Explain in detail about acute diarrhoea in children with classification of dehydration and management
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
I now have all the information needed for a comprehensive answer. Let me compose it.
Acute Diarrhoea in Children - A Comprehensive Overview
Definition
Diarrhoea is defined as the passage of 3 or more loose or watery stools per day (or more frequently than is normal for the individual). Acute diarrhoea lasts fewer than 14 days. A young infant has diarrhoea if stools have changed from the usual pattern and are many and watery (more water than faecal matter) - the normally frequent or semi-solid stools of a breastfed baby are NOT diarrhoea.
- Acute diarrhoea: < 14 days
- Persistent diarrhoea: ≥ 14 days
- Dysentery: diarrhoea with blood in the stool
Epidemiology & Global Burden
Diarrhoeal diseases remain one of the leading causes of morbidity and mortality in children under 5 years globally, particularly in low- and middle-income countries. The primary danger is dehydration, which can lead to death if untreated. Rotavirus vaccination has significantly reduced the burden of viral gastroenteritis in vaccinated populations.
Etiology and Classification of Acute Diarrhoea
By Mechanism (Pathophysiology)
| Type | Mechanism | Common Causes |
|---|---|---|
| Secretory | Toxin-mediated hypersecretion of fluid/electrolytes | V. cholerae, ETEC, Rotavirus |
| Osmotic | Unabsorbed solutes draw water into the gut lumen | Lactose intolerance, viral gastroenteritis |
| Invasive/Inflammatory | Mucosal invasion causing blood/mucus in stool | Shigella, Salmonella, Campylobacter, E. coli O157:H7, Entamoeba |
| Dysmotility | Altered gut transit | Post-infectious IBS, medications |
By Etiology
Infectious (most common in children):
- Viral (most common overall): Rotavirus (leading cause of severe dehydration in children under 5), Norovirus, Adenovirus, Astrovirus. Rotavirus vaccination has made it less prevalent in vaccinated populations.
- Bacterial: E. coli (ETEC, EPEC, EHEC), Shigella, Salmonella, Campylobacter, V. cholerae, Clostridium difficile
- Parasitic: Giardia lamblia, Entamoeba histolytica, Cryptosporidium
Non-infectious:
- Lactose malabsorption
- Small bowel bacterial overgrowth
- Allergic enteropathy / cow's milk protein allergy
- Cystic fibrosis
- Hirschsprung disease
- Medications (antibiotics)
WHO IMCI Classification of Diarrhoea (Pediatric)
A. Classification for Dehydration
The Integrated Management of Childhood Illness (IMCI) framework classifies diarrhoea by dehydration severity using a "traffic light" colour-coded system based on clinical signs:
Assessment Signs (Look and Feel):
- General condition: Lethargic/unconscious? Restless and irritable?
- Eyes: Sunken?
- Thirst: Not able to drink / drinking poorly? Or drinking eagerly / thirsty?
- Skin pinch: Goes back very slowly (>2 seconds)? Slowly? Or immediately?
Dehydration Classification Table (WHO/IMCI)
| Classification | Colour | Signs Required | Treatment Plan |
|---|---|---|---|
| Severe Dehydration | 🔴 Pink | Two or more: Lethargic/unconscious; Sunken eyes; Not able to drink or drinking poorly; Skin pinch goes back very slowly (>2 sec) | Plan C - IV fluids urgently |
| Some Dehydration | 🟡 Yellow | Two or more: Restless/irritable; Sunken eyes; Drinks eagerly/thirsty; Skin pinch goes back slowly | Plan B - ORS in clinic over 4 hours |
| No Dehydration | 🟢 Green | Not enough signs for Some or Severe dehydration | Plan A - Treat at home with extra fluids |
(Park's Textbook of Preventive and Social Medicine)
B. Classification by Duration
| Type | Duration | Key Feature |
|---|---|---|
| Acute Diarrhoea | < 14 days | Most common; risk of dehydration |
| Persistent Diarrhoea | ≥ 14 days | Risk of malnutrition |
| Dysentery | Any duration | Blood in stool - needs antibiotic |
C. Percentage Dehydration (Clinical/Weight-Based)
This is the traditional pediatric classification used alongside IMCI:
| Degree | % Body Weight Lost | Clinical Features |
|---|---|---|
| Mild | 3-5% | Slightly dry mucous membranes, increased thirst, normal skin turgor |
| Moderate | 6-9% | Sunken eyes and fontanelle, decreased skin turgor, tachycardia, decreased urine output, irritable |
| Severe | ≥ 10% | Markedly sunken eyes/fontanelle, very poor skin turgor, tachycardia, weak/absent pulse, lethargic/unconscious, cold extremities, oliguria/anuria |
Management
Overview
Management of acute diarrhoea in children follows the WHO IMCI Treatment Plans A, B, and C, based on the degree of dehydration.
