Postpartum Complications: Sepsis, hematoma, Mastitis, UTI, DVT, Psychological
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Postpartum Complications
The puerperium spans 6 weeks after delivery. Several complications can arise during this period; early recognition and prompt management are the cornerstones of care.
1. Puerperal Sepsis
Definition: Infection of the genital tract within 3 weeks after delivery.
Clinical features:
- Pyrexia (fever) and tachycardia
- Foul-smelling lochia
- Pain and tenderness in the lower abdomen
- The most common organism is Streptococcus pyogenes (Group A beta-hemolytic streptococcus), which can cause endometritis and bacteremia. Staphylococci and anaerobes are also implicated.
Pathophysiology: Streptococci enter the uterus after delivery, infecting the wound (endometritis), and can progress to septicemia.
Prevention: Strict asepsis before, during, and after delivery - especially important in domiciliary (home) midwifery services.
Management:
- Blood cultures + wound swabs
- Broad-spectrum IV antibiotics (e.g., IV amoxicillin-clavulanate ± metronidazole; clindamycin + gentamicin)
- Sepsis bundle: IV fluids, monitoring lactate, organ support as needed
- Source control (e.g., evacuation of retained products if endometritis)
- Park's Textbook of Preventive and Social Medicine
- Jawetz Melnick & Adelberg's Medical Microbiology 28E
2. Postpartum Hematoma
Definition: A collection of blood in the connective tissue spaces of the genital tract following delivery, usually within 24 hours.
Sites:
- Vulval hematoma - most common; below the pelvic floor
- Paravaginal hematoma - above the pelvic floor, extends into the broad ligament
- Broad ligament hematoma - serious; can be life-threatening
Causes:
- Injury to blood vessels during delivery without a corresponding laceration of the overlying mucosa
- Episiotomy or perineal tear with poor hemostasis
