Histoplasma capsulatum in view of Adrenal TB or Adrenal mass
Reading File
Finding Sources
Finding Sources
Searching PubMed
Histoplasma capsulatum adrenal insufficiency
Searching PubMed
adrenal mass tuberculosis histoplasmosis differential diagnosis
Reading File
Reading File
Finding Sources
Reading Article
PMID: 40205654
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
I now have all the information needed for a comprehensive, well-sourced answer. Let me compose it.
Histoplasma capsulatum - Adrenal Involvement: In Context of Adrenal TB and Adrenal Mass
Overview
Both Histoplasma capsulatum and Mycobacterium tuberculosis are leading infectious causes of primary adrenal insufficiency (Addison disease) worldwide. They share a granulomatous mechanism, predominantly affect both adrenal glands, and can present as bilateral adrenal masses - making their clinical and radiological differentiation challenging yet therapeutically critical.
Why the Adrenal Gland?
The adrenal glands have a rich blood supply (three arterial inputs, one venous outflow), high lipid content, and relative immunological privilege - features that make them a preferred sanctuary for both M. tuberculosis (via hematogenous spread) and H. capsulatum (via dissemination from pulmonary primary infection through the reticuloendothelial system). A 2025 retrospective study from Bangkok (PMID: 40205654) confirmed that 91% of patients with either adrenal histoplasmosis or adrenal TB showed bilateral adrenal abnormalities, and all initially unilateral lesions eventually developed contralateral involvement.
Histoplasma capsulatum: Adrenal Pathology in Detail
Mechanism of Adrenal Injury
H. capsulatum var. capsulatum is an intracellular dimorphic fungus. At 37°C (body temperature), it converts to small (2-4 μm) yeast forms that parasitize macrophages and disseminate via the RES. The adrenal cortex is infiltrated, leading to:
- Granuloma formation (epithelioid histiocytes ± giant cells)
- Caseous or coagulative necrosis
- Progressive destruction of functional cortical tissue
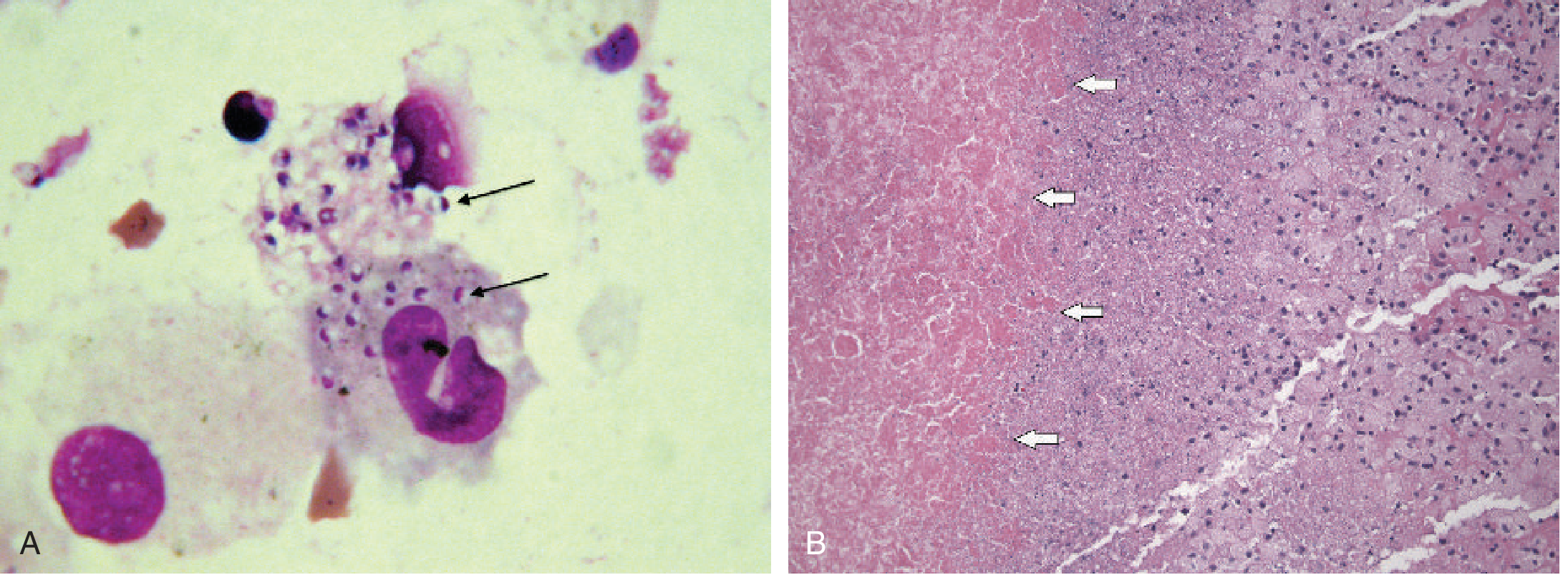
The classical histopathological finding is yeast forms packed within macrophages destroying adrenal parenchyma, with a surrounding area of necrosis. On H&E, yeasts are difficult to see; GMS (Gomori Methenamine Silver) stain is required to identify the small intracellular organisms within necrotic tissue.
