Acetylcystine vs acebrophylline
Reading File
Finding Sources
Finding Sources
Searching PubMed
acetylcysteine acebrophylline mucolytic COPD comparison
Reading File
Reading File
Finding Sources
Searching PubMed
acebrophylline COPD asthma
Reading Article
PMID: 40454226
Finding Sources
Reading File
Finding Sources
Finding Sources
Searching the Web
acebrophylline mechanism of action mucolytic bronchodilator pharmacology
Finding Sources
Reading File
Here is a detailed comparison of Acetylcysteine (NAC) vs Acebrophylline:
Acetylcysteine (N-Acetylcysteine / NAC) vs Acebrophylline
1. Drug Identity
| Feature | Acetylcysteine (NAC) | Acebrophylline |
|---|---|---|
| Class | Mucolytic / Antioxidant / Antidote | Mucoregulator + Bronchodilator (combination) |
| Composition | Single agent - N-acetyl derivative of L-cysteine | Fixed combination of Ambroxol + Theophylline-7-acetate |
| Category | Pure mucolytic with antioxidant properties | Dual-action: mucolytic + xanthine bronchodilator |
2. Mechanism of Action
Acetylcysteine:
- Cleaves disulfide bonds in mucus glycoproteins, directly reducing mucus viscosity and gel structure
- Donates cysteine for glutathione synthesis, making it a powerful antioxidant
- Protects against oxidative stress, which is especially relevant in COPD where cigarette smoke depletes glutathione
- Additional mechanism: replenishes glutathione stores to protect hepatocytes in paracetamol overdose
Acebrophylline:
- Ambroxol component:
- Stimulates synthesis and secretion of pulmonary surfactant (type II pneumocytes), liquefying the sol phase of mucus
- Increases ciliary motility, enhancing mucociliary clearance
- Reduces gel-phase viscosity without directly cleaving bonds
- Anti-inflammatory: reduces TNF-alpha and leukotriene release
- Theophylline-7-acetate component:
- Inhibits phosphodiesterase (PDE), raising intracellular cAMP
- Causes bronchial smooth muscle relaxation (bronchodilation)
- Selectively inhibits phosphatidylcholine and phospholipase A
- Anti-inflammatory at low doses (histone deacetylase activation)
- Net effect: Acebrophylline shows 45% improvement in lung health vs ambroxol alone, due to synergism of its two components
3. Pharmacological Actions Summary
| Action | Acetylcysteine | Acebrophylline |
|---|---|---|
| Mucolytic (direct) | Yes - breaks disulfide bonds | Yes - via ambroxol (surfactant ↑, sol phase ↑) |
| Bronchodilation | No | Yes - via theophylline moiety (PDE inhibition) |
| Antioxidant | Yes (major effect, GSH precursor) | Mild (ambroxol has some antioxidant properties) |
| Anti-inflammatory | Yes (indirect via GSH) | Yes (inhibits TNF-alpha, leukotrienes) |
| Surfactant stimulation | No | Yes (ambroxol) |
| Mucociliary clearance | Modest | Strong (ambroxol enhances ciliary beat) |
4. Indications
Acetylcysteine:
- COPD - reducing exacerbation frequency (especially at 600 mg twice daily; supported by PANTHEON trial in moderate-severe COPD)
- Chronic bronchitis / viscous secretions in cystic fibrosis
- Paracetamol (acetaminophen) overdose - hepatoprotective (IV form)
- Contrast-induced nephropathy prevention (IV/oral)
- Nebulized form for thinning airway secretions in ICU / post-op
- Vernal keratoconjunctivitis (topical - dissolves mucus filaments)
Acebrophylline:
- COPD (add-on therapy, especially when bronchospasm co-exists with hypersecretion)
- Bronchial asthma (particularly when inhaler therapy is not preferred or as add-on to ICS/LABA)
- Acute/chronic bronchitis with both secretion problems and airway obstruction
- Preferred in patients needing simultaneous mucolysis and bronchodilation in a single oral tablet
5. Clinical Evidence
Acetylcysteine:
- The PANTHEON study established NAC (600 mg BD) as useful in moderate-severe COPD, significantly reducing exacerbation rates
- Fishman's Pulmonary Diseases notes that NAC "does not alter the decline in FEV1" but "may have a role in reducing exacerbations" - Murray & Nadel's confirms a "small reduction in number of exacerbations" with "small improvement in cough, decrease in volume of sputum"
