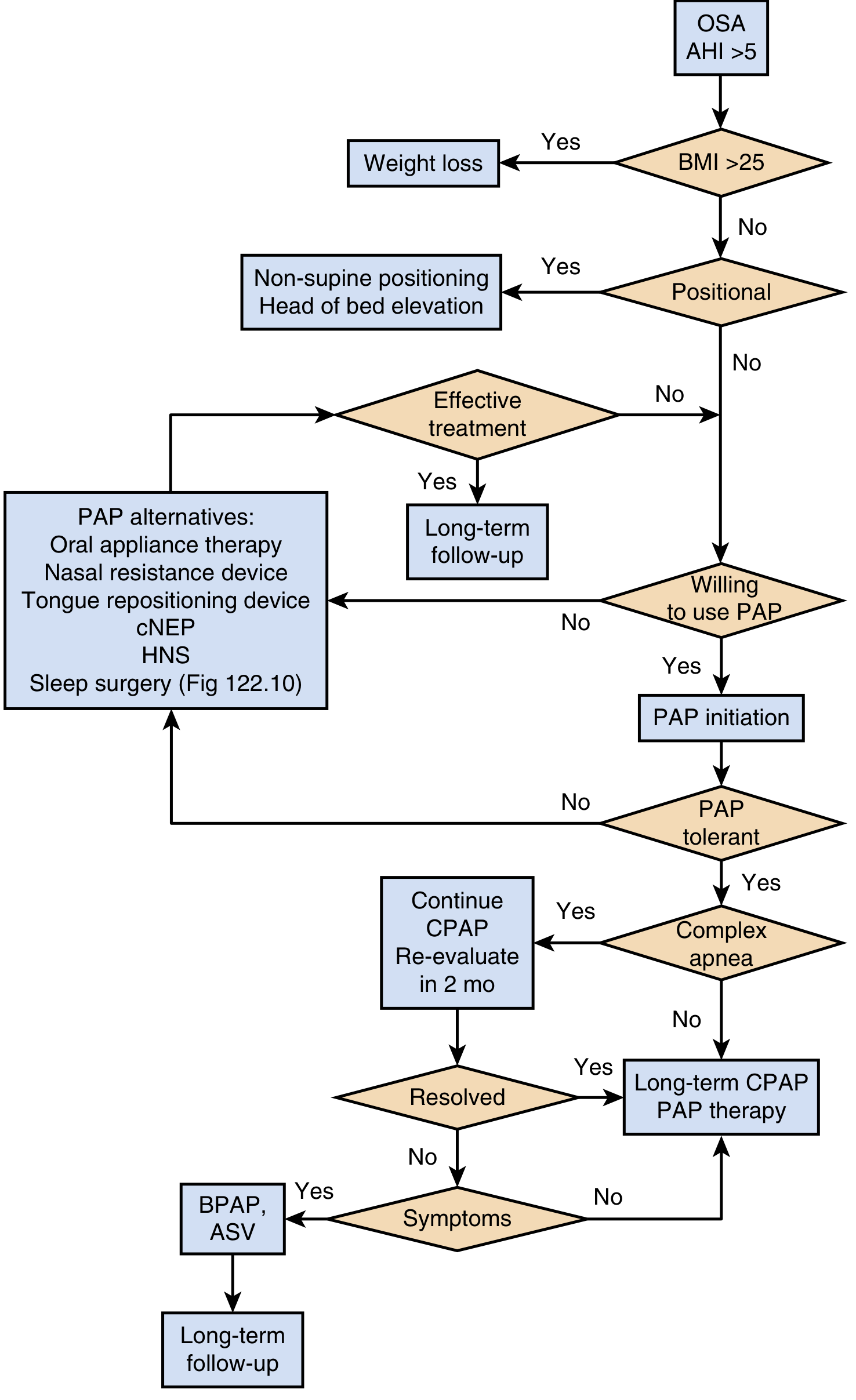
A. Behavioral and Lifestyle Modifications
- Weight loss - strongly recommended for all overweight/obese OSA patients; can resolve mild-moderate OSA with substantial loss
- Positional therapy - for positional OSA (AHI worse in supine): non-supine sleeping devices, head-of-bed elevation
- Alcohol and sedative avoidance - especially within 4 hours of sleep
- Sleep hygiene - regular sleep schedule, adequate total sleep time
B. Positive Airway Pressure (PAP) Therapy - First-Line for Moderate-Severe OSA
PAP therapy acts as a pneumatic splint, maintaining upper airway patency.