Clinical Presentation
- Chronic progressive disseminated histoplasmosis (PDH) is the form that typically involves the adrenal - it can appear months or years after leaving an endemic area
- Symptoms: anorexia, weight loss (91% in the 2025 Bangkok series), fatigue, fever
- Adrenal crisis (acute adrenal insufficiency) occurred in 26% in one series
- Extra-adrenal involvement: oral/pharyngeal ulcers, hepatosplenomegaly, lymphadenopathy
- Adrenal masses may reach up to 9.8 cm in size
- Mostly affects older (mean age ~64), non-HIV males
Histoplasmosis vs. Adrenal TB: Key Comparisons
| Feature | Adrenal Histoplasmosis | Adrenal Tuberculosis |
|---|---|---|
| Mechanism | Hematogenous from primary pulmonary focus via RES/macrophages | Hematogenous from active TB (lungs, GU tract) |
| Bilaterality | ~91% bilateral | ~91% bilateral |
| Adrenal insufficiency | ~73% | ~100% (in small series) |
| Calcification | Less common, late | Common with longer duration (>2 years) |
| Calcification pattern | Rare, dystrophic | Bilateral focal calcification on CT |
| Active extra-adrenal infection | ~45% | ~67% (lung, GU) |
| Coinfection with TB | ~10% | - |
| Endemic zone clue | Ohio/Mississippi river valleys (USA); Central/South America; SE Asia | Developing world, TB-endemic areas |
| AI persistence after treatment | High (all patients with AI remained on steroids at 22 months) | High |
| Tissue biopsy stain | GMS stain for yeast; PAS; H&E often misses | ZN stain for AFB; caseating granulomas |
Sources: Robbins & Kumar Basic Pathology, p. 760; Frameworks for Internal Medicine, p. 4632; Vorasayun et al., 2025 (PMID 40205654)
Adrenal TB: Key Distinguishing Points
From Frameworks for Internal Medicine:
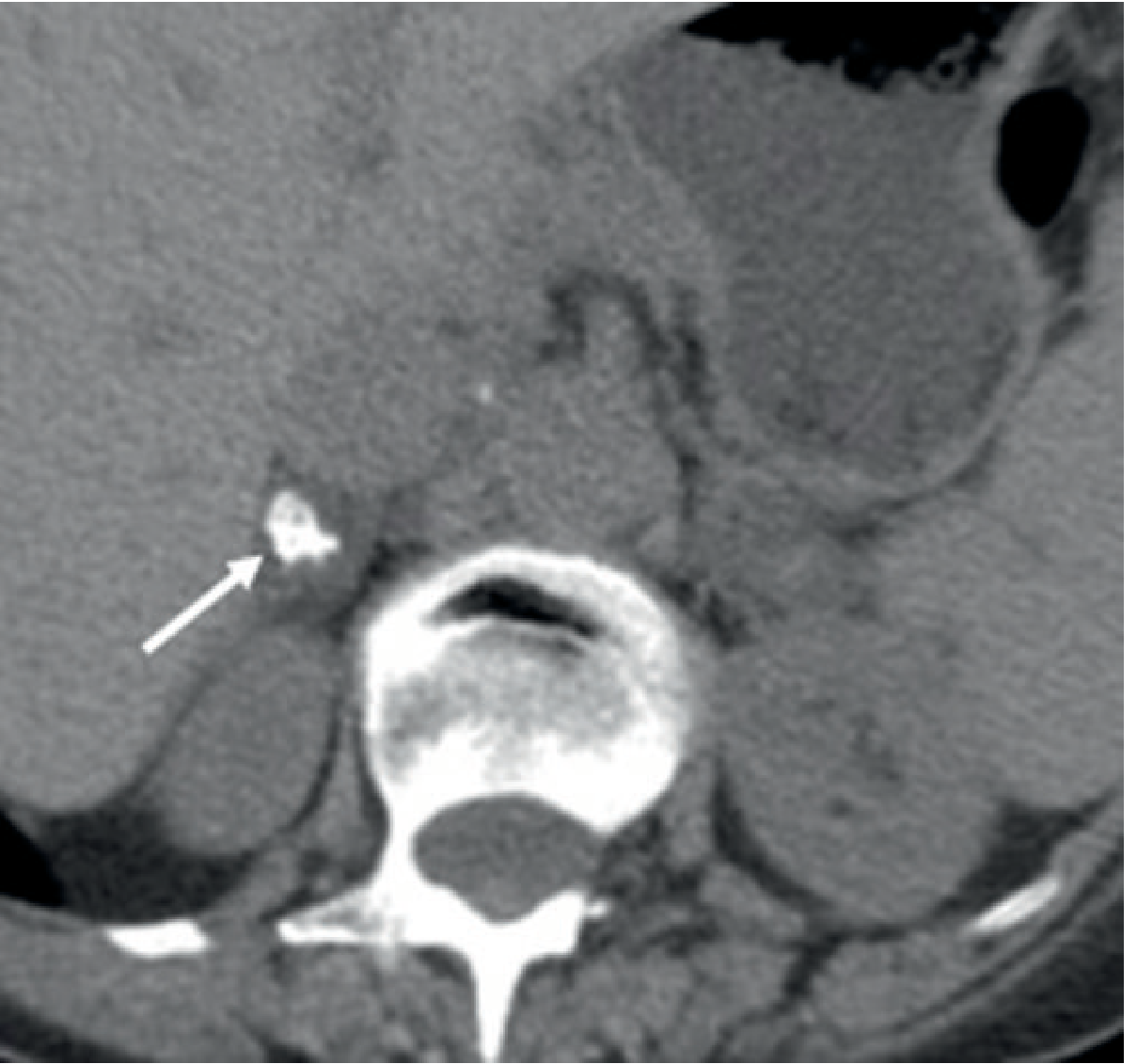
- Early disease (<2 years): bilateral adrenal enlargement, minimal or no calcification
- Late/chronic disease: calcification (can be dense, bilateral) + cortical atrophy
On CT (unenhanced), bilateral adrenal enlargement with focal calcification in the setting of known active TB is virtually diagnostic:
Adrenal Incidentaloma Differential: Where Infection Fits
When a bilateral adrenal mass is found, the differential must include:
- Adenoma (most common single lesion, benign)
- Metastases (breast, lung - account for up to 40% of adrenal incidentalomas)
- Adrenal carcinoma (rare, ~4%)
- Granulomatous infection: TB, histoplasmosis, coccidioidomycosis, blastomycosis, paracoccidioidomycosis
- Lymphoma, sarcoidosis, amyloid, hemorrhage
Clinically, bilateral enlarging adrenal masses + adrenal insufficiency symptoms + granulomatous disease risk factors = infectious etiology until proven otherwise. The key point from the 2025 study is that extra-adrenal infections are present in <50% of histoplasmosis cases - so their absence does NOT rule out adrenal infection, and tissue biopsy remains necessary to distinguish TB from histoplasmosis.
