Fibromyalgia , diagnostic criteria and notes as per harrison
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
I now have all the information needed for a complete answer. Let me compile the full response from Harrison's 22E.
Fibromyalgia - Diagnostic Criteria & Clinical Notes
Harrison's Principles of Internal Medicine, 22nd Edition (2025), Chapter 385
Definition
Fibromyalgia (FM) is characterized by chronic widespread musculoskeletal pain and tenderness. It is defined primarily as a pain syndrome, but patients also commonly report associated neuropsychological symptoms: fatigue, unrefreshing sleep, cognitive dysfunction, anxiety, and depression. Available evidence implicates the central nervous system as the key driver of pain and other core symptoms. FM is part of the broader group of chronic overlapping pain conditions (also including myalgic encephalitis/chronic fatigue syndrome, temporomandibular disorder, irritable bowel syndrome, interstitial cystitis, and other pelvic pain syndromes).
Epidemiology
- Worldwide prevalence ~2%; ~4% in women, <1% in men
- Female:male ratio in clinical settings ~8:1; in population studies ~3:1
- Prevalence rises to 10-30% in patients with rheumatic diseases (RA, SLE), likely because these serve as peripheral pain generators
- Over 5 million Americans affected
- Additional risk factors: sleep disturbance, physical inactivity, overweight/obesity
2016 Diagnostic Criteria (Wolfe et al., revised from 2010/2011)
All three of the following must be met:
Criterion 1 - Widespread Pain Index (WPI) + Symptom Severity Score (SSS):
WPI ≥ 7 AND SSS ≥ 5 OR WPI 4-6 AND SSS ≥ 9
Criterion 2 - Generalized pain in at least 4 of 5 regions (jaw/neck/chest/abdomen count as axial)
Criterion 3 - Symptoms present at a similar level for at least 3 months
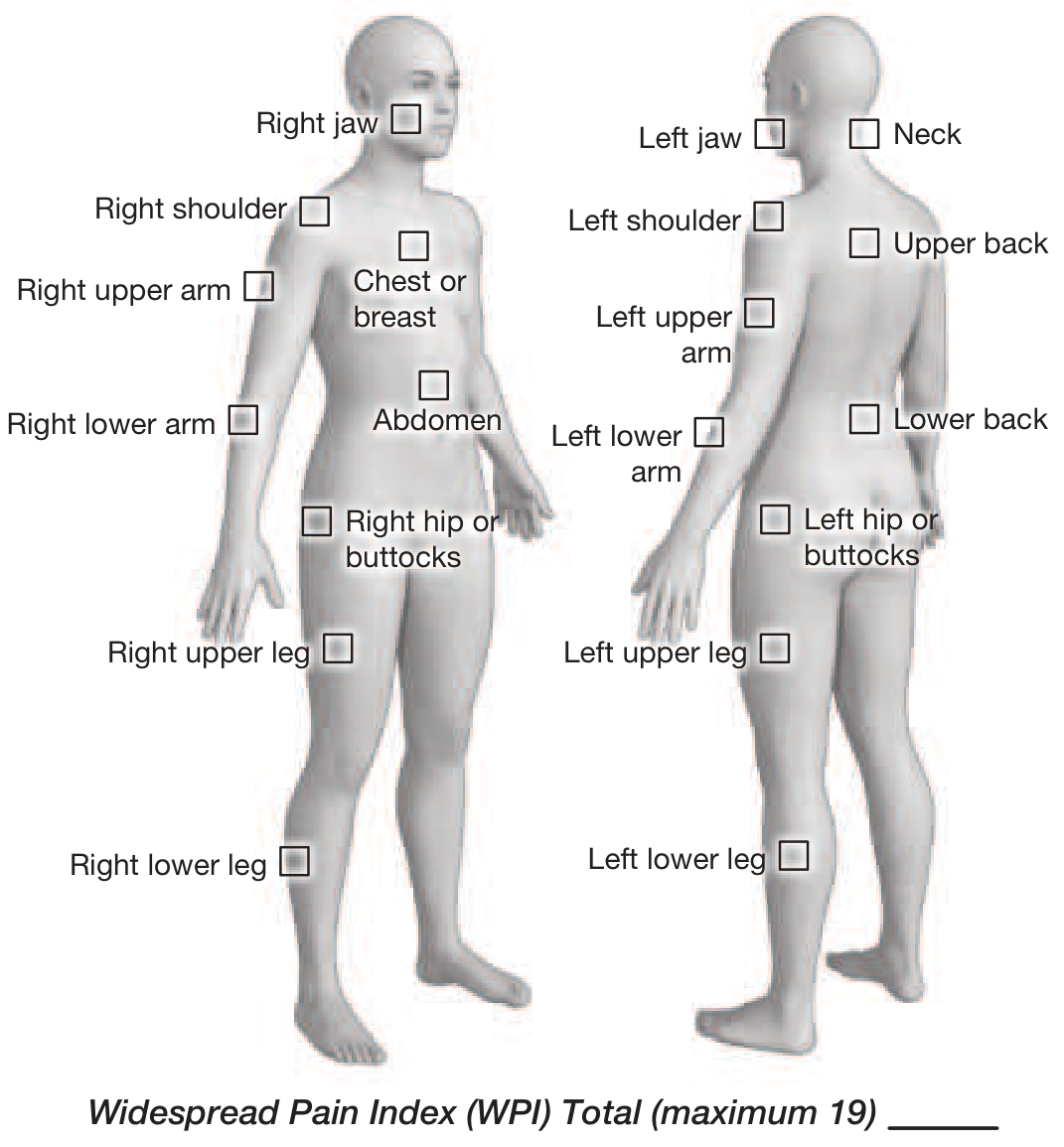
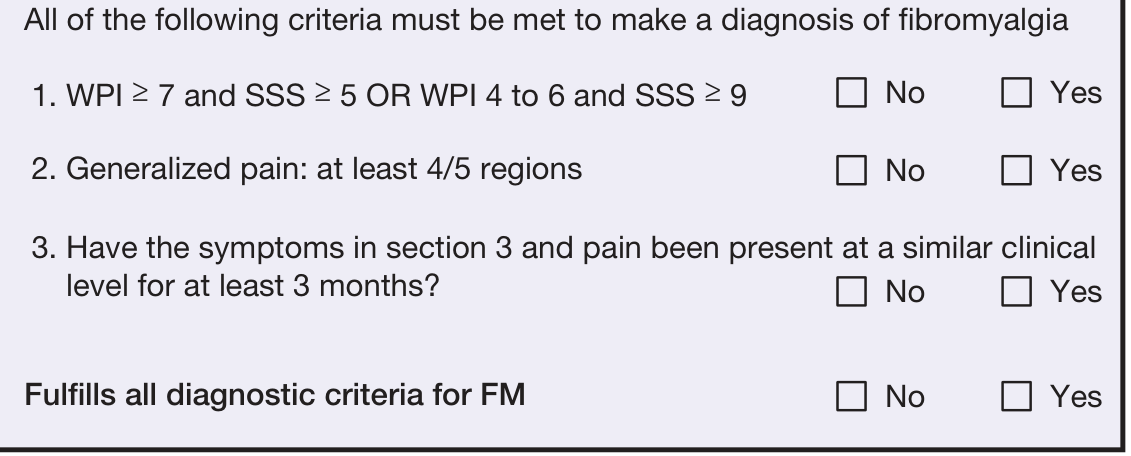
FIGURE 385-1, Harrison's 22E - FM 2016 Diagnostic Criteria
Widespread Pain Index (WPI) - Scoring (max 19)
The patient indicates where they had pain during the past week from the following 19 regions:
| Side | Regions |
|---|---|
| Right | Jaw, Shoulder, Upper Arm, Lower Arm, Hip/Buttocks, Upper Leg, Lower Leg |
| Left | Jaw, Shoulder, Upper Arm, Lower Arm, Hip/Buttocks, Upper Leg, Lower Leg |
| Axial | Neck, Chest/Breast, Abdomen, Upper Back, Lower Back |
Symptom Severity Score (SSS) - Scoring (max 12)
Part A - Over the past week (0 = no problem, 1 = slight/mild, 2 = moderate, 3 = severe):
- Fatigue (0-3)
- Trouble thinking or remembering (0-3)
- Waking up tired/unrefreshed (0-3)
Part B - During the past 6 months (Yes = 1, No = 0):
- Pain or cramps in the abdomen
