Neuromuscular blockade in details
Reading File
Finding Sources
Finding Sources
Searching PubMed
"neuromuscular blockade" AND reversal
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the content I need for a comprehensive, detailed response. Let me compose the full answer.
Neuromuscular Blockade - Comprehensive Review
1. The Neuromuscular Junction (NMJ) - Physiological Basis
The NMJ is the synapse between a motor nerve terminal and the skeletal muscle fiber. Understanding it is essential to understanding how neuromuscular blocking drugs (NMBDs) work.
Structure of the nicotinic ACh receptor:
The postjunctional nicotinic receptor consists of five protein subunits arranged around a central ion channel: two α subunits + β + δ + ε (in adult/mature junctional receptors). A fetal or extrajunctional isoform replaces the ε subunit with a γ subunit, producing a receptor with lower channel conductance but prolonged open-channel time.
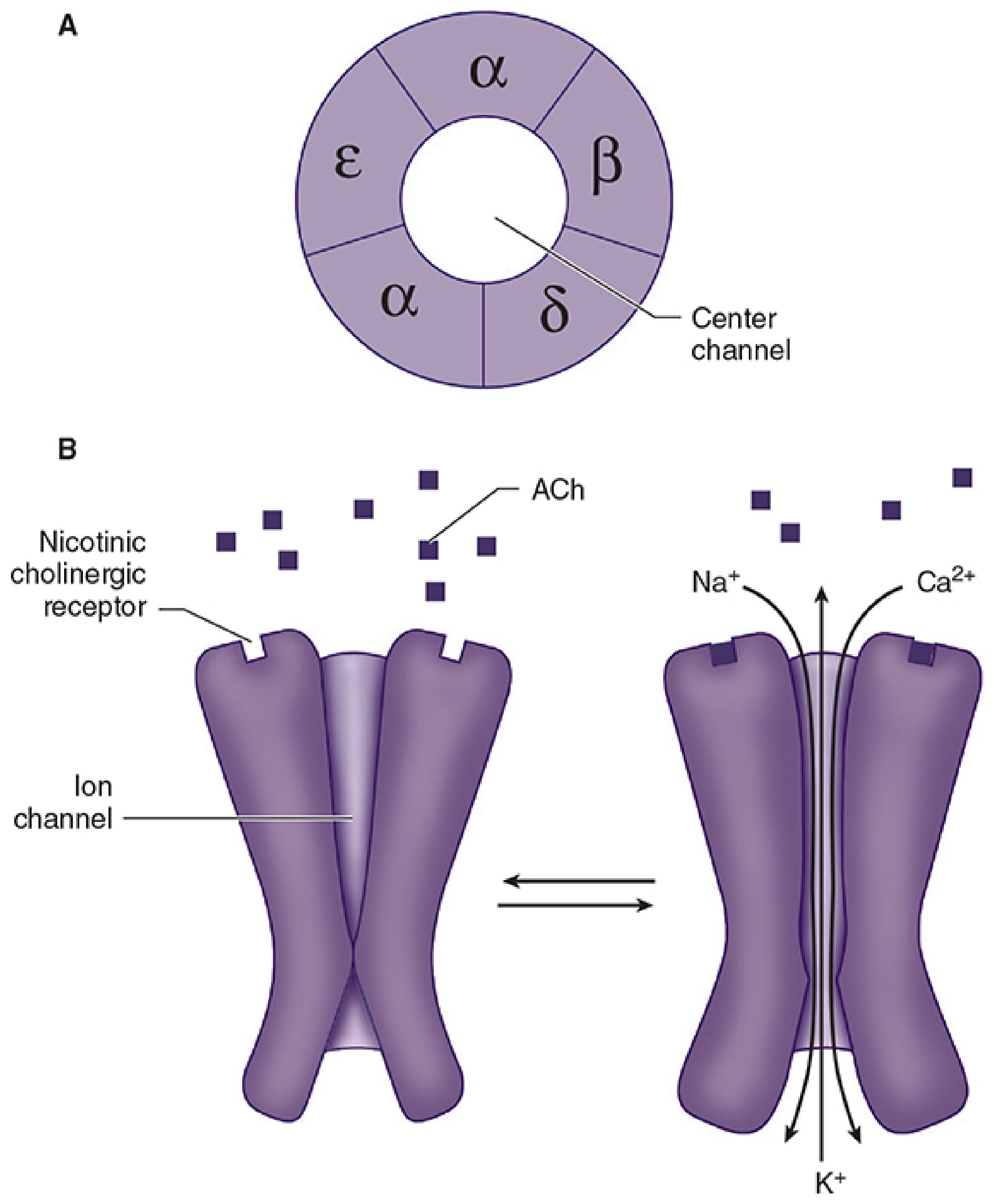
FIGURE: A - Five-subunit structure of the ACh receptor. B - Binding of ACh causes channel opening with influx of Na⁺ and Ca²⁺, and efflux of K⁺.