Diagnosis of Adrenal Histoplasmosis
(Harrison's Principles of Internal Medicine, 22nd Ed., Table 239-1)
For progressive disseminated histoplasmosis (which is what adrenal disease represents):
| Test | Utility |
|---|---|
| Histoplasma urine/serum antigen | Most useful; extremely sensitive in PDH; also monitors treatment response |
| Histoplasma serology (ID, CFI, EIA - IgG/IgM) | Useful; may be negative in severe immunosuppression |
| Blood or bone marrow fungal culture | Definitive; slow (weeks) |
| Tissue biopsy (adrenal) | CT-guided; GMS stain shows yeast; culture confirms |
| Blood smear | Occasionally yeasts visible in phagocytes in severe PDH |
For adrenal TB: ZN stain + AFB culture + GeneXpert on biopsy material; tuberculin skin test/IGRA; chest imaging.
Treatment
Adrenal Histoplasmosis (Progressive Disseminated)
- Liposomal Amphotericin B 3-5 mg/kg/day for 1-2 weeks (preferred initial therapy for moderate-severe disease)
- Followed by Itraconazole 200 mg bid (target blood levels 2-5 μg/mL) for at least 12 months
- Monitor urine and serum Histoplasma antigen to gauge treatment response
- In AIDS/immunosuppressed: may need lifelong antifungal maintenance
Adrenal Insufficiency (Both TB and Histoplasmosis)
- Glucocorticoid replacement is mandatory - hydrocortisone 15-20 mg/day (AM) + 5-10 mg (PM), with fludrocortisone if mineralocorticoid deficiency
- Adrenal insufficiency is likely permanent - the 2025 Bangkok study showed all patients with AI remained on glucocorticoid supplements through 22-month follow-up despite specific treatment
- Specific antifungal/anti-TB therapy treats the infection but does not reliably restore cortical function
Adrenal TB
- Standard anti-TB regimen (HRZE for 2 months, then HR for 4-7 months)
- Same permanent AI caveat applies
Key Takeaways
- H. capsulatum and M. tuberculosis are the two dominant infectious causes of bilateral adrenal mass with adrenal insufficiency globally.
- Radiologically, both produce bilateral adrenal enlargement; calcification is more characteristic of TB (especially chronic/healed disease).
- Extra-adrenal infection is absent in >50% of adrenal histoplasmosis cases - do not rely on systemic clues alone.
- Tissue diagnosis (CT-guided biopsy + GMS stain + fungal culture / ZN stain + AFB culture) is required because the treatments are completely different.
- Urine Histoplasma antigen is a rapid, non-invasive first-line test and should be sent in any suspected disseminated histoplasmosis case.
- Adrenal insufficiency in both conditions is usually irreversible and requires lifelong hormonal replacement.