- Depression
- Headache
SSS total = Part A (0-9) + Part B (0-3) = 0-12
Clinical Manifestations
Pain and Tenderness
- Patients report "pain all over" - poorly localized, severe, with reduced function
- Widespread pain = both above and below the waist, both sides of the body, involving the axial skeleton (neck, back, or chest)
- Pain present most of the day on most days for ≥ 3 months (required for diagnosis)
- Associated tenderness and elevated evoked pain sensitivity (hyperalgesia, allodynia)
- The older 1990 ACR criteria required ≥ 11 of 18 tender points at ~4 kg/m² pressure (thumbnail blanching pressure) - this is no longer required by current criteria
Neuropsychological Symptoms
- Fatigue (often profound)
- Unrefreshing sleep
- Cognitive dysfunction ("fibro fog")
- Anxiety and depression
Overlapping Syndromes
- Headaches, facial/jaw pain, regional myofascial pain
- Visceral pain: GI, bladder, pelvic/perineal
- Importantly, FM often coexists with other overlapping conditions and treatment of one may help global symptom management
Differential Diagnosis (Table 385-1)
| Category | Conditions |
|---|---|
| Inflammatory | Polymyalgia rheumatica, RA, spondyloarthritides, SLE, Sjögren's syndrome |
| Infectious | Hepatitis C, HIV, Lyme disease, Parvovirus B19, EBV |
| Noninflammatory | Degenerative joint/spine/disk disease, myofascial pain syndrome, bursitis, tendinitis |
| Endocrine | Hypothyroidism, hyperthyroidism, hyperparathyroidism |
| Neurologic | Multiple sclerosis, neuropathic pain syndromes |
| Psychiatric | Major depressive disorder |
| Drugs | Statins, aromatase inhibitors |
Laboratory & Radiographic Testing (Table 385-2)
Routine (all FM patients):
- ESR or CRP
- CBC
- TSH
Guided by History and Physical Exam:
- Complete metabolic panel
- ANA
- Anti-SSA and anti-SSB
- RF and anti-CCP
- Creatine phosphokinase (CPK)
- Viral/bacterial serologies (Hep C, HIV, Lyme)
- Spine and joint radiographs (only if inflammatory arthritis features present)
Key note: Routine labs and imaging are normal in uncomplicated FM. MRI of the spine should be discouraged unless there are features of inflammatory spine disease or neurologic symptoms. Repeat testing after initial evaluation is also discouraged.
Pathogenesis
- Genetic predisposition: polymorphisms in pathways controlling serotonin and monoamine metabolism/transport, and other pain transmission pathways
- Psychophysical testing shows altered sensory afferent pain processing and impaired descending noxious inhibitory control → hyperalgesia and allodynia
- Functional MRI demonstrates brain activation in pain-processing regions in response to innocuous stimuli
