Cerebral palsy
Reading File
Finding Sources
Searching PubMed
"cerebral palsy"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Cerebral Palsy
Definition
Cerebral palsy (CP) is defined as a group of permanent disorders of the development of movement and posture, causing activity limitation, that are attributed to non-progressive disturbances that occurred in the developing fetal or infant brain. Onset is before age 2 years. Despite the brain lesion being static and non-progressive, the musculoskeletal consequences (contractures, deformities, scoliosis, hip dislocation) do worsen over time.
- Bradley and Daroff's Neurology in Clinical Practice, p. 2040
- Goldman-Cecil Medicine, p. 4048
Epidemiology
- Prevalence: approximately 2-3 per 1,000 live births
- Most common physical disability of childhood
- Prevalence initially decreased in the 1950s-60s with improved management of Rh incompatibility and obstetric care
- Improved survival of premature/low-birth-weight infants has not significantly increased overall prevalence in population-based studies
Etiology & Risk Factors
Cause is often not identifiable, but known causes include:
| Category | Examples |
|---|---|
| Prematurity | Most common; periventricular leukomalacia (PVL) |
| Perinatal hypoxia-ischemia | Birth asphyxia in term/near-term infants |
| Prenatal/intrauterine | Congenital brain malformations (e.g., absent corpus callosum), TORCH infections |
| Perinatal infections | Toxoplasmosis, rubella, CMV, herpes simplex |
| Vascular | Perinatal stroke, intracranial hemorrhage |
| Metabolic/toxic | Kernicterus (bilirubin toxicity to basal ganglia) |
| Genetic | ~20% idiopathic; ~1/3 of idiopathic cases have de novo copy number variants; ~14% may have single-gene disorders on whole exome sequencing |
| Post-natal | Meningitis, anoxic injury in infancy |
Note: ~20% of cases remain idiopathic. A growing fraction have underlying genetic etiologies, including inborn errors of metabolism - some of which are treatable.
Classification
1. Physiologic (Motor Type)
Spastic (80% of all cases) - injury to the pyramidal (corticospinal) tracts
- Velocity-dependent increase in muscle tone with passive stretch