Sources:
- Robbins & Kumar Basic Pathology, Addison Disease section, p. 760
- Robbins, Cotran & Kumar Pathologic Basis of Disease, 10th Ed., Pathogenesis section
- Harrison's Principles of Internal Medicine, 22nd Ed. (2025), Table 239-1 (Histoplasmosis diagnosis/treatment)
- Tietz Textbook of Laboratory Medicine, 7th Ed., Fig. 87.26 (adrenal biopsy histology)
- Grainger & Allison's Diagnostic Radiology, Fig. 37.43 (adrenal TB CT)
- Frameworks for Internal Medicine, Infectious causes of primary adrenal insufficiency, p. 4632
- Vorasayun T et al., "Adrenal Histoplasmosis and Tuberculosis: Clinical Presentations and a High Prevalence of Adrenal Insufficiency," Clin Endocrinol 2025 (PMID: 40205654)
- Jagadish I et al., "Case Report of Disseminated Adrenal Histoplasmosis and Secondary Adrenal Insufficiency," Cureus 2022 (PMID: 36426344)
What are the risk for performing surgery in a case of ischemic stroke
Reading File
Finding Sources
Finding Sources
Searching PubMed
"ischemic stroke" AND "perioperative" AND "surgical risk"
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Loading Image
Reading File
Excellent - I now have comprehensive, well-sourced material. Here is the complete answer.
Risks of Performing Surgery in Ischemic Stroke
Core Problem: Why Surgery is Hazardous After Ischemic Stroke
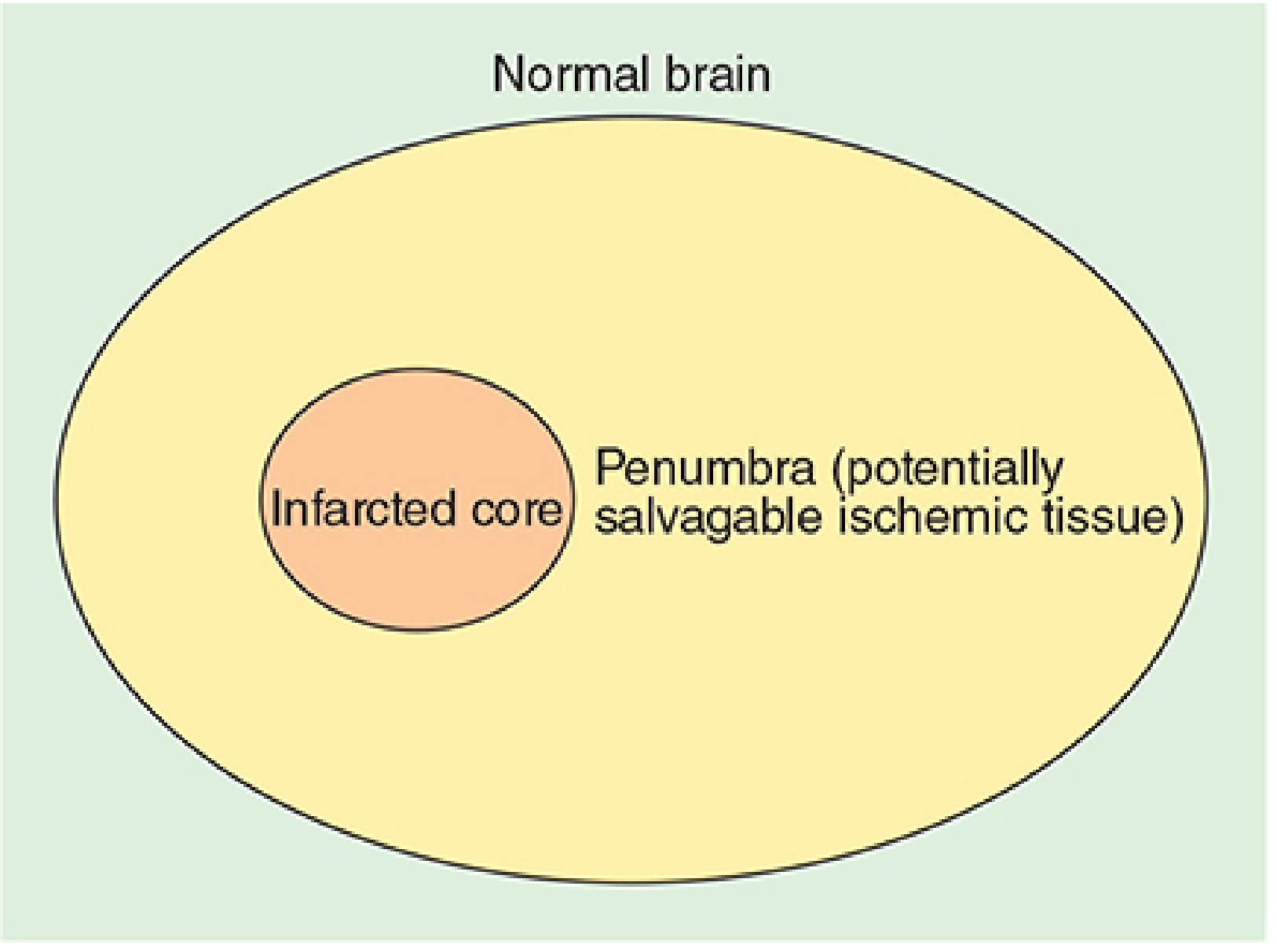
After an ischemic stroke, the brain undergoes a cascade of pathophysiological changes that make it uniquely vulnerable to the stress of surgery and anesthesia. The infarcted core is surrounded by a penumbra of potentially salvageable ischemic tissue - tissue that is alive but fragile, requiring precise perfusion pressure to survive.