- Instrumental delivery (forceps)
- Bleeding diatheses
Clinical features:
- Severe vulval pain and pressure sensation
- Visible or palpable tense, fluctuant swelling
- Bluish discoloration of the perineum/vulva
- Tachycardia and hypotension if large
Management:
- Small hematoma (< 4 cm, stable): Conservative - ice packs, analgesia, observation
- Large/expanding hematoma: Surgical incision, evacuation of clot, suture of bleeding points, vaginal packing
- Blood transfusion if significant blood loss
- Antibiotics to prevent secondary infection
3. Mastitis
Definition: Inflammation of the breast parenchyma, most common in the second postpartum week, due to milk stasis and retrograde bacterial infection.
Epidemiology: Affects ~1/3 of breastfeeding women in the US; progresses to breast abscess in up to 10% of cases. - Red Book 2021
Causative organisms:
- Staphylococcus aureus (40% of cases) - most common
- Escherichia coli
- Streptococcus species
- Community-acquired MRSA must be considered
Clinical features:
- Severe pain, tenderness, swelling, redness of the breast (usually unilateral, one segment)
- Fever, chills, myalgias
- Flu-like systemic symptoms
Differentials: Breast engorgement, plugged duct, inflammatory breast carcinoma (rare but important)
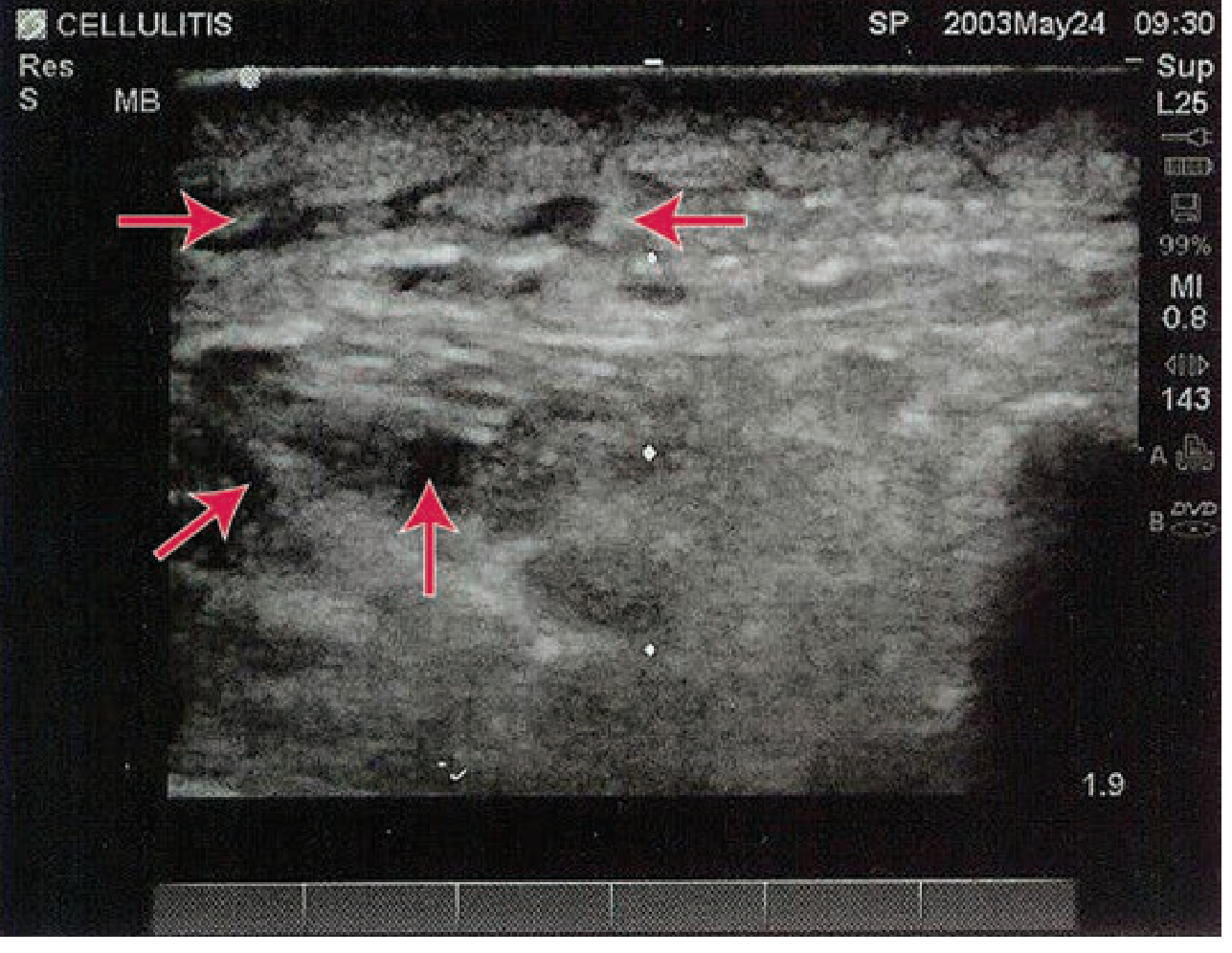
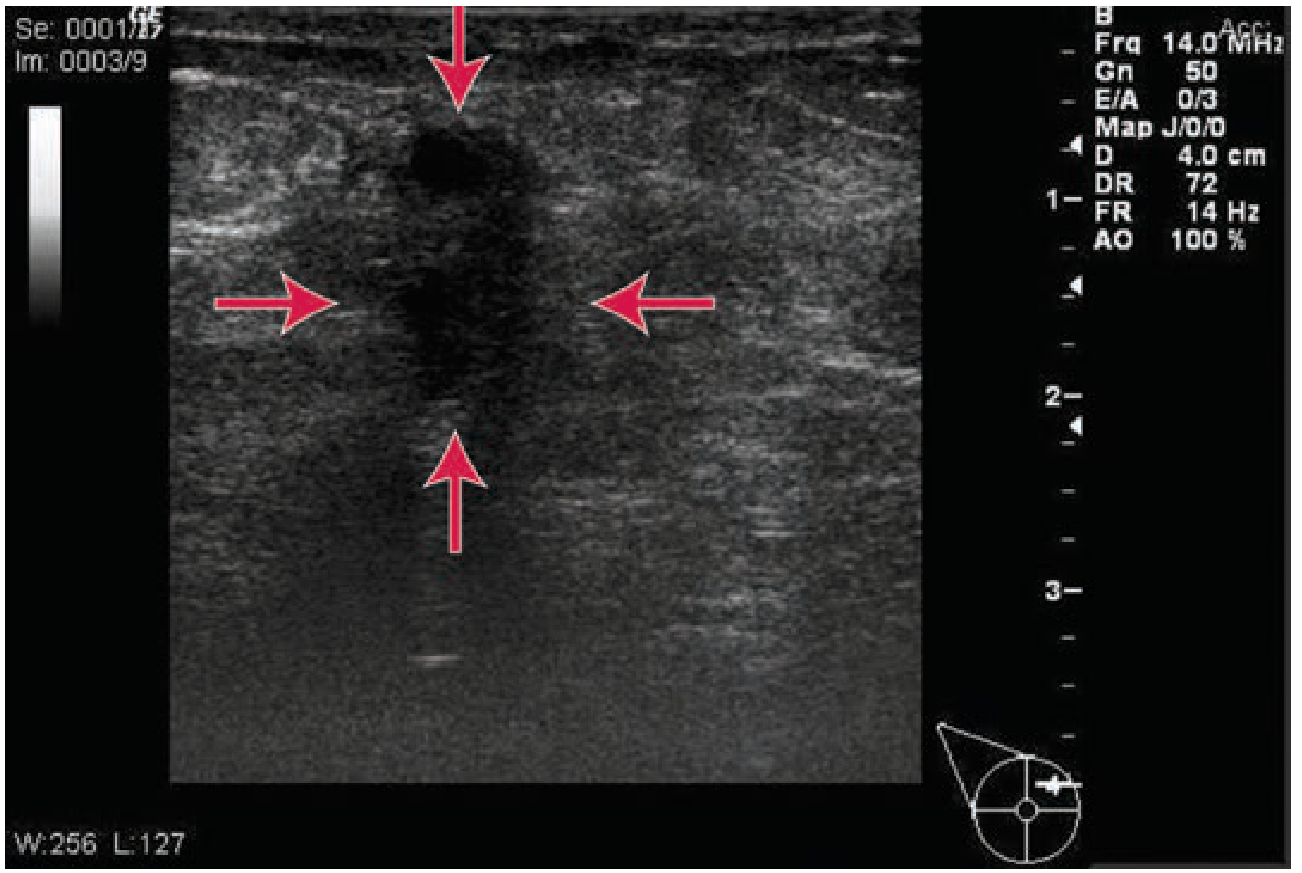
Ultrasound findings:
- Mastitis: hypoechoic fluid surrounding subcutaneous fat lobules, no discrete fluid collection
- Abscess: discrete hypoechoic fluid collection with absent vascular signals
Management:
- Do NOT stop breastfeeding (or pumping) - continued emptying is therapeutic
- Frequent analgesia (NSAIDs/paracetamol)
- Antibiotics: antistaphylococcal penicillins (dicloxacillin/flucloxacillin) or 1st-generation cephalosporins
- Note: Sulfamethoxazole-trimethoprim is contraindicated in lactating mothers with infants < 2 months old
