I now have comprehensive, rich content from all key sources. Let me compile the complete guide.
Disseminated Intravascular Coagulation (DIC): Complete Guide for Emergency Physicians
Sources: Harrison's Principles of Internal Medicine 22E (2025), Tintinalli's Emergency Medicine, Rosen's Emergency Medicine, ISTH 2025 Updated Criteria, Japan 2024 Clinical Practice Guidelines
1. DEFINITION
Classic (ISTH 2001): An acquired syndrome characterized by intravascular activation of coagulation with loss of localization, arising from different causes, that can originate from and cause damage to the microvasculature, which if sufficiently severe, can produce organ dysfunction.
Updated ISTH 2025 Definition: "An acquired, life-threatening intravascular disorder characterized by systemic coagulation activation, dysregulated fibrinolysis, and endothelial injury, resulting in microthrombosis. DIC arises from various underlying etiologies and progresses from a potentially asymptomatic early phase to an advanced phase with hemorrhage and/or organ dysfunction."
Key innovations in the 2025 update:
- Phase-based classification: Pre-DIC → Early-phase DIC (subclinical/compensated) → Overt DIC
- Phenotypic classification: Thrombotic DIC (microvascular thrombosis + organ failure) vs. Hemorrhagic DIC (factor consumption + bleeding)
- Sepsis-Induced Coagulopathy (SIC) score now recognized as an early-phase detection tool
- Revised D-dimer thresholds (see scoring below)
2. PATHOPHYSIOLOGY
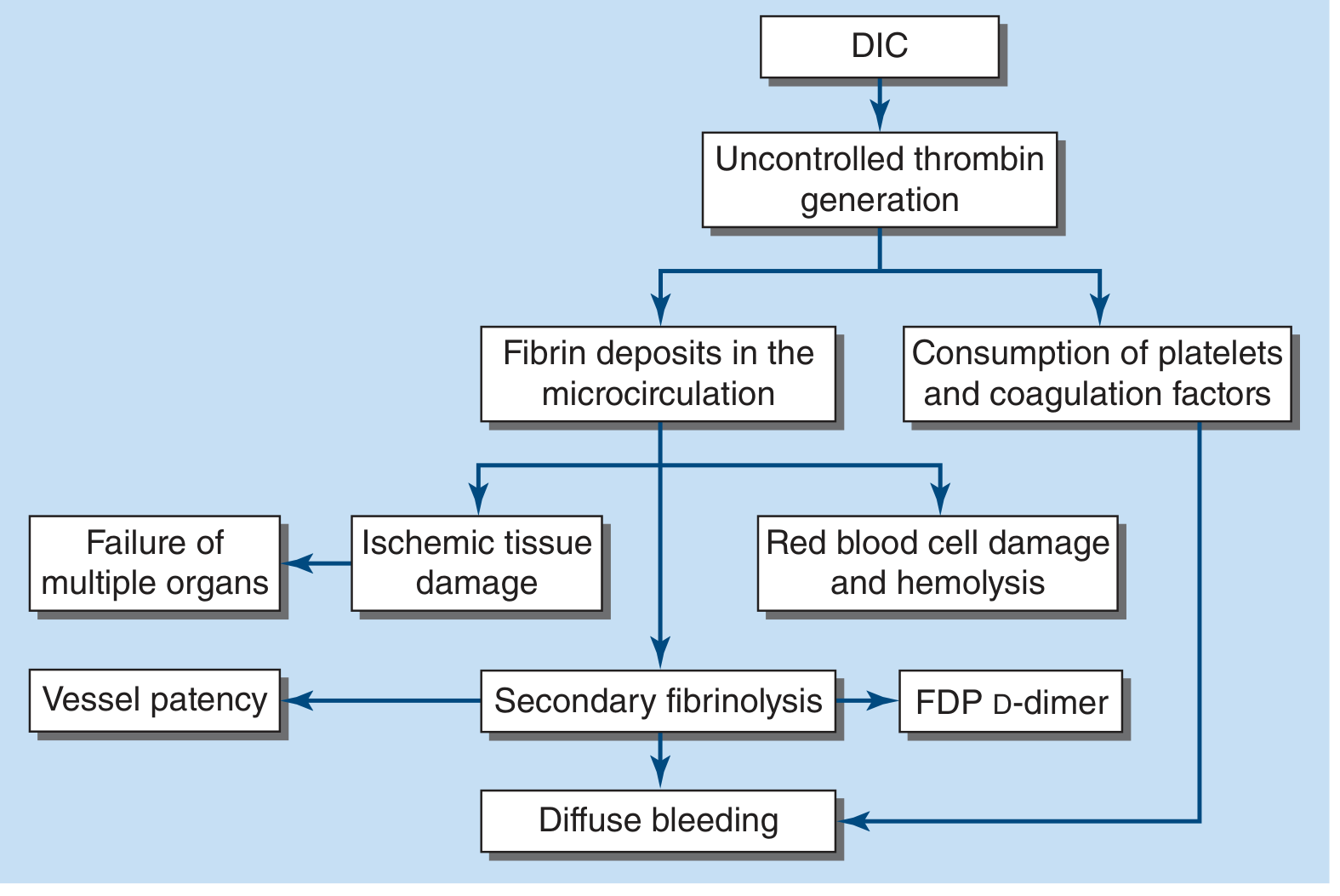