1. Loss of Cerebral Autoregulation
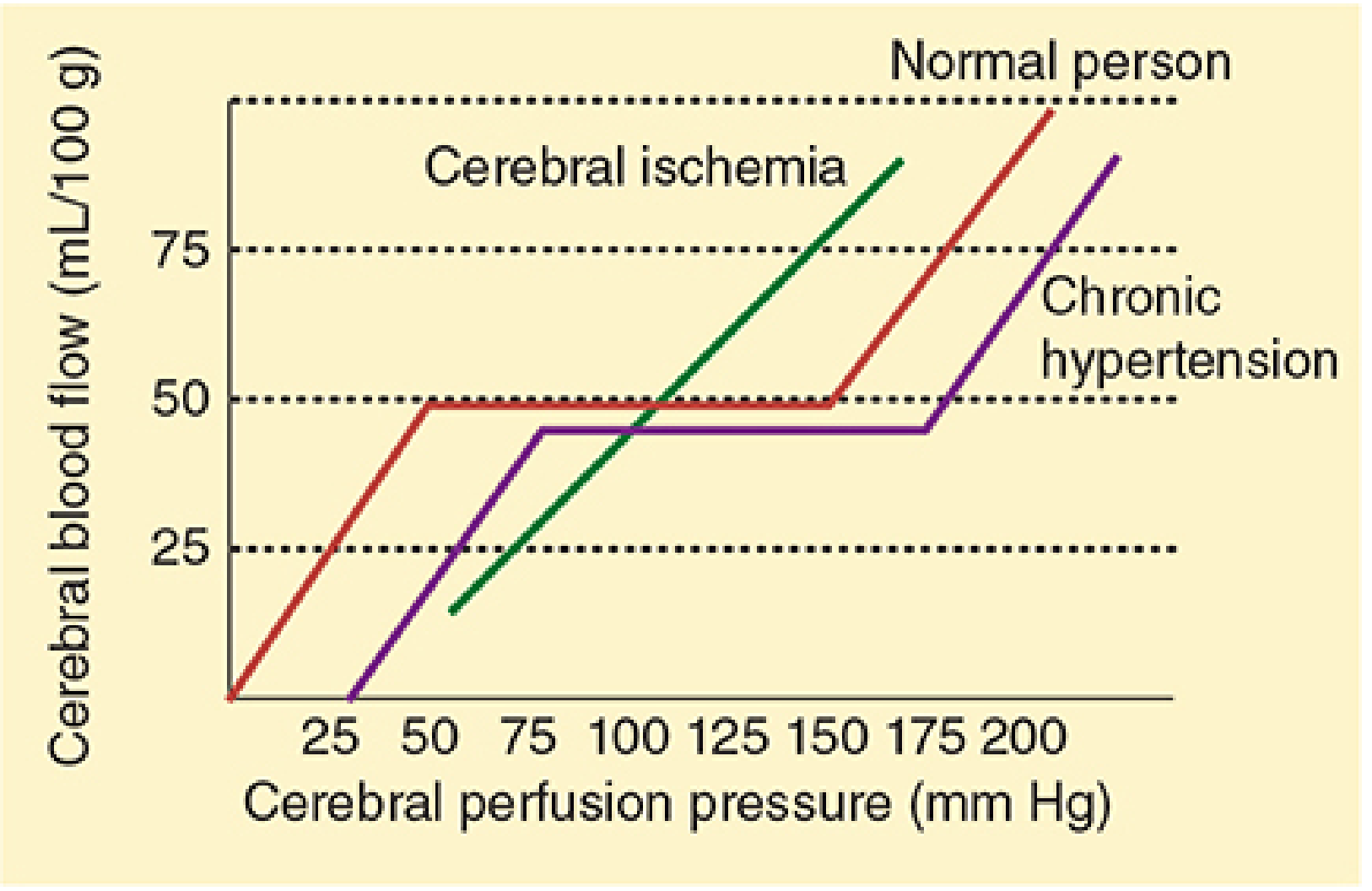
This is the central physiological problem. Under normal conditions, cerebral blood flow (CBF) is kept constant over a wide range of perfusion pressures (mean arterial pressure 50-150 mmHg). After ischemic stroke, autoregulation fails in the ischemic region - cerebral blood flow becomes passively pressure-dependent. This means:
- Hypotension (common during general anesthesia, blood loss, or vasodilators) directly reduces CBF, potentially extending the infarct into the penumbra
- Hypertension (pain response, pressor use) can worsen edema, rupture fragile vessels, and cause hemorrhagic transformation
The timeline of autoregulatory recovery matters:
- Regional blood flow and metabolic abnormalities resolve after ~2 weeks
- CO2 responsiveness and blood-brain barrier may take more than 4 weeks to normalize
2. Risk of Recurrent Stroke
Patients with a prior ischemic stroke are at significantly elevated risk for perioperative recurrent stroke. The risk is highest immediately after the index event:
- The highest risk of another event is within the first month after a stroke (Miller's Anesthesia, 10th Ed.)