- If no improvement in 48 hours: assess for abscess with ultrasound
- Breast abscess: ultrasound-guided aspiration/drainage preferred; surgical drainage reserved as last resort (risk of milk fistula); IV vancomycin for septic inpatients
- Tintinalli's Emergency Medicine
4. Urinary Tract Infection (UTI)
Context: One of the most common postpartum infections. Predisposing factors are unique to the puerperium.
Risk factors:
- Bladder overdistension and incomplete emptying postpartum
- Urinary catheterization during labor
- Perineal trauma and local contamination
- Epidural analgesia (reduces awareness of bladder fullness)
- Residual urine from uterine pressure
Causative organisms: E. coli (most common), Klebsiella, Enterococcus, Proteus
Clinical features:
- Dysuria, frequency, urgency
- Suprapubic tenderness
- If ascending to kidneys (pyelonephritis): high fever, rigors, flank/loin pain, vomiting
Management:
- Urine culture and sensitivity (midstream clean-catch)
- Encourage high fluid intake
- Uncomplicated cystitis: 3-7 day course of antibiotics - nitrofurantoin (avoid if breastfeeding), trimethoprim, cefalexin (note: TMP-SMX avoided in first 6 weeks if breastfeeding)
- Pyelonephritis: IV cephalosporins or aminoglycosides, then oral step-down
- Remove/change urinary catheter early
- Park's Textbook of Preventive and Social Medicine
5. Deep Vein Thrombosis (DVT) / Thrombophlebitis
Why postpartum women are high risk (Virchow's triad is fully activated):
| Factor | Postpartum Change |
|---|---|
| Stasis | Immobility, bed rest, prolonged labor |
| Hypercoagulability | Elevated clotting factors, decreased protein S, increased fibrinogen |
| Endothelial injury | Pelvic/perineal trauma, C-section |
Peak risk period: First 6 weeks postpartum; risk is highest in the first 2 weeks. Risk is 5-10x higher than in non-pregnant women.