The central driver is uncontrolled thrombin generation, with simultaneous disruption of physiologic anticoagulant mechanisms and abnormal fibrinolysis.
Pathophysiology of DIC: Uncontrolled thrombin generation leads to fibrin deposits in the microcirculation and consumption of platelets/coagulation factors, resulting in ischemic organ failure and diffuse bleeding via secondary fibrinolysis (FDP/D-dimer). - Harrison's 22E, Fig. 121-4
Step-by-step cascade (Rosen's):
- Platelets and coagulation factors are consumed (especially fibrinogen, factors V, VIII, XIII)
- Thrombin is formed - overwhelms its inhibitor system, directly activates fibrinogen
- Fibrin is deposited in small vessels of multiple organs
- Plasmin lyses fibrin and impairs thrombin formation (secondary fibrinolysis)
- Fibrin degradation products (FDPs) are released - impair platelet function and inhibit fibrin polymerization
- Coagulation inhibitors (antithrombin III, protein C, TFPI) are depleted
Thrombo-inflammation (Harrison's 22E): In sepsis, activation of inflammatory pathways increases tissue factor expression, activates neutrophils/monocytes with cytokine release, generates neutrophil extracellular traps (NETs), and releases polyphosphates that engage the coagulation system. Endothelial damage strips native antithrombotic properties.
Purpura fulminans is a severe DIC variant - extensive skin thrombosis, predominantly in young children post-viral/bacterial infection, associated with protein C pathway deficiencies.
