The patient is a 58-year-old male with a 10-year history of Type 2 diabetes (on Metformin 1000mg twice daily), hypertension (on Amlodipine 5mg), and recently started experiencing chest tightness, mild shortness of breath on exertion, occasional dizziness, and swelling in both ankles over the past 3 weeks. His last HbAlc was 8.2%, BP today is 148/92 mmHg, and my fasting blood sugar this morning was 210 mg/dL. He also smoke half a pack a day and have a family history of heart disease. What could be going on, and what should I do?
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Searching PubMed
"heart failure" AND "type 2 diabetes" AND "SGLT2"
Loading Image
I now have everything needed for a comprehensive, well-cited response.
Clinical Assessment: 58-Year-Old Male with Diabetes, Hypertension, and New Cardiopulmonary Symptoms
Disclaimer: This is clinical educational content based on authoritative medical textbooks and current evidence. It is not a substitute for direct patient evaluation, full history/physical, and clinical judgment.
What Is Likely Going On
This patient's symptom cluster - chest tightness, exertional dyspnea, bilateral ankle edema, and dizziness over 3 weeks - in the context of a 10-year history of Type 2 DM, poorly controlled hypertension (BP 148/92), and active smoking, raises several serious and overlapping diagnoses that must be urgently evaluated.
The Leading Differentials (in order of urgency)
1. Heart Failure (Most Probable Primary Diagnosis)
The triad of exertional dyspnea + bilateral ankle edema + chest tightness is the textbook presentation of heart failure. This patient has three of the most powerful drivers of heart failure converging simultaneously:
- Hypertension is the single greatest population-attributable risk factor for heart failure. Even modest increases in blood pressure confer disproportionate risk over decades.
- Type 2 Diabetes (10 years duration) doubles the risk of heart failure independently. Heart failure is twice as common in people with diabetes and is related to diabetes duration and hypertension. It can present as HFpEF, HFmEF, or HFrEF. Some patients develop "diabetic cardiomyopathy" - reduced left ventricular function without any CHD or hypertension as a separate mechanism.
- Coronary artery disease (CAD) accounts for nearly 70% of heart failure cases in developed countries, and this patient's CAD risk is very high (see below).
- Harrison's Principles of Internal Medicine 22E, p. 3271; Goldman-Cecil Medicine, p. 461
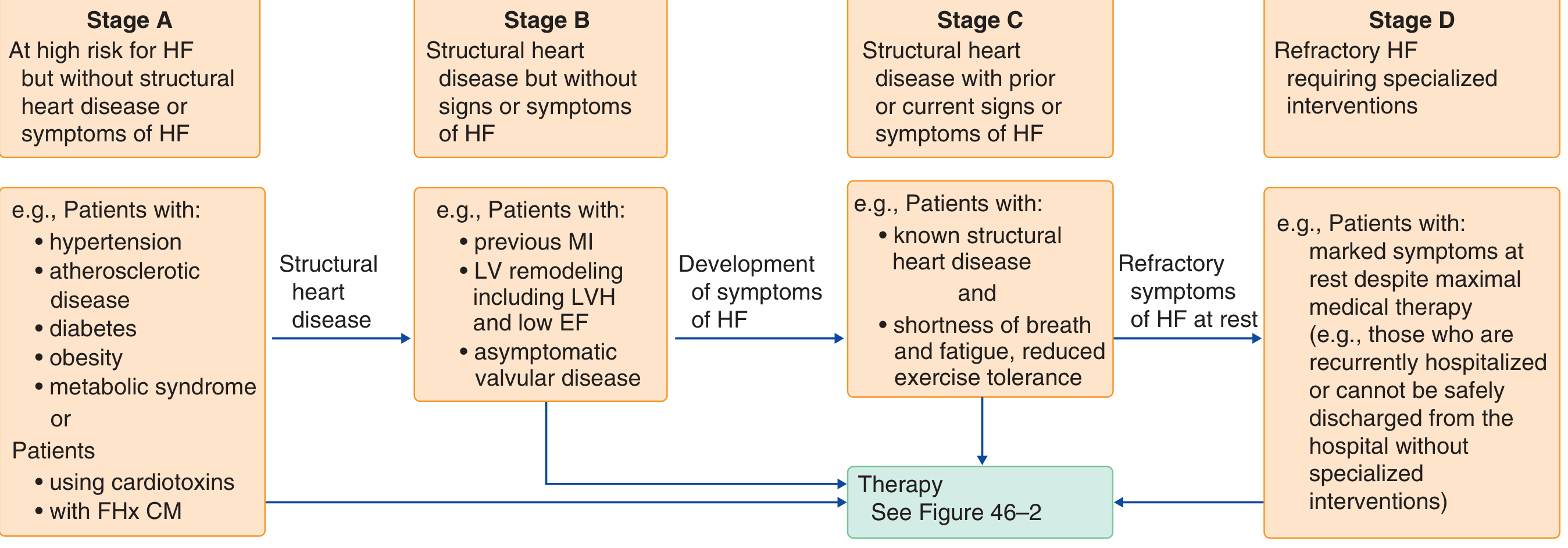
This patient fits Stage C heart failure on the AHA/ACC staging framework - structural heart disease with current signs and symptoms:
2. Acute Coronary Syndrome / Ischemic Heart Disease (Must Rule Out Urgently)
