Serotonin pharmacology
Reading File
Finding Sources
Finding Sources
Searching PubMed
serotonin pharmacology receptors
Reading File
Reading File
I now have a comprehensive body of content. Let me compile the full answer.
Serotonin Pharmacology
Sources: Katzung's Basic and Clinical Pharmacology, 16th Edition (pp. 446-455)
1. History & Background
Serotonin was first identified as a vasoconstrictor released from blood clots (hence "sero-tonin," from serum). A parallel discovery in intestinal mucosa called the substance "enteramine." The synthesis of 5-hydroxytryptamine (5-HT) in 1951 unified both discoveries. It is now known to be a neurotransmitter, a local gut hormone, a platelet constituent, and a mediator in migraine and carcinoid syndrome.
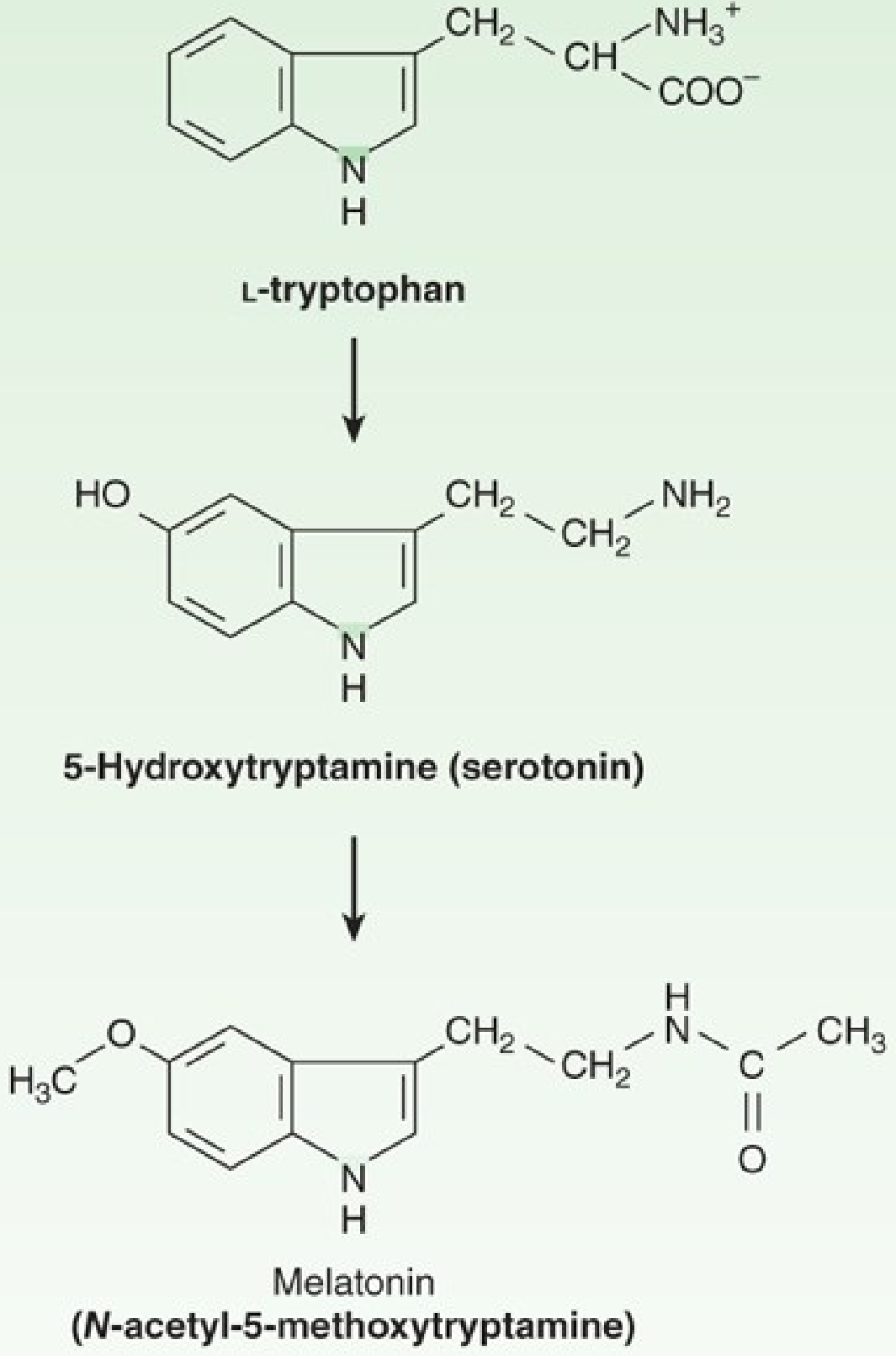
2. Chemistry & Synthesis
Serotonin is an indolealkylamine derived from the essential amino acid L-tryptophan:
- Tryptophan hydroxylase-1 hydroxylates the indole ring at C5 (rate-limiting step) - blocked by p-chlorophenylalanine (PCPA/fenclonine) and p-chloroamphetamine
- Aromatic L-amino acid decarboxylase removes the carboxyl group to yield 5-HT
In the pineal gland, 5-HT is acetylated and then methylated to form melatonin.