PLAN A: No Dehydration - Home Treatment
4 Rules of Home Treatment:
1. Give Extra Fluid (as much as the child will take)
- Breastfed: breastfeed frequently and for longer
- Non-exclusively breastfed: ORS, food-based fluids (soup, rice water, yoghurt drinks), or clean water
| Age | ORS Amount per Loose Stool |
|---|---|
| Up to 2 years | 50-100 mL after each loose stool |
| 2 years or older | 100-200 mL after each loose stool |
- Give frequent small sips from a cup
- If the child vomits, wait 10 minutes, then continue more slowly
2. Give Zinc Supplements (for age 2 months up to 5 years)
- 2 months - 6 months: 10 mg/day for 10-14 days
- 6 months - 5 years: 20 mg/day for 10-14 days
- For infants: dissolve in breast milk, ORS or clean water
- For older children: chew or dissolve in small amount of water
Rationale for zinc: Zinc reduces the duration and severity of diarrhoea and decreases the probability of subsequent episodes over the following 2-3 months.
3. Continue Feeding
- Exclusive breastfeeding if age < 6 months
- Do NOT restrict food - early refeeding prevents malnutrition
4. When to Return Immediately:
- Cannot drink or breastfeed
- Becomes sicker
- Develops fever
- Blood in stool
PLAN B: Some Dehydration - ORS in Clinic Over 4 Hours
ORS dose = 75 mL/kg over 4 hours
| Age | Weight | ORS in 4 hours |
|---|---|---|
| Up to 4 months | < 6 kg | 200-450 mL |
| 4-12 months | 6-<10 kg | 450-800 mL |
| 12 months - 2 years | 10-<12 kg | 800-960 mL |
| 2-5 years | 12-19 kg | 960-1600 mL |
(Approximate formula: weight in kg × 75 = mL of ORS)
Administration:
- Give frequent small sips from a cup
- If vomiting: wait 10 minutes, then restart more slowly
- Continue breastfeeding whenever the child wants