- Risk remains significantly elevated for at least 6 weeks for ischemic stroke and 12 weeks for hemorrhagic stroke after procedures such as total hip arthroplasty
- A 4.7-fold increased risk of ischemic stroke was reported in the first 2 weeks after major joint arthroplasty in stroke patients compared with controls
Timing recommendations (AHA/ASA-based guidance):
- The 2021 AHA/ASA scientific statement recommended delaying elective noncardiac surgery for at least 6 months after an acute stroke
- More recent data (cited in Miller's Anesthesia 2024) suggest the incremental risk stabilizes after 90 days, making this a more practical threshold for many patients
- Emergency surgery: If unavoidable within 2 weeks, risk of cardiovascular complications is very high. Paradoxically, if surgery must occur, doing so within 72 hours of stroke may carry lower risk than operating between days 3-14, because cerebral autoregulation deteriorates progressively over the first 5 days before recovering over 3 months
3. Hemorrhagic Transformation of the Infarct
One of the most feared complications. Mechanisms include:
- Reperfusion injury - restoration of blood flow to ischemic tissue causes oxidative damage and BBB breakdown
- Anticoagulant/thrombolytic continuation or initiation perioperatively
- Hypertension breaching the already-damaged blood-brain barrier
Patients who received thrombolytic therapy (tPA) for their stroke are at particularly elevated risk of cerebral hemorrhage if taken to surgery shortly thereafter. Tight blood pressure control is the primary preventive measure.
4. Medication-Related Risks
Most stroke patients are on anticoagulant and/or antiplatelet therapy:
| Medication | Risk if Stopped | Risk if Continued |
|---|---|---|
| Antiplatelet (aspirin, clopidogrel) | Recurrent stroke/TIA, stent thrombosis | Increased surgical bleeding |
| Vitamin K antagonists (warfarin) | Cardioembolic stroke (AF) | Major bleeding |
| DOACs | Cardioembolic stroke | Major bleeding |
| Beta-blockers (new initiation) | Cardiac risk | Significantly increases risk of acute perioperative stroke |
Key points:
- Both VKAs and DOACs should be temporarily discontinued before surgery
- Aspirin may be selectively continued in patients with recent stroke (within 9 months) or high-risk atherosclerotic CVD
- Starting new beta-blockade in a patient awaiting noncardiac surgery significantly increases stroke risk even though it reduces cardiac risk - a critical perioperative tradeoff
- Bridging decisions must weigh thromboembolism risk against bleeding risk on a case-by-case basis
5. Anesthesia-Specific Risks
General Anesthesia
- Hypotension during induction and maintenance is almost universal - especially dangerous given absent autoregulation
- Volatile anesthetics reduce cerebral metabolic rate but also cause vasodilation and may worsen hypotension
- Delayed emergence may mask new neurological deficits
Cardiovascular Surgery (Highest Risk)
Stroke risk is greatest for:
- Cardiac valve surgery (embolic risk from bypass circuit)
- Coronary artery surgery with ascending aortic atherosclerosis (atheromatous debris embolism)
- Thoracic aortic surgery (ischemia from circulatory arrest or clamp near carotid origins)
- 6% of patients experienced adverse neurological outcomes after cardiac surgery in one study
Noncardiac Surgery
- Stroke incidence: 0.08-0.4% after general surgery
- Even in known cerebrovascular disease: 0.4-3.3%
- Pathophysiology: sustained hypotension causing watershed infarctions, thrombosis, or hypertension causing hemorrhagic conversion; perioperative atrial fibrillation causing cardioembolism
6. Systemic Comorbidity Burden
Most ischemic stroke patients carry significant comorbidities that amplify surgical risk:
- Hypertension (already-shifted autoregulatory curve, see Fig. above)
- Diabetes mellitus (poor glycemic control worsens neurological outcomes)
- Coronary artery disease (risk of perioperative MACE - Major Adverse Cardiac Events)
- Renal impairment
- Atrial fibrillation (both a cause of stroke and a perioperative arrhythmia that creates new embolic risk)
- Advanced age (independently increases stroke risk after noncardiac surgery; incidence doubles in patients >75 years)
7. Postoperative Risks Specific to Stroke Patients
| Complication | Mechanism |
|---|---|
| Recurrent ischemic stroke | Hemodynamic instability, AF, hypercoagulable state |
| Hemorrhagic transformation | Reperfusion + anticoagulation |
| Cerebral edema worsening | BBB disruption, fluid shifts, hypertension |
| Postoperative cognitive dysfunction (POCD) | Pre-existing cerebral vulnerability |
| Postoperative delirium | Age, cognitive impairment, systemic stress |
| Aspiration pneumonia | Dysphagia common in stroke patients |
| DVT/PE | Immobility, hemiplegia, hypercoagulable state |
| MACE (MI, cardiac death) | Shared atherosclerotic risk factors |
Summary: Practical Risk Framework
| Time Since Stroke | Elective Surgery | Emergency Surgery |
|---|---|---|
| < 72 hours | Defer unless life-threatening | Proceed with extreme caution; better than 3-14 days window |
| 3-14 days | Highest risk period - defer | Unavoidable only |