3. CAUSES / PRECIPITANTS
| Category | Specific Causes / Key Notes |
|---|
| Infection (most common) | Gram-negative sepsis (10-20% develop DIC); endotoxins stimulate TF expression on monocytes/endothelium. Rocky Mountain spotted fever causes direct endothelial damage. More likely thrombosis than bleeding in sepsis. Asplenic/cirrhotic patients at higher risk |
| Malignancy | Adenocarcinoma (mucin-producing) - tends toward thrombosis (Trousseau's syndrome); AML (esp. APML/M3) - blast cells release procoagulant enzymes, excessive release at cell lysis → bleeding; lymphoma; prostate cancer - tends toward bleeding |
| Trauma | Brain injury, crush injury, burns, hypothermia/hyperthermia, rhabdomyolysis, fat embolism, hypoxia - massive bleeding can occur |
| Obstetric | Placental abruption, amniotic fluid embolism, septic abortion, dead fetus syndrome (chronic DIC), HELLP syndrome |
| Vascular | Large aortic aneurysm (chronic DIC → acute at surgery), giant hemangiomas (Kasabach-Merritt), vasculitis |
| Organ injury | Acute hepatic failure (TF from injured hepatocytes), pancreatitis, ALI/ARDS (20% of ALI develop DIC; 20% of DIC develop ALI) |
| Immunologic | Acute hemolytic transfusion reaction (DIC + severe bleeding + shock + acute renal failure), graft-vs-host disease, transplant rejection |
| Envenomation | Rattlesnakes and vipers - endothelial damage; bleeding not as severe as labs suggest |
| Drugs | Fibrinolytic agents, aprotinin, warfarin (neonates with protein C deficiency), PCCs, amphetamines |
4. CLINICAL PRESENTATION
Acute DIC:
- Petechiae, ecchymoses, purpura
- Bleeding from venipuncture sites - hallmark finding
- Severe hemorrhage: GI tract, lung, CNS
- Microvascular thrombosis → organ dysfunction (renal failure, hepatic failure, CNS changes, ARDS)
- Hemodynamic instability/shock (from underlying disease)
- Mortality 30-80%
Chronic/Compensated DIC:
- Discrete bleeding limited to skin or mucosal surfaces
- Associated with giant hemangioma, metastatic carcinoma, late-gestation fetal demise
- Labs: Elevated FDPs/D-dimer, near-normal PT/aPTT/fibrinogen, mild thrombocytopenia or normal platelet count
Red Flags requiring urgent workup:
- Purpura + bleeding tendency + signs of organ injury (CNS, kidney)
- Oozing from IV sites after sepsis, trauma, obstetric complication, or malignancy
- Thrombosis in unusual locations + concurrent bleeding
5. LABORATORY DIAGNOSIS
Core Labs (order all simultaneously)
| Test | Finding | Pathophysiology |
|---|
| Platelet count | Usually low (<100,000/mm³), or dropping trend | Consumed in clotting |
| PT | Prolonged | Factors II, V, VII, X consumed (factor VII has shortest half-life - falls first) |
| aPTT | Usually prolonged | Factors II, V, VIII consumed |
| Thrombin time | Prolonged | Factor II consumed + decreased fibrinogen + in vivo fibrinolysis |
| Fibrinogen | Low - but may be normal/elevated early (acute-phase reactant!) | Fibrinogen <100 mg/dL = severe DIC |
| D-dimer / FDPs | Elevated (sensitive but not specific) | Secondary fibrinolysis; D-dimer markedly elevated in DIC vs. normal/minimal in liver disease |
| Peripheral smear | Schistocytes, RBC fragments, low platelets | RBC fragmentation on fibrin strands (not always present) |
| Creatinine/UA | May be abnormal | Renal microvascular fibrin deposition |
| Factor assays | Extrinsic pathway most affected: factors VII (falls first), X, V, II low; Factor VIII variable (acute-phase reactant) | - |
Key clinical pearl: In critically ill patients, labs must be repeated every 6-8 hours as patients can rapidly deteriorate. The trend matters more than a single value.
Fibrinogen is tricky: As an acute-phase reactant, it may start elevated. Normal fibrinogen does NOT rule out DIC. Only a frankly low fibrinogen (<100 mg/dL) is diagnostic weight.
6. DIAGNOSTIC SCORING
ISTH Overt DIC Score (Updated 2025)
Only apply when an underlying condition known to cause DIC is present
| Parameter | Value | Points |
|---|
| Platelet count | ≥100 × 10⁹/L | 0 |
| 50-<100 × 10⁹/L | 1 |
| <50 × 10⁹/L | 2 |
| D-Dimer | >7× upper normal limit | 3 |
| >3× upper normal limit | 2 |
| Normal | 0 |
| PT prolongation | ≥6 seconds | 2 |
| ≥3s - <6s | 1 |
| <3s | 0 |
| Fibrinogen (Clauss) | <100 mg/dL (<1 g/L) | 1 |
| >100 mg/dL (>1 g/L) | 0 |
Score ≥5 = Overt DIC (repeat labs daily)
Score <5 = Low-grade/Non-overt DIC (repeat every 1-2 days)
Maximum score = 8 points
Not to be used in pregnant patients
2025 Update: D-dimer thresholds revised - >3× UNL = 2 points, >7× UNL = 3 points (previously used "moderate/severe increase" without numerical anchors). This makes scoring institution-independent when UNL is known.