| PAP Mode | Mechanism | Indication |
|---|---|---|
| CPAP (continuous PAP) | Fixed pressure throughout breath | Standard OSA; most widely used |
| APAP (autotitrating PAP) | Automatically adjusts pressure breath-to-breath | Variable OSA severity, preferred for home titration |
| BPAP (bilevel PAP) | Separate inspiratory (IPAP) and expiratory (EPAP) pressures | High pressure needs, CPAP intolerance (aerophagia), hypoventilation |
| ASV (adaptive servo-ventilation) | Dynamically adjusts pressure support to normalize breathing | Central/complex sleep apnea, Cheyne-Stokes breathing - contraindicated in HFrEF (EF <45%) |
| VAPS (volume-assured pressure support) | Targets a set tidal volume | OHS, neuromuscular disease, central hypoventilation |
CPAP adherence is the major clinical challenge - common barriers and solutions (Table 122.3):
| Issue | Solutions |
|---|---|
| Nasal congestion | Heated humidification, nasal steroids, saline rinse, check mask leak |
| Air leaks | Mask refitting, chinstrap, adjust hose placement |
| Claustrophobia | Desensitization, low-profile mask, helmet mask |
| Aerophagia | Head-of-bed elevation, expiratory pressure relief, switch to APAP or BPAP |
| Pressure too high | Ramp feature, switch CPAP → APAP, expiratory pressure relief |
| Hesitancy/non-adherence | Education, motivational interviewing, peer support, PAP nap |
C. Oral Appliance Therapy (Mandibular Advancement Device)
- Repositions the mandible and tongue anteriorly, increasing oropharyngeal space
- Appropriate for mild-moderate OSA, or as alternative/complement to PAP
- Takes 3 months to complete evaluation + fabrication + adjustments
- Less effective than CPAP but better tolerated by some patients
- Requires intact dentition
D. Surgical Options
| Procedure | Target | Notes |
|---|---|---|
| Uvulopalatopharyngoplasty (UPPP) | Soft palate, uvula, tonsillar pillars | Most common adult sleep surgery; 50% success rate |
| Tonsillectomy/Adenoidectomy | Tonsillar/adenoid hypertrophy | Most effective surgery in children |
| Maxillomandibular advancement (MMA) | Skeletal advancement of upper + lower jaw | Highly effective (~85% success); definitive for those who fail PAP; preferred for craniofacial anatomic abnormality |
| Hypoglossal nerve stimulation (HNS) | Genioglossus activation during sleep (via implanted device) | For moderate-severe OSA, BMI <32, no concentric palatal collapse; Inspire device |
| Tracheostomy | Bypasses entire upper airway | Reserved for life-threatening severe OSA unresponsive to all other treatments |
| Nasal surgery | Nasal septal deviation, turbinate hypertrophy | Improves nasal airflow; rarely curative alone |
E. Pharmacologic Therapy
Currently no drug is FDA-approved as primary treatment for OSA, but:
- Solriamfetol and modafinil - approved for residual excessive daytime sleepiness despite adequate PAP use
- GLP-1 receptor agonists (semaglutide, tirzepatide) - substantial weight loss from these agents improves OSA severity; emerging data shows direct benefit
- Acetazolamide - useful for central apneas at high altitude; reduces loop gain
- Oxygen supplementation - may be used adjunctively in central sleep apnea or as bridge therapy
F. Special Situations
Heart failure with CSA/Cheyne-Stokes breathing:
- CPAP is beneficial
- ASV is contraindicated in HFrEF (EF <45%) - SERVE-HF trial showed increased mortality
High altitude OSA: OSA persists after ascent; acetazolamide + CPAP reduces central apneas and improves AHI
Pregnancy: Increasing OSA prevalence due to weight gain and hormonal changes; CPAP is safe and recommended
10. Central Sleep Apnea - Special Considerations
| Feature | OSA | CSA |
|---|---|---|
| Mechanism | Airway obstruction | Loss of CNS respiratory drive |
| Respiratory effort | Present (paradoxical) | Absent |
| Common causes | Obesity, anatomic | HF, opioids, stroke, high altitude |
| PSG finding | Paradoxical thoracoabdominal motion | No effort; flat chest + abdominal channels |
| Treatment | CPAP/APAP, surgery | Address cause; CPAP, BPAP, ASV (if no HFrEF) |
11. Summary: Key Clinical Pearls
- OSA is defined by AHI ≥5 with symptoms, or AHI ≥15 regardless of symptoms
- CPAP is the most effective treatment - pneumatically splints the airway open; adherence (≥4 hrs/night on ≥70% of nights) is the key measure
- Weight loss is the only potentially curative intervention for obesity-related OSA
- OSA is the most common secondary cause of resistant hypertension - always screen for it
- Untreated OSA dramatically increases cardiovascular risk - 3.5x CVD mortality in women, increased rates of MI, stroke, AF
- Never use ASV in HFrEF (EF <45%) with central/mixed sleep apnea
- Mild-moderate OSA can be managed with oral appliance therapy as an effective PAP alternative
- Hypoglossal nerve stimulation (Inspire) is an effective surgical option for selected patients who cannot tolerate PAP
- Always check for hypothyroidism and acromegaly in OSA patients resistant to standard therapy
- Murray & Nadel's Textbook of Respiratory Medicine, 2-Volume Set, Ch. 120-122
- Goldman-Cecil Medicine International Edition, Ch. 374 (Sleep Apnea) and related chapters
- Guyton and Hall Textbook of Medical Physiology, Ch. on Breathing Control
- Braunwald's Heart Disease, Ch. 14 (Sleep Apnea and Cardiovascular Disease)
This is a shared conversation. Sign in to Orris to start your own chat.