| 2-6 weeks | High risk - defer | With intensive neuro-monitoring |
| 6-12 weeks (3 months) | Elevated risk - individualize | Acceptable with precautions |
| > 3 months (90 days) | Risk stabilizes; may proceed if necessary | Lower incremental risk |
| > 6 months | Acceptable for elective (AHA/ASA original guidance) | Standard precautions |
Intraoperative management principles:
- Maintain blood pressure at or above the patient's baseline (avoid hypotension - "tight control")
- Invasive arterial pressure monitoring
- Optimize oxygenation and ventilation (avoid hypocapnia)
- Neurological monitoring (EEG, evoked potentials, near-infrared cerebral oximetry, transcranial Doppler) for high-risk procedures
- Careful anticoagulation management in cooperation with the treating neurologist
Sources:
- Miller's Anesthesia, 10th Ed. - Cerebrovascular Disease section, p. 3993-3994
- Morgan & Mikhail's Clinical Anesthesiology, 7th Ed. - Cerebrovascular Disease (Figs. 28-1 and 28-2), pp. 1147-1149
- Miller's Anesthesia, 10th Ed. - Stroke (Orthopedic/Geriatric surgery), p. 9154
- Barash, Cullen & Stoelting's Clinical Anesthesia, 9th Ed. - Perioperative ischemic evaluation
- AHA/American Stroke Association 2021 Scientific Statement (cited in Miller's, ref. 258)
Why urological surgery is contraindicated in ischemic stroke
Finding Sources
Finding Sources
Searching PubMed
"ischemic stroke" AND "noncardiac surgery" AND "risk" AND "timing"
Finding Sources
Finding Sources
Searching PubMed
"stroke" AND "elective surgery" AND "delay" AND "cerebrovascular"
Reading File
Finding Sources
Reading Article
PMID: 39384506
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
I now have sufficient data for a thorough, accurate answer to this question. Let me synthesize it clearly, including the important clarification.
Urological Surgery and Ischemic Stroke: Risks and Considerations
Important Clarification First
Urological surgery is not uniquely or categorically contraindicated in ischemic stroke in the medical literature. There is no special prohibition that applies only to urology. The contraindication - more accurately described as a relative contraindication to elective surgery - applies to all noncardiac, non-emergency surgery performed within a defined window after ischemic stroke (generally the first 3-6 months).
However, urological procedures carry specific, compounding risks on top of the general surgical risks that make them particularly hazardous in stroke patients. Here is why.
General Surgical Risks After Ischemic Stroke (Applies to All Surgery)
These are established in the previous discussion, but summarized here:
| Risk | Mechanism |
|---|---|
| Recurrent ischemic stroke | Risk highest in first month; persists up to 20+ months |
| Hemorrhagic transformation | Disrupted blood-brain barrier + anticoagulation withdrawal/reinitiation |
| Cerebral hypoperfusion | Autoregulation failure - CBF is pressure-passive |
| MACE (cardiac events) | Shared atherosclerotic substrate |
| Death | Combination of above |
A large NHS England observational study (Luney et al., Br J Anaesth 2025, PMID 39384506) covering 877,430 patients with prior cardiovascular events showed:
- CVA, ACS, and AMI in the year after elective surgery were 2.12 times more frequent after prior cardiovascular events
- The risk of postoperative stroke plateaued only after a 20-month interval from the stroke to surgery
- Risk of cardiac events (ACS/AMI) remained elevated for up to 37 months after a major cardiovascular event
This is considerably longer than the AHA/ASA's 6-month guidance, underscoring the real-world persistence of stroke-related surgical risk.
Why Urological Surgery Specifically Compounds These Risks
1. Patient Demographics - The Overlap Problem
Most urological patients undergoing major procedures (TURP, radical prostatectomy, radical cystectomy, nephrectomy) are:
- Older men (average age 65+ for bladder cancer, older for BPH)
- With comorbid hypertension, atherosclerosis, coronary artery disease
- On long-term antiplatelet or anticoagulant therapy for the same cardiovascular disease that caused their stroke
This is the identical population most at risk for ischemic stroke. The two conditions coexist at high frequency, meaning a stroke patient requiring urological surgery is rarely a healthy baseline patient.
2. Anticoagulation Dilemma - Especially Acute in Urology
Stroke patients are typically on:
- Antiplatelet agents (aspirin, clopidogrel)
- Anticoagulants (warfarin, DOACs) - particularly if stroke was cardioembolic (AF)
Urological procedures carry high bleeding risk from vascular, mucosa-rich fields:
- TURP / TURBT: highly vascular transurethral resection - requires stopping antiplatelets and anticoagulants
- Radical cystectomy: major pelvic surgery with significant blood loss (transfusion frequently needed)
- Nephrectomy: major abdominal/retroperitoneal dissection
Stopping anticoagulation to prevent surgical bleeding directly increases the risk of recurrent cardioembolic stroke. Bridging with heparin adds its own bleeding complications. This is a genuine no-win dilemma that does not resolve easily.