- After 4 hours: Reassess and classify dehydration, select appropriate plan, begin feeding in clinic
Note for infants < 6 months not breastfed using standard ORS: Also give 100-200 mL clean water during this period (not needed with low-osmolarity ORS)
PLAN C: Severe Dehydration - Treat Quickly
The WHO Plan C flowchart:
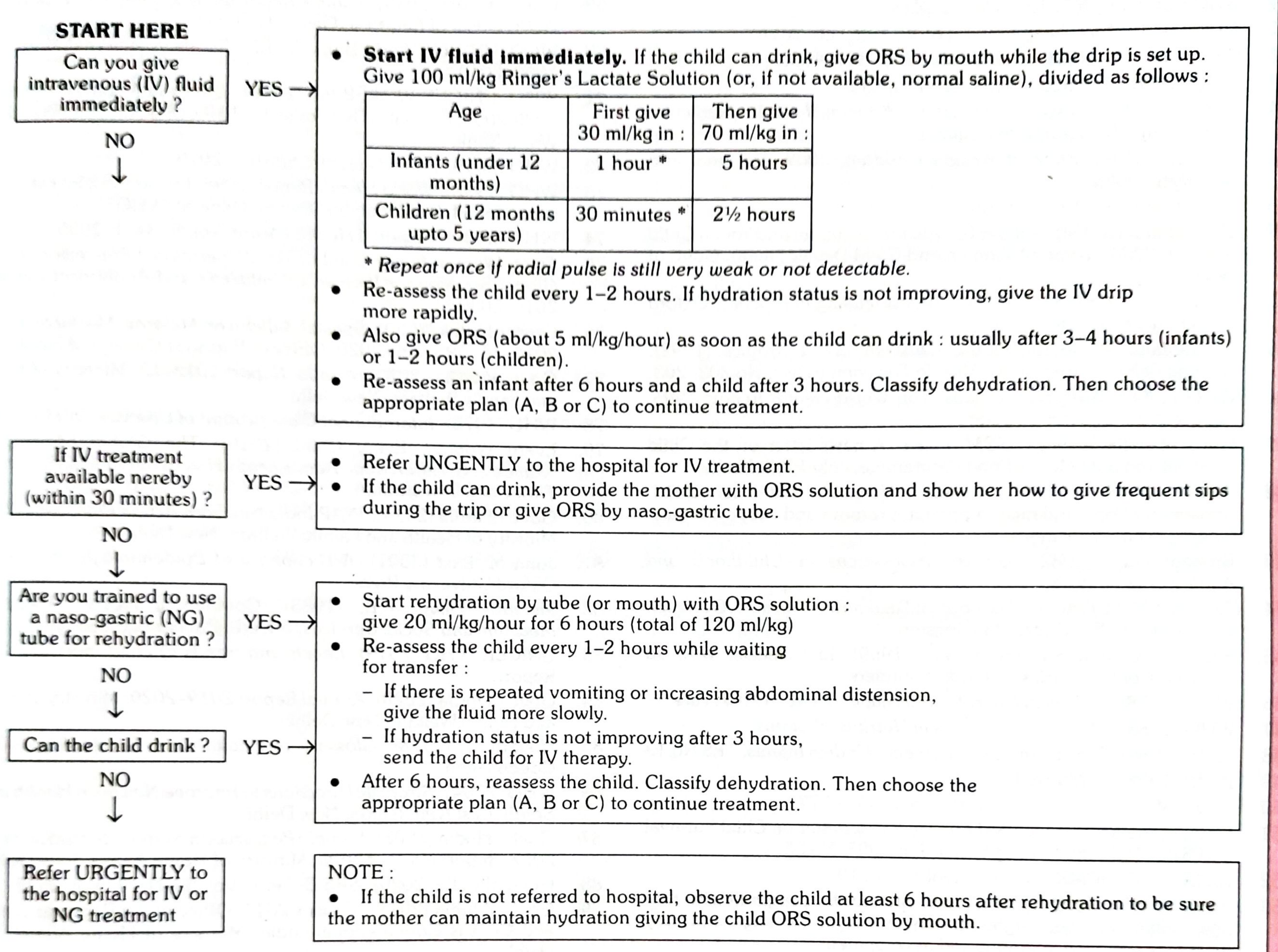
If IV fluids available immediately:
- Start IV fluids with Ringer's Lactate solution (or normal saline if RL unavailable): 100 mL/kg total
| Age | First: 30 mL/kg | Then: 70 mL/kg |
|---|---|---|
| Infants (< 12 months) | Over 1 hour* | Over 5 hours |
| Children (12 months - 5 years) | Over 30 minutes* | Over 2.5 hours |
Repeat first bolus once if radial pulse is still very weak or not detectable
- Reassess every 1-2 hours; if not improving, give IV drip more rapidly
- Also give ORS (~5 mL/kg/hour) as soon as child can drink: after 3-4 hours (infants) or 1-2 hours (children)
- Reassess after 6 hours (infants) or 3 hours (children), then choose appropriate plan
If IV unavailable but within 30 minutes:
- Refer URGENTLY to hospital; give ORS sips on the way
If trained in NG tube:
- ORS via NG: 20 mL/kg/hour for 6 hours (120 mL/kg total)
- Reassess every 1-2 hours
If unable to drink and none of the above:
- Refer URGENTLY for IV or NG treatment
WHO Oral Rehydration Solution (ORS) Composition
The reduced-osmolarity WHO-ORS is recommended (Harrison's Principles of Internal Medicine):
| Constituent | Concentration (mmol/L) |
|---|---|
| Na⁺ | 75 |
| K⁺ | 20 |
| Cl⁻ | 65 |
| Citrate | 10 |
| Glucose | 75 |
| Total osmolarity | 245 |
This reduced-osmolarity formula (vs. old 311 mOsm/L) reduces stool output and vomiting and reduces the need for unscheduled IV therapy.