Sequence of normal transmission:
- Action potential arrives at nerve terminal → voltage-gated Ca²⁺ channels open
- Ca²⁺ influx triggers exocytosis of ACh vesicles (~200 quanta released per impulse; 10,000 molecules per quantum)
- ACh diffuses across the synapse and binds both α subunits simultaneously
- Conformational change opens the ion channel for ~1 ms (Na⁺ and Ca²⁺ in; K⁺ out)
- End-plate potential (EPP) generated → propagates as action potential along T-tubule
- Ca²⁺ release from sarcoplasmic reticulum → actin-myosin interaction → contraction
- ACh rapidly hydrolyzed by acetylcholinesterase (AChE) in the synaptic cleft
Margin of safety: The amount of ACh released and receptors activated normally far exceeds the minimum threshold - there is a ~10-fold margin of safety. This is reduced in Lambert-Eaton syndrome (decreased ACh release) and myasthenia gravis (decreased receptor number). - Morgan & Mikhail's Clinical Anesthesiology
2. Classification of Neuromuscular Blocking Drugs
All NMBDs are quaternary ammonium compounds - the positively charged nitrogen confers affinity for nicotinic ACh receptors. They are divided into two fundamentally distinct classes:
| Feature | Depolarizing | Nondepolarizing |
|---|---|---|
| Mechanism | ACh receptor agonist | Competitive antagonist |
| Fasciculations | Yes (initial) | No |
| Train-of-four (TOF) | Equal fade (no fade) | Progressive fade |
| Tetanic stimulation | Sustained tetanus | Fade + post-tetanic facilitation |
| Reversal | Cannot be reversed pharmacologically (phase I) | Reversed by neostigmine or sugammadex |
| Anticholinesterase effect | Prolongs block (phase I) | Reverses block |
| Prototype | Succinylcholine | Rocuronium, vecuronium, atracurium |
- Morgan & Mikhail's Clinical Anesthesiology, 7e
3. Depolarizing Neuromuscular Blockade
Succinylcholine (Suxamethonium)
The only depolarizing NMBD in clinical use. Structurally, it consists of two ACh molecules joined together (visible in the molecular structure below).

Mechanism:
- Binds ACh receptors and generates an action potential (agonist) - this causes the initial fasciculations
- Unlike ACh, it is resistant to AChE - concentration in the cleft does not fall rapidly
- Prolonged depolarization → perijunctional Na⁺ channels inactivate and cannot reopen until the end plate repolarizes
- The end plate cannot repolarize as long as succinylcholine occupies the receptor → flaccid paralysis (Phase I block)
Phase II block:
With increasing concentrations or prolonged infusion, the block converts from Phase I (depolarizing) to a Phase II block that resembles nondepolarizing blockade clinically, but the mechanism is poorly understood. Reversal with anticholinesterases is unpredictable and should be done cautiously.
