Invasive pulmonary aspergillosis full details for md exams
Reading File
search_medical_text
invasive pulmonary aspergillosis pathogenesis risk factors clinical features diagnosis
search_medical_text
invasive pulmonary aspergillosis treatment antifungal management voriconazole prognosis
search_medical_image
invasive pulmonary aspergillosis CT scan halo sign fungal
GradeResponse
GradeResponse
GradeResponse
Here is a comprehensive, exam-focused review of Invasive Pulmonary Aspergillosis (IPA).
Invasive Pulmonary Aspergillosis (IPA)
1. Etiology & Microbiology
| Feature | Detail |
|---|---|
| Causative organism | Aspergillus fumigatus (most common, ~90%), A. flavus, A. niger, A. terreus, A. nidulans |
| Morphology | Septate hyphae branching at 45° (acute angles) |
| Transmission | Inhalation of ubiquitous airborne conidia (spores) |
| Key property | Thermotolerant (grows at 37–50°C); angioinvasive |
High-yield: A. terreus and A. nidulans are intrinsically resistant to amphotericin B (AmB). A. niger is resistant to itraconazole and isavuconazole.
2. Risk Factors & Pathogenesis
(Harrison's Principles, p. 6263)
Primary Risk Factors
| Risk Factor | Mechanism |
|---|---|
| Profound neutropenia | Primary defense against conidia; risk ↑ with duration |
| High-dose glucocorticoids | Impair macrophage killing; dose-dependent risk |
| Neutrophil/phagocyte dysfunction | Chronic granulomatous disease (CGD), advanced HIV |
| Hematologic malignancy | AML, allogeneic HSCT (especially during engraftment failure) |
| Solid organ transplant | Lung transplant > other organs |
| Underlying structural lung disease | COPD, prior TB cavities, bronchiectasis |
Pathogenesis
- Conidia inhalation → deposition in alveoli
- Normal hosts: alveolar macrophages and neutrophils kill conidia before germination
- In immunocompromised hosts: conidia germinate into hyphae
- Hyphae invade bronchial walls → angioinvasion → vascular thrombosis and infarction
- Hematogenous spread possible → CNS, kidneys, eyes, skin
3. Clinical Features
Symptoms
- Fever unresponsive to broad-spectrum antibiotics (classic presentation in neutropenic patient)
- Pleuritic chest pain (due to infarction)
- Hemoptysis (angioinvasion → vessel erosion)
- Dry cough, dyspnea
- Friction rub on auscultation
- CNS symptoms if disseminated (headache, focal deficits)
Clinical Forms
| Form | Setting | Key Feature |
|---|---|---|
| Angioinvasive | Neutropenic patients | Halo sign on CT, infarction |
| Airway-invasive | Less severe immunosuppression | Bronchopneumonia, tracheobronchitis |
| Chronic necrotizing | Mildly immunosuppressed (COPD, DM) | Indolent, cavity formation |
4. Diagnosis
Imaging
CT Chest is the most important early diagnostic tool in neutropenic patients.
Classic CT Signs:
| Sign | Description | Timing |
|---|---|---|
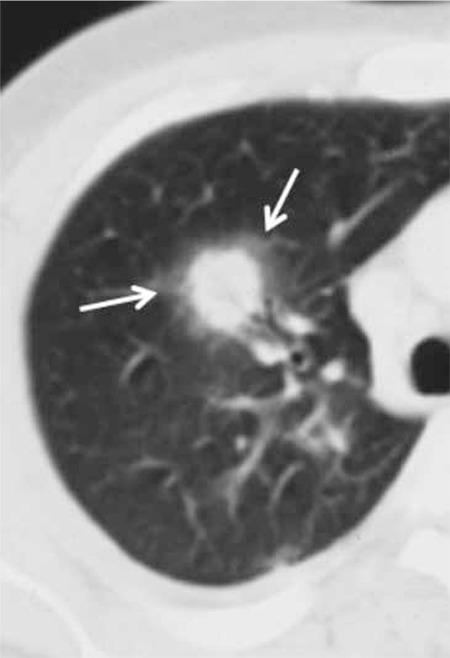
| Halo sign | Nodule/mass surrounded by ground-glass opacity (hemorrhage) | Early (first 10 days) |
| Air-crescent sign | Crescent of air within a cavity | Late (during recovery/neutrophil recovery) |
| Wedge-shaped infarct | Due to vascular occlusion | Variable |
| Consolidation | Segmental/lobar | Any time |
Halo sign = hemorrhage around a central fungal nodule — highly characteristic of angioinvasive aspergillosis in neutropenic patients.
Microbiological Diagnosis
| Test | Sensitivity | Specificity | Notes |
|---|---|---|---|
| BAL / Sputum culture | Moderate | High | Definitive if positive, but slow (24–72h) |
| Serum Galactomannan (GM) | 70–80% | ~90% | Polysaccharide cell wall antigen; useful in HSCT/neutropenic; false positives with piperacillin-tazobactam, mold-active prophylaxis |
| BAL Galactomannan | Higher than serum | High | Preferred in non-neutropenic & SOT |
| Beta-D-glucan (1,3-β-D-glucan) | ~80% | Moderate | Pan-fungal; not specific for Aspergillus |
| Aspergillus PCR | High | High | Increasingly used; ESCMID endorsed |
| Serum LFD (lateral flow device) | ~80% | ~95% | Point-of-care |
| Tissue biopsy | Gold standard | Gold standard | Septate hyphae with 45° branching |
High-yield: Galactomannan is most reliable in neutropenic patients and HSCT recipients. It is less sensitive in solid organ transplant patients on mold-active prophylaxis.
