Wydm by effector cells in cns
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
In central nervous system
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Here is a consolidated answer on what effector cells release in the CNS:
What Effector Cells Release in the CNS
The CNS is an immune-privileged site, but during inflammation (e.g., multiple sclerosis, viral encephalitis, autoimmune disease), activated effector cells infiltrate or are resident there and release a range of soluble mediators.
1. T Cells (CD4+ and CD8+)
CD4+ Th1 cells are the dominant effectors in most CNS autoimmune conditions. They release:
| Mediator | Effect in CNS |
|---|---|
| IFN-γ (interferon-gamma) | Activates microglia/macrophages; upregulates MHC II on APCs |
| TNF-β (lymphotoxin) | Direct cytotoxic injury to oligodendrocytes and axons |
| TNF-α | Promotes demyelination, oligodendrocyte death |
| IL-2 | T cell autocrine growth factor; sustains effector response |
CD4+ Th17 cells also infiltrate the CNS and release:
- IL-17 - drives neutrophil recruitment, disrupts blood-brain barrier
- IL-22 - inflammatory, barrier disruption
CD8+ cytotoxic T cells (CTLs) kill target cells by releasing:
- Perforin - forms pores in target cell membranes
- Granzymes (A and B) - serine proteases that trigger apoptosis in target cells (neurons, oligodendrocytes)
- IFN-γ - antiviral and pro-inflammatory
Key textbook quote: "Activated T cells and the microglia-macrophages can contribute to tissue injury via non-antigen-restricted mechanisms. Each of these cell types releases an array of soluble factors... Cytokines characteristic of T cells include interleukin 2 (IL-2), interferon gamma (IFN-γ), and tumor necrosis factor β (TNF-β; lymphotoxin)."
- Bradley and Daroff's Neurology in Clinical Practice
2. Microglia / Macrophages (Resident + Recruited)
These are the major innate effector cells of the CNS. When activated ("M1 state"), they release:
| Mediator | Effect |
|---|---|
| TNF-α | Oligodendrocyte death, demyelination, BBB disruption |
| IL-1β | Pro-inflammatory, promotes T cell activation, fever |
| IL-6 | Drives acute-phase response; promotes Th17 differentiation |
| IL-12 | Drives Th1 polarization of infiltrating T cells |
| Reactive oxygen species (ROS) | Oxidative damage to myelin and axons |
| Nitric oxide (NO) | Produced via iNOS; blocks axonal conduction, causes demyelination |
| Proteases (MMP-9) | Degrade extracellular matrix; facilitate immune cell entry through BBB |
| Complement proteins | Opsonization and lysis of target cells |
3. Astrocytes (Reactive Astrogliosis)
In the reactive state, astrocytes release:
- IL-6, IL-1β - amplify inflammatory signals
- Chemokines (CXCL10, CCL2) - recruit T cells and monocytes into CNS
- Glutamate (excess) - excitotoxicity and neuronal death
- VEGF - promotes vascular permeability
4. NK Cells
NK cells can enter the inflamed CNS and release:
- Perforin + Granzymes - kill infected or stressed neurons
- IFN-γ - activates macrophages and microglia
- TNF-α - cytotoxic effects
Summary Table
| Cell Type | Key Mediators Released |
|---|---|
| CD4+ Th1 | IFN-γ, TNF-α/β, IL-2 |
| CD4+ Th17 | IL-17, IL-22 |
| CD8+ CTL | Perforin, Granzymes, IFN-γ |
| Microglia/Macrophage | TNF-α, IL-1β, IL-6, IL-12, ROS, NO, MMP-9 |
| Astrocyte | IL-6, IL-1β, Chemokines, Glutamate |
| NK Cell | Perforin, Granzymes, IFN-γ, TNF-α |
Clinical relevance: In MS, the dominant pathway is myelin-specific Th1/Th17 cells entering the CNS and releasing IFN-γ and IL-17, which activate microglia/macrophages, leading to demyelination through TNF-α, ROS, and NO. This is the rationale for therapies targeting IFN-β, TNF blockade, and B-cell depletion (rituximab, ocrelizumab).