Acebrophylline:
- The CARE study (2025) - a prospective post-marketing surveillance study of the NAC + Acebrophylline combination ("Abiways") in 97 patients with moderate-severe COPD and asthma - showed FEV1 improved from 1.287L to 1.484L (p<0.001), and COPD CAT scores improved from 17.2 to 10.6 (p=0.0001). No severe adverse events were reported. (PMID 40454226)
- A separate study (PMC4225926) comparing acebrophylline vs sustained-release theophylline in COPD found acebrophylline better tolerated with equivalent or superior bronchodilatory and mucociliary effects
6. Dosing
| Acetylcysteine | Acebrophylline | |
|---|---|---|
| Oral | 200 mg TDS or 600 mg OD/BD (effervescent) | 100 mg BD |
| Inhaled/Nebulized | 3-5 mL of 10-20% solution | Not available |
| IV | Used in paracetamol OD (Rumack-Matthew protocol) | Not available |
7. Adverse Effects
Acetylcysteine:
- Oral: nausea, vomiting, stomatitis, bad odor
- IV: anaphylactoid reactions (flushing, bronchospasm, hypotension) - more common with rapid infusion
- Inhaled: bronchospasm (especially in asthmatics - always give with bronchodilator)
Acebrophylline:
- Generally well tolerated (better tolerated than theophylline alone due to lower theophylline dose)
- Nausea, headache, palpitations (theophylline-related)
- Theophylline-related toxicity at high doses (narrow therapeutic index concern, though acebrophylline uses the acetate form which is considered safer)
8. Key Differentiating Points
- NAC is the only one with non-respiratory indications - it is a life-saving antidote for paracetamol overdose and a renal protectant for contrast nephropathy
- Acebrophylline adds bronchodilation - NAC has no bronchodilatory effect; acebrophylline is preferred when airway obstruction co-exists with mucus hypersecretion
- NAC is the stronger antioxidant - important in COPD pathogenesis driven by oxidative stress
- Acebrophylline stimulates surfactant - useful in conditions where alveolar stability is impaired
- Both can be combined - the CARE study (2025) shows NAC + Acebrophylline together improve both QoL and FEV1 in COPD and asthma, suggesting complementary (not redundant) mechanisms
- NAC has inhaled/IV forms; acebrophylline is oral only
Bottom line: NAC is a simpler, older, better-studied agent with uses well beyond the respiratory tract. Acebrophylline is a dual-action respiratory-specific agent that addresses both obstruction and secretion problems simultaneously. In clinical practice, they can be used together as complementary agents in obstructive airway disease.
- Murray & Nadel's Textbook of Respiratory Medicine, Expectorants and Mucolytics section
- Fishman's Pulmonary Diseases and Disorders, Chronic Maintenance Therapy section
- K.J. Lee's Essential Otolaryngology, Mucolytics and Expectorants section
- Dhar R et al., CARE Study, J Asthma Allergy 2025 (PMID 40454226)
Explain Rumack Matthew protocol
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Now I have comprehensive information. Here is the full explanation:
The Rumack-Matthew Protocol (Nomogram)
Background
The Rumack-Matthew nomogram was originally published by Rumack BH and Matthew H in Pediatrics (1975;55:871). It was derived from a retrospective analysis of oral paracetamol (acetaminophen / APAP) overdose patients and their clinical outcomes. It remains the standard tool for risk-stratifying acute paracetamol poisoning and guiding treatment with N-acetylcysteine (NAC).
Why Paracetamol is Hepatotoxic in Overdose
Under normal circumstances, paracetamol is metabolized mainly by glucuronidation and sulfation to non-toxic conjugates. A small fraction goes through CYP450 (mainly CYP2E1) to form NAPQI (N-acetyl-p-benzoquinoneimine), a highly reactive toxic metabolite, which is rapidly detoxified by hepatic glutathione.