- Co-contraction of antagonist muscle groups
- Leads to joint contractures, subluxation, degeneration
- Collagen deposition (type I) in endomysium of affected muscle causing fibrosis
Dyskinetic / Extrapyramidal (involves basal ganglia/cerebellum)
- Dystonia - sustained or repetitive muscle contractions, twisting/abnormal postures
- Athetosis - slow, writhing, involuntary movements
- Chorea - rapid, irregular, involuntary movements
- Ataxia - cerebellar-type with balance/coordination problems
- Spastic diplegia usually detected at 8-10 months; hemiplegia ~20 months; athetoid type after 24 months
Mixed - combination of movement disorder types
2. Anatomic (Topographic) Distribution
| Type | Distribution | Key Features |
|---|---|---|
| Hemiplegia | One side, arm > leg | ~30% of CP; sensory changes common; leg-length discrepancy possible |
| Diplegia | All 4 limbs, legs >> arms | ~50% of CP; most common in premature infants; usually normal intelligence; most walk by age 4 |
| Quadriplegia | All 4 limbs equally | Significant cognitive deficits frequent; head/neck control usually present |
| Total body | All limbs + head/neck | Profound cognitive deficits; drooling, dysarthria, dysphagia; requires full-time care |
3. Functional Classification - GMFCS
The Gross Motor Function Classification System (GMFCS) is the most widely used system, stratifying children by self-initiated movement with emphasis on sitting, walking, and wheeled mobility:
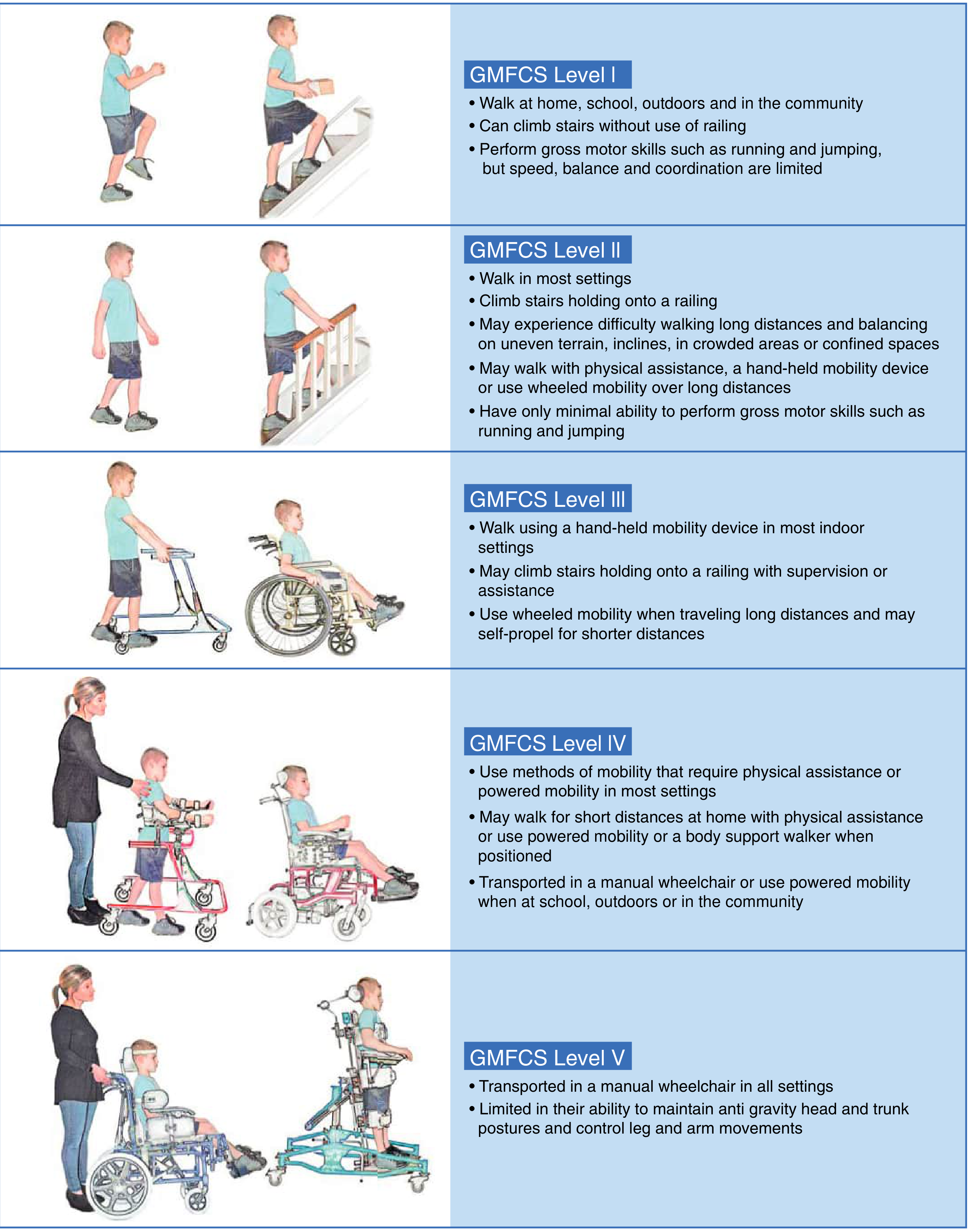
- Level I - Walks without restrictions; limitations in advanced gross motor skills
- Level II - Walks with limitations; difficulty with uneven terrain, long distances
- Level III - Walks with hand-held mobility device; wheelchair for long distances
- Level IV - Self-mobility limited; requires powered mobility or physical assistance
- Level V - Transported in manual wheelchair; very limited self-mobility
GMFCS has been shown to be predictive of hip dislocation risk. It is reliable and stable for children up to 18 years.
The Manual Abilities Classification System (MACS) is an analogous 5-level system for upper-extremity function in children 4-18 years.