Pharmacokinetics:
- Onset: 45-60 seconds (rapid - ideal for RSI)
- Duration: ~5-10 minutes (single bolus)
- Metabolism: Rapidly hydrolyzed by plasma butyrylcholinesterase (pseudocholinesterase) synthesized by the liver
- Standard intubating dose: 1-1.5 mg/kg IV; can also be given IM (4-5 mg/kg) for laryngospasm
Pseudocholinesterase deficiency:
- Heterozygous atypical gene (1:500): block prolonged to ~20-30 min
- Homozygous atypical (1:3000): block prolonged to 4-8 hours - requires mechanical ventilation until recovery
- The dibucaine number tests pseudocholinesterase quality:
- Normal: dibucaine inhibits enzyme by 80% → dibucaine number 80
- Homozygous atypical: inhibited by only 20% → dibucaine number 20
- Measures function, not quantity of enzyme
Adverse effects of succinylcholine:
| Side Effect | Mechanism | Clinical Significance |
|---|---|---|
| Hyperkalemia | Depolarization releases K⁺ normally ~0.5 mEq/L; massively elevated in burns, denervation, paraplegia, quadriplegia (extrajunctional receptor upregulation) | Life-threatening - avoid in these conditions |
| Malignant hyperthermia (MH) | Triggers in genetically susceptible patients (RyR1 mutation) - massive Ca²⁺ release | Treat with IV dantrolene 1 mg/kg (up to 10 mg/kg) |
| Bradycardia | Muscarinic receptor stimulation at sinus node | Especially in children; pretreat with atropine |
| Masseter spasm | Excessive jaw rigidity - may be early sign of MH | |
| Increased intraocular pressure | Extraocular muscle fasciculation | Relatively contraindicated in open-eye injuries |
| Increased intragastric pressure | Fasciculations of abdominal muscles | Offset by lower esophageal sphincter tone increase |
| Myalgias | From fasciculations | May pretreat with small dose nondepolarizing agent (defasciculating dose) |
| Phase II block | With high cumulative doses | Unpredictable duration |
Absolute contraindications: Burns (>24h), crush injuries, denervation/paraplegia, prolonged immobilization, MH susceptibility, muscular dystrophy, personal/family history of MH
- Sabiston Textbook of Surgery; Goldman-Cecil Medicine; Morgan & Mikhail's Clinical Anesthesiology
4. Nondepolarizing Neuromuscular Blockade
Mechanism:
- Bind to one or both α subunits of the nicotinic ACh receptor without activating the ion channel
- Competitive antagonism - block is overcome by increasing ACh at the junction
- Also bind presynaptic α3β2 ACh receptors, reducing ACh release with subsequent nerve stimulation (causes fade on TOF)
- Neuromuscular blockade occurs even if only one α subunit is blocked
Sequence of paralysis (competitive blockers):
Small, rapidly moving muscles (eyes, jaw, larynx) are paralyzed first, then limbs/trunk, and finally intercostal muscles and diaphragm (apnea). Recovery occurs in reverse order - the diaphragm recovers first.
Classification by Duration and Chemical Class
Chemical classes:
- Benzylisoquinolines - atracurium, cisatracurium, mivacurium (older: tubocurarine, doxacurium)
- Aminosteroids - rocuronium, vecuronium, pancuronium (older: pipecuronium)
- Asymmetric mixed-onium chlorofumarates - gantacurium (investigational)
Individual Drugs
Intermediate-Acting (20-50 minutes)
Rocuronium
- ED₉₅: 0.3 mg/kg; intubating dose: 0.6 mg/kg (intermediate onset ~3 min) or 1.2 mg/kg for RSI (onset ~60 sec - equivalent to succinylcholine)
- Eliminated primarily via liver (biliary excretion) - prolonged in hepatic disease
- Vagolytic at high doses (mild tachycardia)
- Best reversed by sugammadex (can reverse even profound block in 3 min)
- Drug of choice for RSI when succinylcholine is contraindicated
Vecuronium
- ED₉₅: 0.05 mg/kg; intubating dose: 0.1 mg/kg
- Eliminated by liver (50-60%) and kidney (40-50%) - use with caution in organ failure
- Minimal cardiovascular side effects - no histamine release, no vagolysis
- Metabolite (3-OH vecuronium) has ~50% activity - can accumulate with prolonged infusion in ICU
Atracurium
- Intubating dose: 0.5 mg/kg