Pregangilonic sympathetic outflow detailed
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a detailed breakdown of preganglionic sympathetic outflow:
Preganglionic Sympathetic Outflow - Detailed
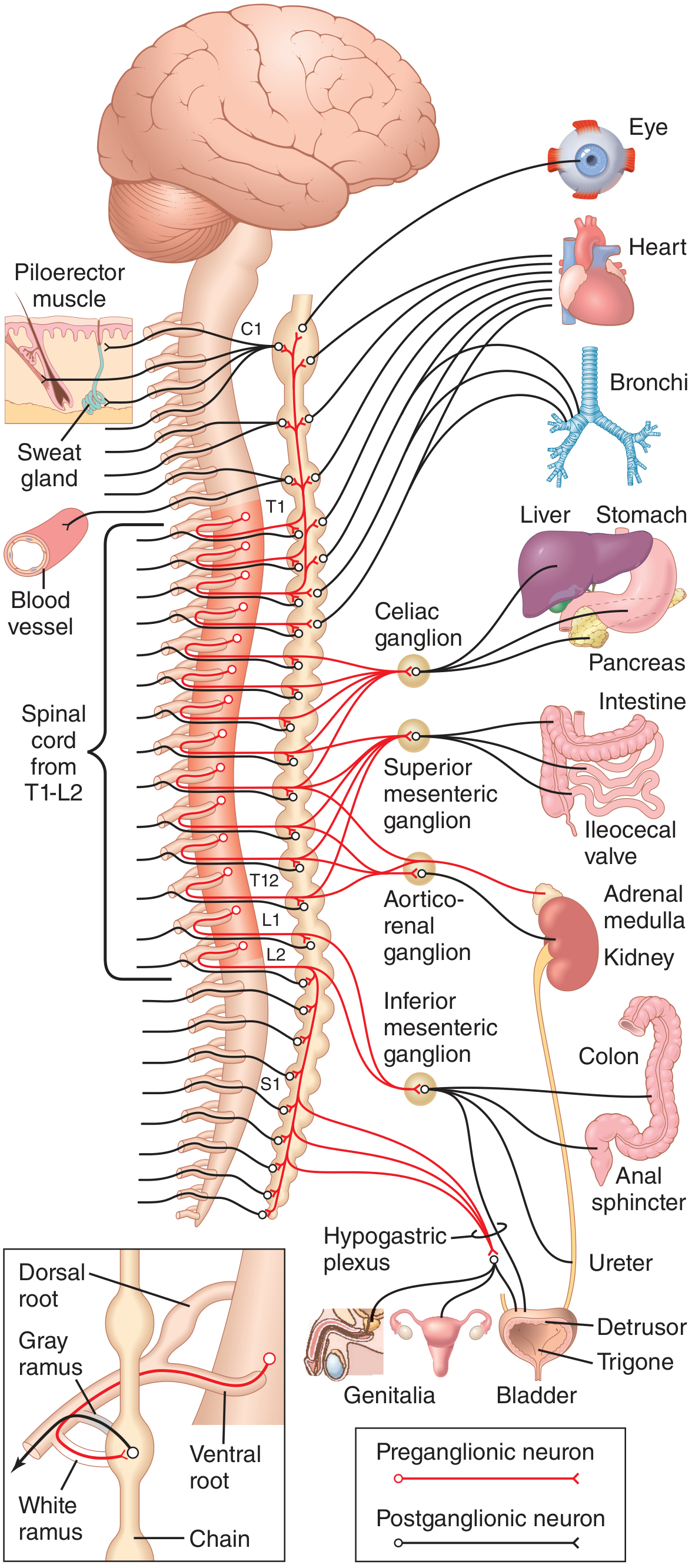
1. Origin - Cell Bodies
- Located in the intermediolateral cell column (IML) / lateral horn of the spinal cord gray matter
- Spans segments T1 to L2 (some texts say T1-L3)
- This is why the sympathetic system is called the thoracolumbar outflow
- White rami communicantes exist only at T1-L2 levels
2. Fiber Characteristics
| Property | Detail |
|---|---|
| Myelination | Lightly myelinated (B fibers) |
| Color | White (contribute to white rami communicantes) |
| Length | Short (ganglia lie close to spinal cord) |
| Neurotransmitter | Acetylcholine (ACh) |
| Receptor on postganglionic | Nicotinic (N2) receptors |
| Divergence | Each preganglionic neuron branches onto ~200 postganglionic neurons - allowing widespread body-wide effects |
3. Path from Spinal Cord to Ganglion
Step-by-step route:
- Cell body in IML of lateral horn (T1-L2)
- Axon exits via the ventral (anterior) root
- Travels briefly in the spinal nerve
- Diverges into the white ramus communicans (myelinated, so white)
- Enters the paravertebral sympathetic chain ganglion
4. Three Fates After Entering the Sympathetic Chain
Once inside a paravertebral ganglion, the preganglionic fiber has three options:
| Fate | Description |
|---|---|
| 1. Synapse at same level | Synapses with postganglionic neuron in the ganglion it entered |
| 2. Ascend or descend in the chain | Travels up or down to synapse in a ganglion at a different vertebral level |
| 3. Pass through without synapsing | Exits the chain, travels via splanchnic nerves to synapse in a prevertebral ganglion in the abdomen |
"After entering a paravertebral ganglion, a preganglionic sympathetic axon may (1) synapse within that segmental paravertebral ganglion, (2) travel up or down the sympathetic chain to synapse within a neighboring paravertebral ganglion, or (3) pass through the chain and then through one of the sympathetic nerves radiating outward from the chain, finally synapsing in a peripheral sympathetic (prevertebral) ganglion."
- Medical Physiology (Boron & Boulpaep)
5. Segmental Distribution of Preganglionic Outflow
| Spinal Level | Target Region |
|---|---|
| T1 | Head (ascends to superior cervical ganglion) |
| T2 | Neck |
| T3-T6 | Thorax (heart, lungs, bronchi) |