Additional Management Measures
Dietary Management
- Do not restrict food - early refeeding reduces intestinal permeability and duration of illness
- Resume regular age-appropriate diet as soon as tolerated
- Avoid high-sugar drinks (juice, soft drinks) - osmotic worsening
- Breastfeeding should never be interrupted
Pharmacotherapy
From the Harriet Lane Handbook (23rd ed.):
- Non-specific antidiarrheal agents: No supporting evidence for routine use
- Antimotility agents (loperamide): NOT recommended in children with acute infectious diarrhoea - risk of ileus, toxic megacolon
- Antisecretory drugs, toxin binders (cholestyramine): No evidence of benefit
- Antibiotics: Only for specific indications:
- Shigella dysentery: azithromycin or ciprofloxacin
- V. cholerae: doxycycline (>8 years) or azithromycin
- Giardia: metronidazole or tinidazole
- C. difficile: oral vancomycin or metronidazole
- Cholera in children ≥ 2 years if cholera in area
- Probiotics: Limited but demonstrated evidence in antibiotic-associated diarrhoea and severe recurrent C. difficile
Zinc Supplementation
- 10-14 day course of zinc reduces duration, severity, and risk of future episodes
- Recommended by WHO for all children 2 months - 5 years with acute diarrhoea
Parenteral Hydration
Indicated when:
- Severe dehydration
- Hemodynamic instability
- Failure of ORT (persistent vomiting, ileus)
- Altered consciousness
When to Refer / Red Flags
- Severe dehydration (Plan C criteria)
- Blood in stool (dysentery) with systemic toxicity
- Persistent diarrhoea ≥ 14 days
- Signs of shock (cold extremities, weak/absent pulse, altered consciousness)
- Failure to improve after rehydration
- Age < 6 months with signs of dehydration
- Concurrent severe illness (pneumonia, meningitis)
Prevention
- Rotavirus vaccination (dramatically reduces burden in children < 5 years)
- Exclusive breastfeeding for the first 6 months
- Safe drinking water and sanitation (WASH)
- Proper hand hygiene / hand-washing with soap
- Safe food preparation
- Continued breastfeeding during illness
Summary Flow
Acute Diarrhoea in a Child
|
Assess Dehydration (IMCI Criteria)
|
_____|_______________
| | |
No Dehy Some Dehy Severe Dehy
| | |
Plan A Plan B Plan C
(Home) (ORS 4 hr (IV fluids
in clinic) urgently)
|
All Plans: Zinc + Continue Feeding + When to Return
Key Sources:
- Park's Textbook of Preventive and Social Medicine (IMCI Management Plans A, B, C)
- The Harriet Lane Handbook, 23rd Ed. (Differential diagnosis and pharmacotherapy)
- Harrison's Principles of Internal Medicine, 22nd Ed. (WHO-ORS composition)
- ROSEN's Emergency Medicine (Etiology - rotavirus, norovirus)
Find recent WHO guidelines on acute diarrhoea management in children
Searching the Web
WHO guidelines acute diarrhoea management children 2023 2024 2025
Searching PubMed
"acute diarrhea" AND "children" AND "guidelines"
Reading Web Page
https://www.who.int/publications/i/item/9789240103412
Reading Article
PMID: 40437180
Searching the Web
WHO 2024 guideline pneumonia diarrhoea children zinc dose new recommendations changes
Reading Web Page
https://www.childhealthtaskforce.org/sites/default/files/202…
Searching the Web
WHO 2024 "9789240103412" diarrhoea children recommendations zinc "new dose" ORS rehydration plan
Reading Web Page
https://www.unicef.org/supply/oral-rehydration-salts-ors-and…
I now have everything needed for a comprehensive, fully up-to-date answer. Here is a detailed summary of the latest WHO guidelines.
Recent WHO Guidelines on Acute Diarrhoea Management in Children
Landmark 2024 WHO Guideline
Title: Guideline on Management of Pneumonia and Diarrhoea in Children up to 10 Years of Age
Published: 31 December 2024 | ISBN: 9789240103412
WHO Teams: Child Health and Development (CHD); Maternal, Newborn, Child & Adolescent Health & Ageing (MCA)
Why This Guideline Matters
This is the most significant update to WHO's childhood diarrhoea management framework in over a decade. Previous guidance focused mainly on children under 5 years. This 2024 guideline extends the scope to children up to 10 years of age, addressing a recognised policy gap called out by national decision-makers worldwide.