- Unique: metabolized by Hofmann elimination (spontaneous chemical degradation at physiological pH and temperature) + plasma esterase hydrolysis - independent of hepatic and renal function
- Metabolite laudanosine can cause CNS excitation/seizures in high concentrations (theoretical concern in ICU)
- Releases histamine - can cause flushing, hypotension; administer slowly
- Preferred in severe renal/hepatic failure
Cisatracurium
- The 1R cis-1'R cis isomer of atracurium
- Same Hofmann elimination pathway - organ-independent metabolism
- 3-5x more potent than atracurium; much less histamine release than atracurium
- Preferred over atracurium in ICU settings (less laudanosine production per equivalent dose)
- Intubating dose: 0.15-0.2 mg/kg
Mivacurium
- Shortest acting nondepolarizing agent (15-20 min); metabolized by pseudocholinesterase
- Prolonged in pseudocholinesterase deficiency (like succinylcholine)
- Releases histamine
Long-Acting (>60 minutes)
Pancuronium
-
Intubating dose: 0.1 mg/kg; duration 60-120 min
-
Excreted mainly by kidney (60-80% unchanged) - prolonged in renal failure
-
Has vagolytic and sympathomimetic effects → tachycardia and hypertension
-
No histamine release
-
Low cost; used less frequently now due to cardiovascular effects and long duration
-
Goodman & Gilman's Pharmacological Basis of Therapeutics; Morgan & Mikhail's Clinical Anesthesiology; Sabiston Textbook of Surgery; Goldman-Cecil Medicine
5. Monitoring Neuromuscular Blockade
Peripheral nerve stimulators are used to objectively assess depth of block. A nerve (ulnar, facial, posterior tibial) is stimulated and the muscle response observed.
Stimulation Patterns
Train-of-Four (TOF):
- 4 supramaximal stimuli at 2 Hz, every 10-15 seconds
- TOF ratio = T4/T1 amplitude
- Nondepolarizing block: progressive fade (T4 fades more than T1) due to presynaptic receptor blockade reducing ACh mobilization
- Depolarizing (Phase I) block: equal depression of all 4 twitches (no fade)
- TOF ratio <0.9 = residual paralysis (clinically relevant)
- TOF count of 0 = profound block; count 1-2 = deep block; count 3-4 = moderate block
Post-Tetanic Count (PTC):
- Used to assess profound block (TOF count = 0)
- 50 Hz tetanus for 5 sec, then single twitches at 1 Hz
- Used to predict time to spontaneous recovery or reversal with sugammadex
Double Burst Stimulation (DBS):
- Two short bursts of 50 Hz tetanus separated by 750 ms
- More sensitive than TOF for detecting residual block by tactile assessment
Key clinical point: Residual neuromuscular blockade (RNMB) is the most common complication - occurs in ~40% of patients when not properly reversed. RNMB is defined as TOF ratio <0.9 and may cause upper airway obstruction, aspiration, and respiratory failure. - Barash, Cullen & Stoelting's Clinical Anesthesia
6. Reversal of Neuromuscular Blockade
A. Anticholinesterase Agents (Indirect - ACh buildup)
Neostigmine (most commonly used)
- Inhibits AChE → ACh accumulates → competitively displaces nondepolarizing NMBD from receptor
- Dose: 0.04-0.07 mg/kg (max ~5 mg)
- Must always be combined with an anticholinergic (glycopyrrolate 0.2 mg per 1 mg neostigmine, or atropine) to prevent muscarinic side effects (bradycardia, bronchospasm, increased secretions)
- Limitations:
- Ineffective against deep/profound block (requires at least TOF count 2-3)
- Ceiling effect - increasing dose does not provide more reversal once AChE is fully inhibited
- Has an "appropriate" dose ceiling - paradoxically, too much neostigmine can cause weakness by causing persistent depolarization (neostigmine-induced weakness)
- Takes 10-20 min for full effect
Edrophonium
- Also an AChE inhibitor; faster onset (1-2 min) but shorter duration
- Dose: 0.5-1.0 mg/kg; combine with atropine (onset matched)
- Less reliable than neostigmine for dense blocks
B. Selective Relaxant Binding Agent: Sugammadex
A revolutionary advance - a modified γ-cyclodextrin that directly encapsulates steroidal NMBDs (rocuronium > vecuronium) in a tight 1:1 complex, rapidly removing them from the neuromuscular junction.