| T7-T11 | Abdomen (stomach, liver, pancreas, small intestine) |
| T12, L1, L2 | Legs and pelvic organs |
The distribution is partly determined by the embryological origin of the organ. For example, the heart receives fibers from the neck region of the sympathetic chain because the heart originally developed in the neck of the embryo before descending into the thorax.
- Guyton & Hall Textbook of Medical Physiology
6. Ganglia Where Preganglionic Fibers Synapse
A. Paravertebral (Sympathetic Chain) Ganglia
- 22-23 ganglia arranged bilaterally along the vertebral column from cervical to coccyx
- Key named ganglia:
| Ganglion | Formed From | Supplies |
|---|---|---|
| Superior cervical ganglion | Fusion of C1-C4 | Head and neck (pupil dilator, eyelid elevator, sweat glands of face) |
| Middle cervical ganglion | C5-C6 | Heart, thyroid |
| Stellate (cervicothoracic) ganglion | C7-C8 + T1 fused | Heart, lungs, upper limb |
| Thoracic ganglia (T2-T12) | Individual | Thoracic wall, intercostals |
| Lumbar ganglia | L1-L2 | Lower limbs |
| Coccygeal (ganglion impar) | Right + left chains merge | Perineum |
B. Prevertebral (Collateral) Ganglia
- Lie anterior to the aorta, near the roots of major visceral arteries
- Preganglionic fibers reach them via splanchnic nerves (bypass the chain without synapsing):
| Splanchnic Nerve | Spinal Origin | Synapse In |
|---|---|---|
| Greater splanchnic | T5-T9 | Celiac ganglion |
| Lesser splanchnic | T10-T11 | Superior mesenteric + aorticorenal ganglia |
| Least splanchnic | T12 | Aorticorenal ganglion |
| Lumbar splanchnic | L1-L2 | Inferior mesenteric ganglion / hypogastric plexus |
7. Special Case: Adrenal Medulla
- Preganglionic fibers from T5-T11 travel via greater splanchnic nerves all the way to the adrenal medulla without synapsing
- The chromaffin cells of the adrenal medulla are modified postganglionic neurons (embryologically derived from neural crest)
- These cells secrete epinephrine (80%) and norepinephrine (20%) directly into the bloodstream in response to ACh from preganglionic fibers
- This is why the adrenal medulla acts like a "sympathetic ganglion released into the blood"
"Preganglionic sympathetic nerve fibers pass without synapsing, all the way from the intermediolateral horn cells, through the sympathetic chains, through the splanchnic nerves, into the adrenal medullae. These secretory cells embryologically are derived from nervous tissue and are actually postganglionic neurons."