3. Distribution & Pharmacokinetics
| Location | % of body 5-HT | Notes |
|---|---|---|
| Enterochromaffin (GI) cells | >90% | Primary source; released into portal blood |
| Platelets | ~8% | Concentrated via SERT transporter |
| CNS raphe nuclei | <2% | Serotonergic neuron cell bodies |
Uptake: Serotonin enters platelets and nerve terminals via the serotonin transporter (SERT), then concentrated in vesicles by a vesicular amine transporter (VAT) - blocked by reserpine.
Metabolism: Primarily by monoamine oxidase (MAO) to 5-hydroxyindoleacetaldehyde, then to 5-HIAA (5-hydroxyindoleacetic acid) by aldehyde dehydrogenase. 5-HIAA is excreted in urine and is a useful marker for carcinoid tumors (elevated in carcinoid syndrome).
4. Receptor Subtypes & Their Pharmacology
There are at least seven receptor families (5-HT1 through 5-HT7) with multiple subtypes.
5-HT1 Family (Gi/Go coupled - inhibitory)
| Subtype | Location | Key effects | Drugs |
|---|---|---|---|
| 5-HT1A | Raphe neurons, hippocampus, limbic areas | Inhibits neuronal firing; reduces anxiety | Buspirone (partial agonist - anxiolytic) |
| 5-HT1B/1D | Presynaptic terminals; cerebral/meningeal vessels | Vasoconstriction; inhibits 5-HT/neuropeptide release | Triptans (sumatriptan, etc. - migraine) |
| 5-HT1F | Neurons | Inhibits neuropeptide release | Lasmiditan (migraine, non-vasoconstrictor) |
5-HT2 Family (Gq/G11 coupled - excitatory/complex)
| Subtype | Location | Key effects | Drugs |
|---|---|---|---|
| 5-HT2A | Smooth muscle, platelets, CNS cortex | Vasoconstriction, platelet aggregation, hallucinations | Antagonism by atypical antipsychotics (clozapine, quetiapine), ketanserin |
| 5-HT2B | Fundus of stomach, heart valves | Excitation; associated with cardiac valvulopathy | Avoided (ergotamine long-term use) |
| 5-HT2C | CNS (especially hypothalamus) | Appetite suppression, mood | Lorcaserin (withdrawn); some antipsychotics |
5-HT3 (Ligand-gated ion channel - unique among 5-HT receptors)
- Location: CNS (area postrema/chemoreceptor trigger zone), peripheral sensory/autonomic neurons, GI tract
- Effect: Rapid depolarization; mediates nausea/vomiting, pain, GI motility
- Drugs: Ondansetron, granisetron, dolasetron (5-HT3 antagonists) - highly effective antiemetics especially for chemotherapy-induced nausea
5-HT4 (Gs coupled - excitatory)
- Location: GI tract neurons, heart, CNS
- Effect: Increases cAMP; enhances gut motility (prokinetic); positive chronotropy in atria
- Drugs: Metoclopramide (partial agonist); tegaserod (partial agonist, approved for IBS-C); cisapride (withdrawn due to QT prolongation)
5-HT5, 5-HT6, 5-HT7
- Less well characterized clinically
- 5-HT6/5-HT7: High affinity for several atypical antipsychotics and antidepressants; role in cognition and circadian rhythm (5-HT7)
5. Physiological Effects by Organ System
Cardiovascular
- Arteries/veins: 5-HT directly constricts most vessels (5-HT2A), but can relax vessels with healthy endothelium via NO release; net effect depends on vascular bed and endothelial integrity
- Heart: Positive inotropy and chronotropy at 5-HT4; bradycardia via Bezold-Jarisch reflex (5-HT3 on vagal afferents)
- Platelets: 5-HT released from activated platelets amplifies aggregation and vasoconstriction
GI Tract
- Stimulates smooth muscle contraction (peristalsis) via 5-HT3 and 5-HT4 on enteric neurons
- Enterochromaffin cells release 5-HT in response to luminal pressure/chemicals - drives the peristaltic reflex
- Diarrhea is a hallmark of carcinoid syndrome (excess 5-HT)
CNS
- Broad modulatory role: mood, sleep (promotes NREM sleep onset), appetite, cognition, impulse control
- Raphe nuclei project to the entire forebrain
- Low serotonergic tone associated with depression, anxiety, impulsivity
Platelet Function
- 5-HT is stored and released from dense granules; amplifies platelet aggregation and potentiates ADP/thromboxane effects
6. Clinical Pharmacology - Key Drug Classes