According to the guideline:
- Pneumonia and diarrhoea together account for 23% of under-five mortality - approximately 1.17 million deaths in children under 5 in 2021
- In children 5-9 years, these same two conditions caused ~86,000 preventable deaths in 2021 - a group previously without dedicated WHO guidance
Key Recommendation Changes from Previous WHO Guidance
1. Extended Age Range
- Recommendations now apply to children up to 10 years (previously up to 5 years)
- The same core diarrhoea management principles apply - ORS + zinc + continued feeding - but now formally cover the 5-9 year age group
2. New Zinc Dose - Most Important Clinical Update
This is the headline change for diarrhoea management:
| Previous WHO Recommendation | 2024 Updated Recommendation | |
|---|---|---|
| Zinc dose | 20 mg/day (children ≥6 months) / 10 mg/day (<6 months) | 5 mg/day for up to 14 days |
| Formulation | Zinc sulphate (prevalent) | Zinc gluconate preferred |
| Reason for change | - | Reduce vomiting as a side effect; better taste/tolerability |
| Duration | 10-14 days | Up to 14 days |
Critical Transitional Note (as of July 2026): Per UNICEF Supply Division (updated 6 July 2026): "As 5 mg zinc tablets are not yet commercially available, WHO and UNICEF advise continued use of the established 20 mg per day for 14 days." The new 5 mg formulation is the target but supply has not yet caught up. Zinc gluconate is the preferred salt going forward.
3. ORS Recommendations - Unchanged Core, Extended Age
- Low-osmolarity ORS remains the standard of care for acute watery diarrhoea and dehydration in children up to 10 years
- ORS composition unchanged: Na⁺ 75 mmol/L, K⁺ 20 mmol/L, Cl⁻ 65 mmol/L, Citrate 10 mmol/L, Glucose 75 mmol/L, total osmolarity 245 mOsm/L
- The Plan A / Plan B / Plan C framework remains the basis of management
4. Pneumonia-Specific Changes (Context)
- Greater scope for community-level pneumonia treatment
- New clinical signs to diagnose hypoxaemia when pulse oximetry is unavailable
Core WHO Diarrhoea Recommendations Reaffirmed (2024)
All of the following are confirmed and reinforced in the 2024 guideline:
| Recommendation | Detail |
|---|---|
| Low-osmolarity ORS | For all children with acute watery diarrhoea + dehydration, up to age 10 |
| Zinc supplementation | For all acute watery OR persistent diarrhoea; target dose 5 mg/day; use 20 mg/day until new formulation available |
| Continued feeding | Do not withhold food; resume regular age-appropriate diet as soon as tolerated |
| Breastfeeding | Never interrupt; continue throughout illness |
| No antidiarrhoeal agents | Antimotility drugs (loperamide) not recommended |
| Selective antibiotics | Only for dysentery (Shigella), suspected cholera with severe dehydration, or specific comorbidities |
China 2024 Clinical Practice Guidelines - Key Updates
A parallel set of Chinese clinical practice guidelines for acute infectious diarrhoea in children (2024), published in World Journal of Pediatrics (2025), updated from their 2018 edition, offer complementary evidence-based guidance:
- Probiotics: Moderately advised for viral watery diarrhoea (modest evidence)
- Racecadotril (antisecretory): Remains unsupported by current evidence
- Zinc: Recommended for children >6 months in zinc-deficient regions
- Antibiotics: Restricted to:
- Dysenteric-like symptoms
- Suspected cholera with severe dehydration
- Cases with significant comorbidities
- Etiological diagnosis: Standardised evaluation now guides management decisions
Global Burden Reminder (2024 Data)
Per UNICEF Supply Division (July 2026), citing UN-IGME 2024:
- Diarrhoea caused ~374,000 deaths in children under 5 in 2024
- ~40,000 deaths in children aged 5-9 in 2024
- Nearly 1.7 billion children fall ill with diarrhoea every year
- 93% of deaths concentrated in low- and middle-income countries
- ORS + zinc, if fully deployed, could prevent up to 93% of diarrhoea deaths
Summary: What Changed vs. What Stayed the Same
| Aspect | Status in 2024 WHO Guideline |
|---|---|
| Age scope of guidance | CHANGED - extended to 10 years (was 5 years) |
| Zinc dose | CHANGED - target is 5 mg/day; interim use of 20 mg/day until supply catches up |
| Zinc formulation | CHANGED - zinc gluconate preferred over zinc sulphate |
| Low-osmolarity ORS | Unchanged - still the cornerstone |
| Plan A / B / C framework | Unchanged - still the management backbone |
| Continued breastfeeding/feeding | Unchanged |
| No antimotility drugs | Unchanged |
| Selective antibiotic use | Unchanged |
Bottom line: The WHO December 2024 guideline is the authoritative current document. The single most clinically actionable update is the new zinc target dose of 5 mg/day (replacing 20 mg), driven by safety and tolerability evidence - though in practice, 20 mg/day remains standard until 5 mg formulations become commercially available. The coverage extension to age 10 fills a longstanding evidence gap.
This is a shared conversation. Sign in to Orris to start your own chat.