- Guyton & Hall
8. White vs. Gray Rami Communicantes
| Feature | White Ramus Communicans | Gray Ramus Communicans |
|---|---|---|
| Fiber type | Myelinated preganglionic | Unmyelinated postganglionic |
| Color | White | Gray |
| Direction | Spinal nerve → sympathetic chain | Sympathetic chain → spinal nerve |
| Levels present | T1-L2 only | All spinal cord levels (C2 to coccyx) |
| Function | Carries preganglionic fibers into ganglia | Carries postganglionic fibers back to spinal nerves |
Summary Flowchart
IML lateral horn (T1-L2)
↓
Ventral root → Spinal nerve → White ramus communicans
↓
Sympathetic chain ganglion
├─ Synapse here → postganglionic via gray ramus → body wall, skin, blood vessels, sweat glands
├─ Ascend/Descend chain → synapse in cervical/lumbar ganglia → head, neck, legs
└─ Pass through (no synapse) → splanchnic nerves → prevertebral ganglia → abdominal/pelvic viscera
↓ (special)
Adrenal medulla → epinephrine/norepinephrine released
Sources: Guyton & Hall Textbook of Medical Physiology; Medical Physiology (Boron & Boulpaep); Gray's Anatomy for Students; Goodman & Gilman's Pharmacological Basis of Therapeutics
Breif me about sympathetic trunks
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
Reading File
Here is a concise but thorough brief on the sympathetic trunks:
Sympathetic Trunks - Brief
Overview
The sympathetic trunks (also called sympathetic chains) are two bilateral paravertebral nerve cords running alongside the vertebral column on each side. They are the highway that allows preganglionic fibers emerging only from T1-L2 to reach every spinal level in the body - from head down to the coccyx.
"On each side, a paravertebral sympathetic trunk extends from the base of the skull to the inferior end of the vertebral column where the two trunks converge anteriorly to the coccyx at the ganglion impar."