Mechanism: Does not act on AChE or receptors - it simply encapsulates the drug molecule, creating a very stable complex excreted by kidneys.
Dosing by depth of block:
| Block Depth | TOF | Sugammadex Dose |
|---|---|---|
| Moderate | TOF count ≥ 2 | 2 mg/kg |
| Deep | Post-tetanic count 1-2 | 4 mg/kg |
| Immediate reversal (RSI rescue) | Complete block (<3 min after 1.2 mg/kg rocuronium) | 16 mg/kg |
Advantages over neostigmine:
- No anticholinergic needed (no muscarinic effects)
- Can reverse profound block - even immediately after RSI dose of rocuronium
- No ceiling effect
- Faster, more predictable reversal
- Preferred for patients with OSA (reduced postoperative pulmonary complications)
Side effects: Hypersensitivity/anaphylaxis (rare ~0.3%); bradycardia; some effect on coagulation (mild prolongation of aPTT/PT - clinically monitored) - 2025 meta-analysis, PMID [40269695]
Important interactions:
- Toremifene (antiestrogen) and fusidic acid can displace rocuronium from sugammadex complex - reduces efficacy
- Re-dosing of rocuronium after sugammadex: wait ≥24h for full dose; shorter-acting NMBDs (atracurium, cisatracurium) can be used immediately after sugammadex
Recent evidence (2025): A systematic review and meta-analysis comparing sugammadex vs. neostigmine showed sugammadex provides faster, more complete reversal with significantly lower rates of RNMB, PONV, and postoperative respiratory events - PMID 40754949
7. Drug Interactions
| Drug | Effect on Depolarizing Block | Effect on Nondepolarizing Block |
|---|---|---|
| Antibiotics (aminoglycosides, clindamycin, polymyxin) | Potentiate | Potentiate |
| Inhalational anesthetics (volatile agents) | Potentiate | Potentiate (dose-dependent) |
| Anticonvulsants (phenytoin, carbamazepine) | Variable | Resistance (increased dose needed) |
| Magnesium sulfate | Potentiate | Potentiate (decreases ACh release) |
| Calcium channel blockers | Potentiate | Potentiate |
| Cholinesterase inhibitors (neostigmine, pyridostigmine) | Potentiate | Reverse/antagonize |
| Lithium | Potentiate | Potentiate |
| Ketamine | Variable | Potentiate |
| Dantrolene | Variable | Potentiate |
| Local anesthetics | Potentiate | Potentiate |
Key points:
-
Patients on anticonvulsants require higher NMBDs doses but have accelerated recovery
-
Magnesium (used in obstetrics for eclampsia) markedly potentiates nondepolarizing block - reduce doses by 25-50%
-
Aminoglycosides cause neuromuscular blockade by reducing ACh release (presynaptic Ca²⁺ channel inhibition) - can be reversed by IV calcium
-
Patients with myasthenia gravis are exquisitely sensitive to nondepolarizing NMBDs (10-fold); resistant to succinylcholine
-
Morgan & Mikhail's Clinical Anesthesiology; Goldman-Cecil Medicine
8. Receptor Upregulation and Downregulation - Special States
| Condition | Receptor Change | Response to Succinylcholine | Response to Nondepolarizing |
|---|---|---|---|
| Denervation, burns, immobilization, prolonged ICU | Upregulation (extrajunctional receptors) | Exaggerated hyperkalemia | Resistance (need higher doses) |
| Myasthenia gravis | Downregulation | Resistance | Profound sensitivity |
| Lambert-Eaton syndrome | Normal receptors, decreased ACh release | Normal/increased sensitivity | Increased sensitivity |
9. Specific Clinical Applications
Rapid Sequence Intubation (RSI)
- Goal: secure airway quickly in patients at risk for pulmonary aspiration
- Classic: succinylcholine 1.5 mg/kg (onset 45-60 sec) - gold standard
- Alternative: rocuronium 1.2 mg/kg (onset ~60 sec) - preferred when succinylcholine is contraindicated; must have sugammadex 16 mg/kg immediately available as rescue