Clinical features (superficial/DVT):
- Leg becomes tender, pale, and swollen ("white leg" or phlegmasia alba dolens if severe)
- Calf tenderness, warmth, erythema
- Positive Homans' sign (limited diagnostic value)
- Frequently associated with varicose veins
Diagnosis:
- Wells score clinical probability assessment
- D-dimer (high sensitivity, low specificity postpartum)
- Compression duplex ultrasonography - first-line imaging
- CT pulmonary angiography if pulmonary embolism suspected
Management:
- Low Molecular Weight Heparin (LMWH) - treatment of choice; safe with breastfeeding
- Warfarin acceptable postpartum (safe in breastfeeding); target INR 2-3
- DOACs (rivaroxaban, apixaban) generally avoided while breastfeeding
- Graduated compression stockings
- Early mobilization - key prevention strategy
- Risk-stratify all postpartum women for VTE prophylaxis
Prevention:
- Early ambulation after delivery
- Hydration
- LMWH thromboprophylaxis in high-risk women (C-section, obesity, prior VTE, thrombophilia)
- Park's Textbook of Preventive and Social Medicine
6. Psychological Complications
Psychological disturbances form a spectrum, from mild and transient to severe and life-threatening.
A. Postpartum Blues ("Baby Blues")
- Affects up to 65% of mothers
- Onset: days 3-5 after delivery
- Features: tearfulness, mood lability, anxiety, irritability
- Self-limiting; resolves within 2 weeks
- Management: reassurance, support, rest
B. Postpartum Depression (PPD)
- Affects 3-6% of women (some estimates up to 10-15% for major depression)
- DSM-5 specifier: "with peripartum onset" - onset during pregnancy or within 4 weeks of delivery (clinically, often recognized up to 12 months)
- Features: persistent low mood, anhedonia, sleep disturbance, guilt, poor bonding with infant, thoughts of self-harm
- 10% of mothers with blues progress to full major depression
Risk factors: Past history of depression or PPD, bipolar disorder, family history, inadequate social support, stressful life events
Management:
- Psychotherapy (CBT, interpersonal therapy) - first-line for mild-moderate
- SSRIs (sertraline, paroxetine) - safe in breastfeeding; first-line pharmacotherapy
- Brexanolone (IV neuroactive steroid) - FDA-approved specifically for PPD
- Screen with Edinburgh Postnatal Depression Scale (EPDS)
C. Postpartum Psychosis (Puerperal Psychosis)
- Rare but psychiatric emergency - ~1-2 per 1000 deliveries
- Onset: 48-72 hours after delivery (can be delayed)
- Often follows a delivery complicated by hemorrhage or infection, but frequently occurs without any obstetric complication
Features (from Adams & Victor's Neurology):
- Alternating between noisy hyperactivity and mutism/inactivity
- Disorientation, thought disorder
- Baby may be rejected as not belonging to the mother
- Can present as:
- ~40% predominantly affective
- ~20% schizophreniform
- Remainder: self-limited confusional psychoses (Boyd's series)
- Infanticide and suicidal ideation are the most dangerous aspects
Differential diagnosis of postpartum psychosis (must exclude):
- Eclampsia
- Sheehan's syndrome (pituitary infarction)
- Cerebral venous sinus thrombosis
- Ergot-induced psychosis
- Hypoxic-ischemic brain injury
Management:
- Urgent psychiatric admission (mother-baby unit if available)
- Mood stabilizers (lithium - caution with breastfeeding), antipsychotics
- ECT in severe refractory cases
- Risk: most closely related to past history of postpartum psychosis, bipolar disorder, or family history of bipolar disorder
- Adams & Victor's Principles of Neurology, 12th Ed
- Rosen's Emergency Medicine
Summary Table
| Complication | Timing | Key Feature | First-line Management |
|---|---|---|---|
| Puerperal Sepsis | Within 3 weeks | Foul lochia, fever, uterine tenderness | IV broad-spectrum antibiotics |
| Hematoma | First 24 hours | Tense painful vulval/perineal swelling | Incision & evacuation if large |
| Mastitis | Week 2 postpartum | Unilateral red, tender breast with fever | Antistaphylococcal antibiotics + continue feeding |
| UTI/Pyelonephritis | Any time | Dysuria/loin pain; predisposed by catheterization | Antibiotics per culture |
| DVT/Thrombophlebitis | First 6 weeks (highest: weeks 1-2) | Swollen, tender, pale leg | LMWH anticoagulation |
| Postpartum Blues | Days 3-5 | Tearfulness, transient | Reassurance and support |
| Postpartum Depression | Within 4 weeks - months | Persistent low mood, poor bonding | SSRI + psychotherapy |
| Postpartum Psychosis | 48-72 hours | Confusion, rejection of infant, infanticidal risk | Emergency psychiatric admission |
This is a shared conversation. Sign in to Orris to start your own chat.