- Gray's Anatomy for Students
Structure
| Feature | Detail |
|---|---|
| Number | Two (one on each side of vertebral column) |
| Extent | Base of skull → coccyx |
| Ganglia | ~22-23 paravertebral ganglia on each side |
| Termination | Both trunks merge anteriorly to coccyx at the ganglion impar |
| Position | Anterior to transverse processes / anterolateral to vertebral bodies |
| Connections to spinal nerves | Via white rami (T1-L2 only) and gray rami (all levels) |
Regional Parts and Their Ganglia
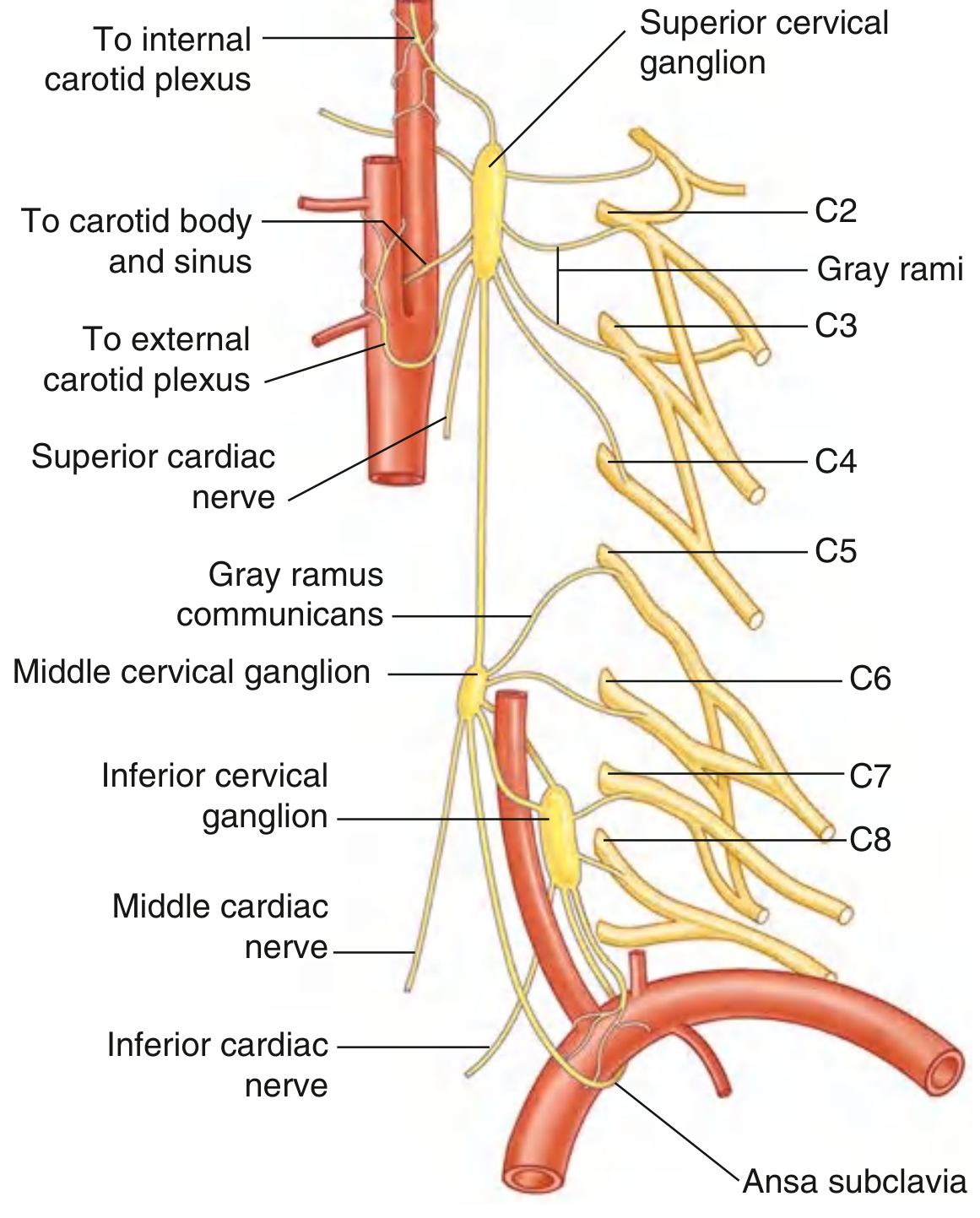
1. Cervical Sympathetic Trunk
- No white rami here (no direct preganglionic input from the cord at cervical levels)
- Receives ascending preganglionic fibers from upper thoracic cord (T1-T3)
- Has 3 ganglia:
| Ganglion | Level | Branches / Supplies |
|---|---|---|
| Superior cervical ganglion | C1-C2 (largest ganglion in the trunk) | Internal/external carotid plexuses, gray rami to C1-C4, pharynx, superior cardiac nerve |
| Middle cervical ganglion | C6 (may be absent) | Gray rami to C5-C6, middle cardiac nerve, thyroid |
| Inferior cervical ganglion | C7 (usually fuses with T1 → stellate/cervicothoracic ganglion) | Gray rami to C7-T1, vertebral artery plexus, inferior cardiac nerve, subclavian loop (ansa subclavia) |
The stellate ganglion (cervicothoracic ganglion) is clinically important - blockade here causes Horner's syndrome (ptosis, miosis, anhidrosis, enophthalmos).