Neuroimaging
Brain MRI is preferred over head ultrasound and is considered essential in evaluation:
- Spastic diplegia: periventricular leukomalacia (PVL) - white matter injury near ventricles
- Spastic hemiplegia: perinatal stroke evidence
- Dyskinetic CP: involvement of thalamus and basal ganglia (especially lenticular nucleus) in ~70% of cases; globus pallidus involvement in kernicterus
- Normal MRI (~13% of dyskinetic CP): raises concern for underlying genetic/metabolic condition requiring further workup
Diagnosis
CP is a clinical diagnosis based on:
- History - perinatal/postnatal brain injury risk factors; exposure history
- Physical examination - abnormal tone, deep tendon reflexes, pathological reflexes, motor delay
- Neuroimaging - MRI brain to define type and extent of injury
Differentiating Genetic from Acquired CP (3-step approach):
- Step 1: Does history + examination + MRI fit a known mechanism of brain injury?
- Step 2: If MRI is normal or atypical, or course is unusual, pursue genetic workup (chromosomal microarray, metabolic screen, whole exome sequencing)
- Step 3: Consider treatable metabolic mimics (dopa-responsive dystonia, neurotransmitter disorders, some leukodystrophies)
Clinical Features & Comorbidities
- Exaggerated deep tendon reflexes, clonus, pathological reflexes (Babinski)
- Spasticity leading to progressive contractures and deformity
- ~50% have cognitive impairment (sometimes severe)
- Epilepsy (~25-35%)
- Speech and language disorders (dysarthria, dysphagia)
- Visual impairment, strabismus
- Drooling
- Pain (increasingly recognized, particularly in adults)
- Bladder dysfunction
Treatment
CP treatment is multidisciplinary and targets motor function, spasticity, pain, and functional independence.
Spasticity Management
| Approach | Details |
|---|---|
| Physical/occupational therapy | Core of management; gait training, stretching |
| Oral medications | Baclofen, benzodiazepines, tizanidine, trihexyphenidyl (for dystonia) |
| Botulinum neurotoxin (BoNT/Botox) | Targeted intramuscular chemodenervation; especially useful for focal spasticity |
| Intrathecal baclofen (ITB) | Pump delivers baclofen directly to CSF; highly effective for generalized spasticity; GMFCS III-V |
| Selective dorsal rhizotomy (SDR) | Resection of 25-40% of abnormal dorsal nerve rootlets; ideal candidates are age 4-10, GMFCS I-III, with PVL on MRI; irreversible |
| Deep brain stimulation (DBS) | Primarily for dyskinetic/dystonic CP |
SDR is cheaper than ITB long-term and has shown functional ambulation gains in GMFCS I-III patients with continued benefit into adolescence.
Orthopedic Interventions
- Hip surveillance - regular radiographs; higher risk at GMFCS IV-V; adductor releases to prevent hip subluxation/dislocation
- Scoliosis/spinal deformity - common in quadriplegic/total body CP; managed with bracing or spinal fusion
- Lower limb surgery - hamstring lengthening, calf muscle lengthening, tibialis posterior transfer; aim for plantigrade foot and improved gait
- Gait analysis - used as an essential tool to guide surgical planning; assesses kinetics and kinematics
Goals by Severity
- Ambulatory patients (GMFCS I-III): Optimize gait, prevent/correct contractures, maximize independence
- Non-ambulatory (GMFCS IV-V): Straight spine, level pelvis, seated hip stability (90° flexion), plantigrade feet, appropriate wheelchair seating
Recent Evidence Updates
Three recent systematic reviews (2025) worth noting:
- Extracorporeal shock wave therapy for motor function in CP - emerging evidence for motor outcomes (PMID 40481808)
- Genetic findings in CP have clinical actionability in a clinically meaningful proportion of patients, supporting expanded genetic testing (PMID 39621323, JAMA Pediatrics 2025)
- Pain in adults with CP is common and underrecognized (PMID 39937705)
Sources: Campbell's Operative Orthopaedics 15th Ed 2026 | Bradley and Daroff's Neurology in Clinical Practice | Goldman-Cecil Medicine | Miller's Review of Orthopaedics 9th Ed
This is a shared conversation. Sign in to Orris to start your own chat.