Serotonin Synthesis Inhibitors
- Telotristat ethyl - oral tryptophan hydroxylase-1 inhibitor, approved for carcinoid syndrome diarrhea
- PCPA/fenclonine - research tools only (too toxic)
5-HT1A Agonists
- Buspirone - partial agonist at 5-HT1A (also D2 antagonist); anxiolytic without sedation/dependence; slow onset (1-3 weeks)
Triptans (5-HT1B/1D Agonists)
- Sumatriptan, zolmitriptan, rizatriptan, eletriptan, naratriptan, almotriptan, frovatriptan
- Acute migraine treatment: constrict dilated meningeal/cerebral vessels; inhibit trigeminal neuropeptide release
- Contraindicated in coronary artery disease, uncontrolled hypertension, prior stroke (risk of vasospasm)
- Lasmiditan (5-HT1F agonist) - newer "dittan"; lacks vasoconstrictor effect; can be used when triptans are contraindicated
5-HT2A Antagonists
- Ketanserin - antihypertensive; blocks vascular 5-HT2A
- Cyproheptadine - antihistamine + 5-HT2 antagonist; used for carcinoid flushing, appetite stimulation, serotonin syndrome
- Methysergide - historical prophylaxis for migraine/cluster headache; now largely abandoned due to retroperitoneal fibrosis risk
5-HT3 Antagonists (Setrons)
- Ondansetron, granisetron, dolasetron, palonosetron
- Prevent chemotherapy-induced, radiation-induced, and post-operative nausea/vomiting
- Act on vagal afferents and area postrema
Serotonin Reuptake Inhibitors (SERT Blockers)
- SSRIs (fluoxetine, sertraline, paroxetine, escitalopram): block SERT on neurons; increase synaptic 5-HT; first-line for depression/anxiety
- SNRIs (venlafaxine, duloxetine): block both SERT and NET
- TCAs (amitriptyline, clomipramine): also block SERT (plus NET, muscarinic, H1)
- Tramadol: weak SERT inhibitor + mu-opioid agonist
- MDMA ("ecstasy"): massive 5-HT release via reversal of SERT
Ergot Alkaloids (Mixed 5-HT Agonist/Antagonist)
- Ergotamine, dihydroergotamine (DHE): partial agonists at 5-HT1B/1D; also affect adrenergic and dopaminergic receptors; used in migraine
- Ergotism (from prolonged ergot exposure): intense vasoconstriction, limb ischemia, CNS effects
7. Serotonin Syndrome
A potentially life-threatening drug toxicity caused by excess serotonergic activity.
Classic triad:
- Neuromuscular abnormalities - tremor, myoclonus, hyperreflexia, clonus (especially lower extremity)
- Autonomic instability - hyperthermia, diaphoresis, tachycardia, hypertension, diarrhea
- Altered mental status - agitation, confusion
Common precipitants: Combination of SSRIs + MAOIs (most dangerous), SSRIs + tramadol, linezolid + SSRIs, triptans + SSRIs (debated)
Treatment: Discontinue offending agents; cyproheptadine (5-HT2A antagonist) as antidote; supportive care; benzodiazepines for agitation; severe cases may need cooling, intubation
8. Carcinoid Syndrome
Enterochromaffin cell tumors secrete excess 5-HT (and other mediators). Manifestations include:
- Flushing, diarrhea, bronchoconstriction, right-sided cardiac valve lesions (tricuspid/pulmonary thickening from 5-HT2B stimulation)
- 5-HIAA elevated in 24-hour urine
- Treatment: Somatostatin analogs (octreotide, lanreotide) as primary therapy; telotristat ethyl for diarrhea; cyproheptadine or ketanserin for symptomatic relief
Summary Table: Receptor-Drug Pairs
| Receptor | Coupling | Clinical Use | Example Drugs |
|---|---|---|---|
| 5-HT1A | Gi | Anxiety | Buspirone |
| 5-HT1B/1D | Gi | Migraine (acute) | Sumatriptan, triptans |
| 5-HT1F | Gi | Migraine (CV risk) | Lasmiditan |
| 5-HT2A (antagonist) | Gq | HTN, carcinoid, antipsychotic | Ketanserin, cyproheptadine |
| 5-HT2C (agonist) | Gq | Obesity (withdrawn) | Lorcaserin |
| 5-HT3 (antagonist) | Ion channel | Antiemetic | Ondansetron |
| 5-HT4 (agonist) | Gs | Prokinetic, IBS-C | Tegaserod, metoclopramide |
| SERT (inhibitor) | - | Depression, anxiety, OCD | SSRIs, SNRIs |
- Katzung's Basic and Clinical Pharmacology, 16th Edition, pp. 446-455
This is a shared conversation. Sign in to Orris to start your own chat.