Diagnostic Criteria (EORTC/MSG 2019)
| Category | Criteria |
|---|---|
| Proven | Histopathology/cytopathology showing hyphae + positive culture from normally sterile site |
| Probable | Host factor + clinical feature + mycological evidence (culture/GM/PCR) |
| Possible | Host factor + clinical feature only (no mycological evidence) |
5. Treatment
(Harrison's Principles, p. 6276)
First-Line Therapy
| Drug | Route | Key Points |
|---|---|---|
| Voriconazole | IV/PO | Drug of choice; CYP2C19 polymorphism affects levels; TDM recommended; adverse effects: visual disturbances, hepatotoxicity, phototoxicity |
| Isavuconazole | IV/PO | Non-inferior to voriconazole; fewer drug interactions; preferred in renal impairment |
| Posaconazole | IV/PO | Alternative first-line; excellent prophylactic agent |
Second-Line Therapy
| Drug | Notes |
|---|---|
| Liposomal AmB (L-AmB) | Preferred AmB formulation; less nephrotoxic; first-line alternative when azoles contraindicated |
| Caspofungin | Echinocandin; salvage therapy; active against glucan synthase |
| Micafungin | Salvage; less data than caspofungin |
Combination Therapy
- Voriconazole + anidulafungin: shown in one RCT to improve survival in "probable" IPA — considered in severe or refractory disease
- Routine combination not yet standard practice
Duration
- Minimum 6–12 weeks; in practice 3 months to several years depending on immune status and response
- Continue until lesions resolve/stabilize AND immunosuppression is reversed
Immune Reconstitution
- Immune reconstitution inflammatory syndrome (IRIS) can complicate recovery — paradoxical worsening despite microbiological improvement
- G-CSF to accelerate neutrophil recovery is an important adjunct
6. Prophylaxis
| Setting | Agent |
|---|---|
| AML/MDS induction, HSCT (pre-engraftment) | Posaconazole (drug of choice) |
| Lung transplant | Voriconazole or inhaled AmB |
| High-risk neutropenic patients | Posaconazole oral suspension/tablet |
7. Complications
- Hemoptysis (can be massive and fatal)
- Dissemination: CNS aspergillosis (worst prognosis), endophthalmitis, skin lesions, osteomyelitis
- Cavitation with secondary bacterial superinfection
- Pleural empyema (rare)
- Azole resistance: multi-azole resistance in A. fumigatus is present in <5% of isolates globally but increasing, especially in Southeast Asia (linked to environmental fungicide use)
8. Prognosis
| Factor | Impact |
|---|---|
| Disseminated disease | Mortality >80–90% |
| Neutropenia recovery | Single most important prognostic factor |
| CNS involvement | Near-universal mortality without treatment |
| Early diagnosis + treatment | Significantly improves outcome |
| Allogeneic HSCT | 12-week mortality 40–60% |
| Solid organ transplant | Mortality 50–80% |
An infectious disease consultation is advised for all patients with invasive disease given management complexity (Harrison's p. 6276).
9. High-Yield Exam Summary Table
| Domain | Key Point |
|---|---|
| Most common species | A. fumigatus |
| Morphology | Septate hyphae, 45° branching |
| Strongest risk factor | Profound neutropenia + glucocorticoids |
| Key early CT sign | Halo sign (ground-glass around nodule) |
| Key late CT sign | Air-crescent sign |
| Best serum biomarker | Galactomannan |
| Drug of choice | Voriconazole (or isavuconazole) |
| AmB-resistant species | A. terreus, A. nidulans |
| Best prophylaxis in AML/HSCT | Posaconazole |
| Gold standard diagnosis | Tissue biopsy (histopathology) |
| Prognostic factor #1 | Neutrophil recovery |
10. Differentials (in Immunocompromised + Pulmonary Nodules)
| Condition | Differentiating Feature |
|---|---|
| Mucormycosis | Broader hyphae (>90° branching), ribbon-like, non-septate; more rhinosinusal; halo sign less typical |
| Pulmonary candidiasis | Rare primary pulmonary disease; usually hematogenous |
| Pneumocystis jirovecii (PCP) | Bilateral ground-glass; no nodules; CD4 <200 |
| Bacterial pneumonia | Culture positive; different epidemiology |
| Pulmonary TB | Upper lobe cavities; AFB smear/culture |
| Lung malignancy | Slower growth; biopsy for differentiation |
References:
- Harrison's Principles of Internal Medicine, 21st Edition, pp. 6263, 6276
- EORTC/MSG Revised Definitions of Invasive Fungal Disease (2019)
- IDSA Aspergillosis Guidelines (2016, updated)
This is a shared conversation. Sign in to Orris to start your own chat.