- Pain perception modulated by emotional/cognitive factors (catastrophizing, perceptions of control) - basis for CBT recommendations
- Some patients may have small fiber neuropathy; early reports suggest possible autoimmune etiology in a subset
- Potential future: confirmatory diagnostic testing from gene expression or metabolic signatures in peripheral blood
Treatment
Nonpharmacologic (first-line, most effective)
- Physical conditioning/aerobic exercise - consistently the most helpful intervention; start low, advance slowly
- Supervised or water-based programs for deconditioned patients
- Strength training after aerobic goals achieved
- FDA-approved devices: laser therapy device; TENS (large RCT showed reduction in movement-evoked pain and fatigue)
- Meditative movement: qigong, yoga, Tai Chi
- Acupuncture, hydrotherapy
- Cognitive-behavioral therapy (CBT) for sleep hygiene and illness behaviors
- Patient education about genetics, triggers, and physiology of FM
Pharmacologic (Table 385-3)
| Drug | Dose |
|---|---|
| Cyclobenzaprine (muscle relaxant) | 10-40 mg/day, at bedtime or divided up to 4x/day |
| Amitriptyline (TCA, SNRI activity) | 10-50 mg/day at bedtime |
| Duloxetine (SNRI) - FDA approved | 60 mg/day; start at 30 mg/day for 1 week |
| Milnacipran (SNRI) - FDA approved | 50 mg BID; titrate over 7 days |
| Pregabalin (α2-δ ligand) - FDA approved | 150-450 mg/day; start 75 mg BID ≥ 1 week |
| Tramadol | 37.5 mg + 325 mg acetaminophen up to 4x/day |
Key prescribing notes:
- NSAIDs and glucocorticoids may treat inflammatory triggers but are not effective for FM symptoms
- Strong opioids are to be avoided - no demonstrated efficacy and worsen symptoms/function
- Tramadol: generally discouraged due to opioid-related adverse effects despite some evidence
- Choose agents that address multiple symptom domains simultaneously:
- Pain + sleep disturbance → cyclobenzaprine, amitriptyline, gabapentin, pregabalin
- Pain + fatigue/anxiety/depression → duloxetine or milnacipran
Approach to the Patient
- Optimal management requires prompt diagnosis + assessment of pain, function, and psychosocial context
- Developing a patient-clinician partnership is essential
- Focus on improved function and quality of life, not elimination of pain
- Discourage illness behaviors (frequent physician visits); encourage function-focused behaviors
- Identify and treat comorbid triggering conditions separately
Source: Harrison's Principles of Internal Medicine, 22nd Edition (2025), Chapter 385 (Fibromyalgia) and Chapter 382 (Approach to the Patient with Musculoskeletal Disease).
This is a shared conversation. Sign in to Orris to start your own chat.