Sepsis-Induced Coagulopathy (SIC) Score - Early-phase DIC detection
| Parameter | Value | Points |
|---|
| PT-INR | 1.2-1.4 | 1 |
| >1.4 | 2 |
| Platelet count | 100-150 × 10⁹/L | 1 |
| <100 × 10⁹/L | 2 |
| SOFA score | ≥2 | 2 |
SIC Score ≥4 = Significant (associated with increased mortality and progression to overt DIC)
7. DIFFERENTIAL DIAGNOSIS
| Condition | Key Differentiating Features |
|---|
| Severe liver disease | Jaundice + splenomegaly clinically; lab abnormalities are stable (not rapidly worsening); D-dimer minimally elevated; no schistocytes |
| Primary fibrinolysis | Rare; plasmin generated without thrombin; platelets, factor V, and factor VIII preserved in low-normal range; D-dimer minimal/normal |
| TTP/HUS | Thrombocytopenia + microangiopathic hemolytic anemia + multiorgan failure; but ADAMTS13 inhibitor present; PT/aPTT typically normal; fibrinogen normal |
| Heparin-induced thrombocytopenia (HIT) | Paradoxical thrombosis; 4Ts score; positive anti-PF4 antibody |
| ITP | Isolated thrombocytopenia; no coagulopathy; normal PT/aPTT/fibrinogen/D-dimer |
Critical differentiating point: In DIC, labs deteriorate rapidly. In liver disease, they are relatively stable. The dynamic change is the key feature.
8. MANAGEMENT
Overarching Principle
DIC is always secondary. The #1 priority is identifying and treating the underlying cause. Many cases of DIC are self-limited (transfusion reaction) or compensated (tumor-associated) and require only supportive care.
Step-by-Step Emergency Approach
Step 1: Treat the precipitating cause
- Sepsis: antibiotics, source control, fluid resuscitation, vasopressors per Surviving Sepsis Campaign
- Obstetric emergency: delivery of fetus/placenta
- Trauma: damage control resuscitation, hemorrhage control
- APML: initiate ATRA (all-trans retinoic acid) + arsenic trioxide urgently
- Acute hemolytic transfusion reaction: stop transfusion immediately
Step 2: Decide if specific DIC management is needed
Specific management is warranted if the patient has:
- Active bleeding
- Significant bleeding risk requiring an invasive procedure
- Arterial or venous thromboembolism
- Skin necrosis or acral ischemia
Asymptomatic DIC or mildly abnormal labs alone do NOT require blood products.
Blood Product Replacement (Hemorrhagic DIC)
| Product | Indication | Dose | Target |
|---|
| Platelets | Active bleeding + platelets <50,000/mm³ OR high-risk (chemotherapy) + platelets <20,000-30,000/mm³ | Standard dose | >50,000 if bleeding |
| Fresh Frozen Plasma (FFP) | Bleeding + PT/aPTT >1.5× normal OR fibrinogen <100 mg/dL (<1 g/L) | 15 mL/kg (some evidence 30 mL/kg superior when volume overload not a concern) | PT prolonged ≤3s above UNL |
| Cryoprecipitate | Low fibrinogen + active bleeding; volume-restricted patients | Per hematology guidance | Fibrinogen >150 mg/dL |
| Fibrinogen concentrate | Alternative to cryo as fibrinogen source | Per hematology guidance | Fibrinogen >150 mg/dL |
| PRBCs | Maintain hemodynamic stability and adequate Hgb | As needed | Hemodynamic stability |
| Vitamin K | Always give (corrects any concurrent vitamin K deficiency) | 10 mg IV/PO | - |
Monitoring response: Slowing of bleeding + decrease in FDPs + rise in platelet count + rise in fibrinogen = improvement. Normalization of clotting times occurs later - less useful for initial monitoring.