In overdose:
- Glucuronidation and sulfation pathways become saturated
- A much larger fraction is shunted to CYP450 → massive NAPQI production
- When hepatic glutathione stores fall below 30% of normal, NAPQI binds covalently to hepatic macromolecules
- This causes centrilobular hepatic necrosis
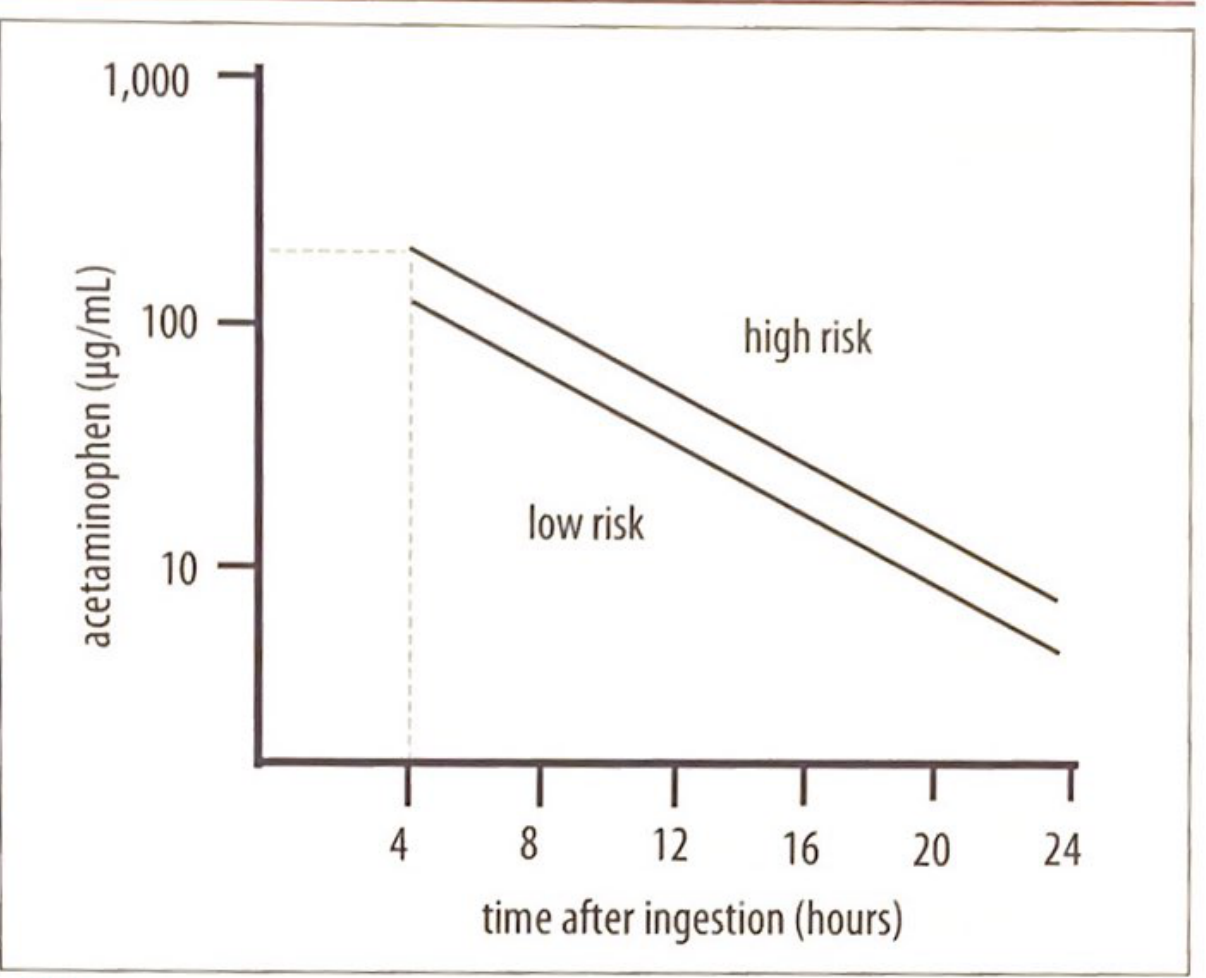
How the Nomogram Works
The nomogram is a semilogarithmic plot of:
- Y-axis: Serum paracetamol concentration (µg/mL) - on a log scale
- X-axis: Time after ingestion (hours, from 4 to 24 hours) - linear scale
Two parallel declining lines define risk zones:
| Zone | Original line | Modified/Treatment line | Risk |
|---|---|---|---|
| Above upper line | >200 µg/mL at 4h | Probable toxicity | ~60% risk of hepatotoxicity |
| Between lines | Possible toxicity | Intermediate | |
| Below lower line | Low/no risk | NAC not needed |
The modified treatment line (the one used in practice) starts at a 4-hour concentration of 150 µg/mL (1000 µmol/L) - this was lowered from the original 200 µg/mL to build in a safety margin. In the US, only this single treatment line is used (below = safe, above = treat).