The chest tightness in this patient cannot be attributed to heart failure alone without first ruling out ACS. Key reasons:
- "Silent ischemia" is common in diabetes. Harrison's explicitly notes that the absence of chest pain is common in individuals with diabetes, and atypical symptoms of cardiac ischemia should prompt a thorough cardiac evaluation.
- The combination of Type 2 DM + hypertension + smoking + family history of heart disease places this patient in the highest-risk category for CAD. Some studies show that type 2 DM patients without a prior MI have equivalent coronary event risk to non-diabetic individuals who have already had an MI.
- The dizziness could represent low cardiac output or arrhythmia secondary to ischemia.
- Harrison's Principles of Internal Medicine 22E, p. 3271
3. Poorly Controlled Hypertension Contributing to Target Organ Damage
BP of 148/92 mmHg is Stage 2 hypertension, uncontrolled on current Amlodipine 5mg monotherapy. Chronic hypertension causes left ventricular hypertrophy (LVH), which leads to diastolic dysfunction - the most common substrate for HFpEF. This also directly amplifies the CAD and stroke risk.
4. Poorly Controlled Diabetes with Cardiovascular Consequences
HbA1c of 8.2% and fasting glucose of 210 mg/dL indicate significant hyperglycemia. This directly accelerates:
- Atherosclerosis and CAD
- Endothelial dysfunction
- Cardiomyopathy
- Renal injury (which further worsens hypertension and fluid retention)
- Harrison's Principles of Internal Medicine 22E, p. 3271
What Should Be Done: Immediate Steps
Urgent Workup (Do Today / Same Day)
| Investigation | Rationale |
|---|---|
| 12-lead ECG | Screen for ischemia, LVH, arrhythmia |
| Chest X-ray | Look for cardiomegaly, pulmonary edema, pleural effusion |
| Cardiac biomarkers (Troponin I or T, BNP/NT-proBNP) | Rule out ACS; BNP confirms/grades heart failure |
| Basic metabolic panel (electrolytes, BUN, creatinine, eGFR) | Assess renal function before starting/adjusting meds |
| CBC | Anemia can exacerbate dyspnea and worsen cardiac output |
| Fasting lipid panel | Assess CV risk; likely dyslipidemia is present |
| HbA1c (already known: 8.2%) | Confirm and track glycemic control |
| Urinalysis + spot urine albumin/creatinine | Detect diabetic nephropathy - also a strong CV risk marker |
If troponin is elevated or ECG shows ischemic changes → Emergency cardiology referral/ER transfer immediately.
Imaging and Functional Assessment
- Echocardiogram - the most important next test. It will distinguish HFrEF vs HFpEF, detect wall motion abnormalities suggesting ischemia, quantify LVH, and guide drug therapy selection.
- Stress testing / myocardial perfusion imaging - appropriate given symptoms suggestive of cardiac ischemia in a diabetic patient, once ACS is ruled out acutely.