- Modified RSI with rocuronium + sugammadex is now widely practiced - Morgan & Mikhail's Clinical Anesthesiology
ICU Neuromuscular Blockade
- Used for: mechanical ventilation optimization, ARDS, status epilepticus refractory to sedation, tetanus, shivering during therapeutic hypothermia
- Cisatracurium is preferred in ICU (Hofmann elimination - no organ dependency; less laudanosine than atracurium)
- Risk: Critical illness myopathy/polyneuropathy - especially with concomitant corticosteroids (prolonged paralysis)
- Drug holiday ("train-of-four holiday") with daily monitoring recommended
Cardiac Surgery
- Nondepolarizing NMBDs preferred; pancuronium used historically (vagolysis offsets bradycardia from opioids/beta-blockers)
- Cisatracurium or vecuronium preferred when hemodynamic neutrality required
10. Residual Neuromuscular Blockade (RNMB)
- Defined as TOF ratio <0.9 at extubation
- Incidence: ~40% without proper reversal
- Risk factors: elderly, obese, obstructive sleep apnea, pulmonary disease, long-acting NMBDs, inadequate reversal
- Clinical consequences: upper airway obstruction, aspiration, hypoxia, reintubation, PONV
- Prevention: quantitative TOF monitoring (acceleromyography or electromyography), confirm TOF ratio ≥0.9 before extubation, prefer sugammadex over neostigmine for reversal
- Current recommendations strongly favor quantitative monitoring rather than clinical signs alone (head lift for 5 seconds, grip strength, tongue depressor test have poor sensitivity for detecting TOF ratios between 0.7-0.9)
11. Summary Table: Key NMBDs at a Glance
| Drug | Class | Onset | Duration | Metabolism | Key Features |
|---|---|---|---|---|---|
| Succinylcholine | Depolarizing | 45-60 sec | 5-10 min | Plasma cholinesterase | RSI; many contraindications |
| Rocuronium | Amino steroid | 1-3 min (0.6 mg/kg); ~60 sec (1.2 mg/kg) | 30-45 min | Liver/bile | RSI alternative; reversible by sugammadex |
| Vecuronium | Amino steroid | 3-5 min | 25-40 min | Liver + kidney | Hemodynamically neutral |
| Cisatracurium | Benzylisoquinoline | 5-7 min | 45-60 min | Hofmann elimination | Organ-independent; preferred ICU |
| Atracurium | Benzylisoquinoline | 3-5 min | 25-35 min | Hofmann + esterase | Organ-independent; histamine release |
| Pancuronium | Amino steroid | 3-5 min | 60-120 min | Kidney (60-80%) | Tachycardia; avoid in renal failure |
| Mivacurium | Benzylisoquinoline | 2-3 min | 15-20 min | Plasma cholinesterase | Shortest ND; histamine release |
Key Takeaways
- NMBDs do not cause unconsciousness or amnesia - awareness under anesthesia remains a risk
- Succinylcholine is unmatched for speed of onset and ultra-short duration for RSI, but carries significant contraindications
- Rocuronium at 1.2 mg/kg with sugammadex 16 mg/kg available provides a viable alternative to succinylcholine for RSI
- Cisatracurium is the preferred NMBD in ICU/organ failure patients due to organ-independent Hofmann elimination
- RNMB is common (~40%) and clinically dangerous - quantitative TOF monitoring and appropriate reversal (preferably sugammadex) are the standard of care
- Sugammadex has replaced neostigmine as the preferred reversal agent for steroidal NMBDs in many centers - 2025 meta-analysis confirms superior outcomes
Sources:
- Morgan & Mikhail's Clinical Anesthesiology, 7e
- Goodman & Gilman's Pharmacological Basis of Therapeutics
- Katzung's Basic and Clinical Pharmacology, 16th Edition
- Barash, Cullen & Stoelting's Clinical Anesthesia, 9e
- Sabiston Textbook of Surgery
- Goldman-Cecil Medicine, 2-Volume Set
- Recent meta-analyses: Sugammadex vs. neostigmine [PMID 40754949] and sugammadex coagulation effects [PMID 40269695]
This is a shared conversation. Sign in to Orris to start your own chat.