2. Thoracic Sympathetic Trunk
- ~12 ganglia (1st thoracic usually fused into stellate ganglion)
- Has both white and gray rami communicantes at each level
- Position: anterior to necks of ribs superiorly, shifting to costovertebral joints in mid-thorax, then anterolateral to vertebral bodies inferiorly
- Key contribution: gives rise to the splanchnic nerves (preganglionic fibers bypass the chain without synapsing here):
| Nerve | Origin | Destination |
|---|---|---|
| Greater splanchnic | T5-T9 | Celiac ganglion |
| Lesser splanchnic | T10-T11 | Superior mesenteric + aorticorenal ganglia |
| Least splanchnic | T12 | Aorticorenal ganglion |
- Also contributes postganglionic fibers to the cardiac plexus, pulmonary plexus, aortic plexus, esophageal plexus
3. Lumbar Sympathetic Trunk
- ~4 ganglia
- Has white rami only from L1-L2 (end of thoracolumbar outflow)
- Gray rami to all lumbar spinal nerves
- Gives lumbar splanchnic nerves → inferior mesenteric ganglion and hypogastric plexus
- Lies on the anterolateral surface of lumbar vertebral bodies, medial to psoas major
4. Sacral Sympathetic Trunk
- ~4-5 ganglia on the anterior surface of the sacrum, medial to the anterior sacral foramina
- No white rami at sacral levels (no preganglionic input directly here)
- Gray rami to all sacral spinal nerves
- Contributes to the hypogastric plexus and innervation of pelvic organs
5. Ganglion Impar (Coccygeal Ganglion)
- Single unpaired ganglion where the two trunks merge in front of the coccyx
- The terminal point of the entire sympathetic chain
Rami Communicantes - Summary
| Ramus | Fiber Type | Direction | Present At |
|---|---|---|---|
| White ramus communicans | Myelinated preganglionic | Spinal nerve → trunk | T1-L2 only |
| Gray ramus communicans | Unmyelinated postganglionic | Trunk → spinal nerve | All levels (C2 to coccyx) |
Four Pathways for Preganglionic Fibers Once in the Trunk
- Synapse in the ganglion at the same level they entered
- Ascend or descend the trunk and synapse in a ganglion at a different level
- Pass through the trunk and exit as splanchnic nerves to synapse in prevertebral ganglia
- Pass through without synapsing to reach the adrenal medulla directly
Clinical Relevance
| Condition | Mechanism |
|---|---|
| Horner's syndrome | Lesion of cervical trunk / superior cervical ganglion (T1 preganglionic or the ganglion itself) → loss of sympathetics to the eye and face |
| Raynaud's phenomenon | Excessive sympathetic vasoconstriction via the chain → sympathectomy (surgical or chemical) at T2-T3 relieves symptoms |
| Hyperhidrosis | Overactive T2-T3 sympathetic trunk to sweat glands → treated by thoracoscopic sympathectomy |
| Stellate ganglion block | Used for pain, arrhythmias, PTSD, and sympathetically-maintained pain syndromes |
Sources: Gray's Anatomy for Students; Neuroanatomy through Clinical Cases (Blumenfeld); Fischer's Mastery of Surgery
This is a shared conversation. Sign in to Orris to start your own chat.