Management Priorities
1. Cardiovascular/Heart Failure Treatment
Based on Goldman-Cecil Medicine and current AHA/ACC guidelines, core therapy for heart failure includes:
- ACE inhibitor or ARB (or sacubitril/valsartan, the ARNI) - reduce afterload, mortality benefit
- Beta-blocker - carvedilol, bisoprolol, or metoprolol succinate. Note: beta-blockers are not contraindicated in diabetes with heart failure - they provide positive benefit. Goldman-Cecil Medicine, p. 491
- Mineralocorticoid receptor antagonist (MRA) - spironolactone or eplerenone
- SGLT2 inhibitor - this is the most important pharmacological upgrade for this specific patient (see below)
2. The SGLT2 Inhibitor - A Critical Addition
SGLT2 inhibitors (empagliflozin, dapagliflozin) are now a cornerstone of heart failure therapy with uniquely applicable benefits here:
"Treatment with an SGLT2 inhibitor is recommended for all patients with symptomatic heart failure and a reduced ejection fraction, irrespective of diabetes status." - Goldman-Cecil Medicine, p. 484
"In patients who have heart failure and type 2 diabetes, the SGLT2 inhibitors are the preferred antidiabetic agents." - Goldman-Cecil Medicine, p. 491
For this patient, SGLT2 inhibitors provide a triple benefit:
- Improve heart failure outcomes (reduce hospitalizations and mortality)
- Lower blood glucose and HbA1c
- Reduce BP modestly and slow CKD progression
Recent evidence supports this strongly: a 2024 systematic review in Circulation confirmed cardiovascular and kidney benefits of GLP-1 + SGLT2 combinations in Type 2 DM, and a meta-analysis in JAMA (2026) confirmed kidney-protective effects of SGLT2 inhibitors across the spectrum of eGFR and albuminuria.
Important caveat: Metformin should be reviewed - it carries a risk of lactic acidosis in patients with severe heart failure. It should be temporarily held if the patient is hospitalized or decompensating, and kidney function must be confirmed to be adequate before continuing. Goldman-Cecil Medicine, p. 491
3. Blood Pressure Control
Current Amlodipine 5mg is inadequate at 148/92. The treatment plan should:
- Add an ACE inhibitor or ARB (which also addresses heart failure)
- Target BP <130/80 mmHg in a diabetic patient with established CVD risk
- Consider up-titrating or adding a diuretic (which will also help with edema)
4. Diabetes Optimization
- SGLT2 inhibitor as above (replaces or supplements Metformin)
- Consider a GLP-1 receptor agonist (e.g., semaglutide, liraglutide) - GLP-1 RAs do not increase heart failure risk and have proven ASCVD benefit in high-risk type 2 DM patients
- Avoid: Thiazolidinediones (cause fluid retention, worsen HF), saxagliptin (increases HF risk), DPP-4 inhibitors (not recommended in HF)
5. Smoking Cessation - High Priority
Smoking is an independent risk factor for CAD restenosis and cardiovascular events. Cessation counseling and pharmacotherapy (varenicline or NRT) should be initiated at this visit. This is not optional - it is one of the most impactful modifiable interventions available.
6. Lifestyle Modifications
- Low-sodium diet (<2g/day) to manage fluid retention
- Fluid restriction if clinically indicated
- Daily weights to monitor fluid status
- Regular, appropriately dosed physical activity once stabilized
- Weight management
Red Flags Requiring Emergency Escalation
Refer to the ER immediately if any of the following occur:
- Troponin elevation or ischemic ECG changes
- Acute pulmonary edema (severe dyspnea at rest, hypoxia)
- BP >180/110 or hypertensive emergency
- Syncope or pre-syncope
- New onset atrial fibrillation
Summary
This patient has a high-probability presentation of new-onset heart failure (likely HFpEF given his hypertension-dominant profile, but HFrEF from CAD must be excluded) on a background of convergent cardiovascular risk factors. The combination of 10-year T2DM, uncontrolled hypertension, active smoking, family history, poor glycemic control, and now symptomatic cardiopulmonary decompensation makes this a high-urgency clinical scenario.
The single most important immediate next step is a BNP/NT-proBNP + ECG + Troponin on the same day, followed by echocardiography. The most impactful pharmacological change is adding an SGLT2 inhibitor, which addresses heart failure, glycemia, and renal protection simultaneously.
This is a shared conversation. Sign in to Orris to start your own chat.