3. TURP / TURBT-Specific Risk: Irrigation Fluid Absorption (TURP Syndrome)
Transurethral resection procedures use hypotonic or isotonic irrigating fluid under pressure. Absorption of large volumes causes:
- Acute hyponatremia (dilutional) and hypoosmolality
- Cerebral edema - in a brain already injured by ischemia and with a compromised blood-brain barrier, even mild cerebral edema can be catastrophic
- Fluid overload, pulmonary edema, cardiovascular decompensation
In a patient with recent ischemic stroke, the already-damaged brain is exquisitely sensitive to osmolar and fluid shifts. TURP syndrome in this context can convert a stable neurological status into acute deterioration.
4. Laparoscopic / Robotic Urological Surgery: Pneumoperitoneum + Trendelenburg
Modern urological surgery (radical prostatectomy, laparoscopic/robotic nephrectomy, cystectomy) is largely performed laparoscopically with steep Trendelenburg positioning. This combination is particularly hazardous post-stroke:
Effects of CO2 pneumoperitoneum + Trendelenburg (from Barash's Clinical Anesthesia, Table 50-5):
| System | Effect |
|---|---|
| CNS | ↑ Intracranial pressure, ↑ Cerebral blood flow |
| Cardiovascular | ↑ SVR, ↓ cardiac output (initial 30% drop), ↑ myocardial O2 consumption |
| Respiratory | ↓ FRC, ↑ peak airway pressure, V/Q mismatch, hypercarbia |
| Endocrine | Activation of renin-angiotensin system |
In a stroke patient:
- Raised ICP from pneumoperitoneum can worsen cerebral ischemia and edema in the infarcted zone
- Hypercarbia from CO2 absorption causes cerebral vasodilation and further ICP rise
- The steep Trendelenburg position (>30°, as used in robotic prostatectomy) is maintained for prolonged periods, with documented cases of upper airway edema, ischemic optic neuropathy, and raised ICP
5. Hypotension During Major Urological Surgery
Radical cystectomy carries 4-6 hours of operative time with significant blood loss. The textbook notes that controlled hypotensive anesthesia (MAP <55-65 mmHg) may be used to reduce bleeding but explicitly states this is associated with increased risk of acute kidney injury and stroke (Morgan & Mikhail's Clinical Anesthesiology, 7th Ed.).
In post-stroke patients, cerebral autoregulation is absent - any drop in MAP directly translates to reduced cerebral perfusion pressure and worsening ischemia in the penumbra.
6. Spinal/Neuraxial Anesthesia Considerations
Many urological procedures (TURP, cystoscopy, orchiectomy) are preferentially performed under spinal anesthesia. While this avoids general anesthetic-related hemodynamic depression, spinal anesthesia causes:
- Sympathetic blockade - acute hypotension (vasodilation below block level)
- Loss of normal baroreceptor compensation in the lower body
In a stroke patient with failed autoregulation, even brief hypotension after spinal induction can compromise the ischemic penumbra.
Summary: Why the Risk Is Considered "Too High" for Elective Urological Surgery
| Factor | How It Impacts Stroke Patient |
|---|---|
| Shared demographics (elderly, hypertensive, atherosclerotic) | Higher baseline recurrent stroke risk |
| Anticoagulation withdrawal (required for surgery) | Exposes patient to cardioembolic/thrombotic recurrence |
| TURP irrigant absorption (TURP syndrome) | Hyponatremia → cerebral edema in injured brain |
| Pneumoperitoneum + Trendelenburg | Raises ICP, worsens cerebral ischemia |
| Controlled hypotension for hemostasis | Direct cerebral hypoperfusion (no autoregulation) |
| Spinal anesthesia hypotension | Same effect on pressure-passive CBF |
| Long operative duration (4-6 hrs for cystectomy) | Prolonged exposure to all of the above |
| Post-op atrial fibrillation | New embolic source; common post-major surgery |
What the Guidelines Say
- AHA/ASA (2021): Delay elective noncardiac surgery for at least 6 months after acute ischemic stroke
- Emerging evidence (Miller's Anesthesia 10th Ed.): Risk stabilizes after 90 days - this may be the more practical threshold
- Luney et al., 2025: Stroke risk plateaus only after ~20 months in real-world data
- Emergency urological surgery (e.g., obstructing urosepsis, ruptured kidney) cannot wait and should proceed with maximal neurological precautions regardless of stroke timing
Bottom Line
Urological surgery after ischemic stroke is not a special category - it falls under the general principle that elective surgery should be deferred after stroke. However, urology is practically among the riskiest domains because it disproportionately involves: (1) elderly men with heavy cardiovascular comorbidity who are the same population that has strokes, (2) procedures requiring anticoagulation cessation, (3) unique physiological hazards such as TURP syndrome, pneumoperitoneum-related ICP rise, and prolonged hypotension that all specifically endanger the post-ischemic brain.
Sources:
- Morgan & Mikhail's Clinical Anesthesiology, 7th Ed. - Urological surgery and Cerebrovascular Disease sections
- Barash, Cullen & Stoelting's Clinical Anesthesia, 9th Ed. - Physiology of Pneumoperitoneum, Table 50-5
- Miller's Anesthesia, 10th Ed. - Cerebrovascular Disease perioperative management
- Luney MS et al., "Adverse outcomes after surgery after a cerebrovascular accident," Br J Anaesth 2025 (PMID 39384506)
This is a shared conversation. Sign in to Orris to start your own chat.