The nomogram stratifies patients into 3 groups (per Quick Compendium of Clinical Pathology):
- Probable hepatic toxicity
- Possible hepatic toxicity
- No hepatic toxicity
Rules for Using the Nomogram
When it APPLIES:
- Single acute oral ingestion
- Ingestion time is accurately known
- Sample drawn between 4 and 24 hours after ingestion
When it DOES NOT APPLY (Washington Manual / Tintinalli's):
- Chronic or repeated supratherapeutic ingestion
- Staggered ingestion over several hours
- Extended-release paracetamol formulations
- Levels drawn before 4 hours (no prognostic value)
- Levels drawn after 24 hours
For patients with uncertain timing, staggered, or chronic ingestion - treat empirically with NAC
Four Clinical Stages of Toxicity (Tintinalli's)
| Stage | Timing | Clinical Features | Lab Changes |
|---|---|---|---|
| Stage 1 | First 24 h | Anorexia, nausea, vomiting, malaise (or asymptomatic) | None |
| Stage 2 | Days 2-3 | GI symptoms improve; RUQ pain, hepatic tenderness | ALT/AST rise, ↑bilirubin, ↑PT if severe |
| Stage 3 | Days 3-4 | GI symptoms recur; encephalopathy, jaundice, anuria | Fulminant hepatic failure, metabolic acidosis, coagulopathy, renal failure |
| Stage 4 | After day 5 | Recovery OR multiorgan failure and death | Normalization OR continued deterioration |
Treatment: N-Acetylcysteine (NAC)
Mechanism: NAC replenishes glutathione by donating cysteine, allowing NAPQI to be conjugated and safely excreted. It also promotes the glucuronidation and sulfation pathways directly.
NAC is most effective if started within 8-10 hours of ingestion but should still be given up to 24 hours post-ingestion. It is indicated whenever the serum level plots above the treatment line.
IV NAC Protocol (21-hour regimen - standard US protocol):
| Phase | Dose | Duration |
|---|---|---|
| Loading dose | 150 mg/kg | Over 1 hour |
| 1st maintenance | 50 mg/kg | Over 4 hours |
| 2nd maintenance | 100 mg/kg | Over 16 hours |
| Total | 300 mg/kg | 21 hours |
Oral NAC Protocol (72-hour regimen):
- Loading dose: 140 mg/kg
- Maintenance: 70 mg/kg every 4 hours for 17 further doses
- Used when IV route not available, or in patients at high risk for anaphylactoid reactions (e.g., asthmatics)
Key side effect of IV NAC: Anaphylactoid reactions (4-17%), mostly in the first 2 hours; higher risk in asthmatics. Treat with diphenhydramine and temporarily stop/slow infusion.
King's College Criteria (for Transplant Evaluation)
When a patient develops hepatic failure despite treatment, prognosis is assessed with King's College Hospital (KCH) criteria. Transplant listing is considered if:
- pH < 7.3 (after resuscitation)
- OR all three of: PT >100 sec + creatinine >300 µmol/L + Grade III-IV encephalopathy
Limitations of the Nomogram
- Only valid for acute single ingestion - not chronic use
- Requires accurate time of ingestion
- Not valid for levels drawn before 4 hours
- Does not account for enzyme inducers (e.g., chronic alcohol, rifampicin, anticonvulsants) which increase CYP2E1 activity and NAPQI generation - these patients may have toxicity at lower plasma levels
- Extended-release formulations may have delayed peaks; a second level at 4-6 hours later is recommended if the first plots below the line
Sources: Tintinalli's Emergency Medicine, Chapter 190; Washington Manual of Medical Therapeutics, Chapter 28; Quick Compendium of Clinical Pathology; Harriet Lane Handbook (Rumack-Matthew nomogram figure)
This is a shared conversation. Sign in to Orris to start your own chat.