Anticoagulation in DIC (Thrombotic DIC)
Heparin is selectively indicated when fibrin deposition and thrombosis predominate:
Use heparin in:
- Purpura fulminans
- Retained nonviable fetus before delivery
- Giant hemangioma (Kasabach-Merritt)
- Acute promyelocytic leukemia (APML)
- Solid tumor-associated chronic DIC
- Dose: Low-dose continuous infusion UFH (5-10 U/kg/h) or LMWH
Do NOT use heparin in:
- Meningococcemia
- Abruptio placentae
- Severe liver disease
- Trauma-related DIC
- General postoperative DIC
Continuous monitoring of clinical response, heparin activity levels, and bleeding status is essential when using anticoagulation.
Advanced/Adjunct Therapies
| Agent | Evidence | Current Recommendation |
|---|
| Antithrombin (AT) concentrate | Japan 2024 Guidelines: GRADE 1B for DIC with sepsis | Recommended in sepsis-DIC (Japan guidelines); variable use in Western practice |
| Recombinant thrombomodulin | Japan 2024 Guidelines: GRADE 1B for DIC with sepsis | Recommended in sepsis-DIC (Japan); not widely available in all countries |
| Antifibrinolytics (TXA, EACA) | Limited evidence; risk of thrombosis | Consider only in primary hyperfibrinolytic state (APML, giant hemangioma) with severe bleeding; use cautiously with concurrent heparin |
| Recombinant factor VIIa | No improved outcome in DIC | Not recommended |
| Activated protein C | No improved outcome in DIC | Not recommended (withdrawn) |
| PCC (4F-PCC) | No demonstrated benefit in DIC | Not indicated for DIC (indicated for warfarin reversal) |
9. SPECIAL CLINICAL SCENARIOS
DIC in Sepsis
- Thrombosis more common than bleeding in early sepsis-DIC
- SIC score useful for early detection
- Antithrombin + recombinant thrombomodulin GRADE 1B (Japan 2024 Guidelines - PMID 39676120)
- Prophylactic LMWH recommended for VTE prevention (not full-dose anticoagulation)
DIC in Trauma
- Massive hemorrhage dominates
- Prioritize damage control resuscitation: 1:1:1 ratio (PRBCs:FFP:platelets) or whole blood
- Cryoprecipitate early to maintain fibrinogen
- Tranexamic acid within 3 hours of injury (CRASH-2 evidence)
- Hypothermia worsens DIC - actively warm patient
DIC in Obstetrics
- Placental abruption, amniotic fluid embolism, HELLP syndrome, septic abortion
- Modified ISTH score (exclude D-dimer, use platelets + fibrinogen + PT vs. lab control) - sensitivity 88%, specificity 96%
- Fibrinogen <200 mg/dL in pregnancy is concerning (normal is higher in pregnancy)
- Definitive treatment = delivery
DIC in APML (M3 Leukemia)
- Bleeding predominates (worst DIC in malignancy)
- Blast cells release procoagulant enzymes; worsens at cell lysis during chemotherapy
- Urgent ATRA + arsenic trioxide - reduces DIC by differentiating blasts
- Platelet transfusion target: >30,000-50,000/mm³
- Consider antifibrinolytics
- Heparin only if clear thrombosis
DIC in Snake Envenomation
- Endothelial damage; interestingly, bleeding is often less severe than labs suggest
- Antivenom is definitive treatment
- Supportive blood product replacement
10. DISPOSITION
- Admit all patients with active DIC or significant unexplained coagulopathy
- ICU-level care for hemodynamically unstable, multi-organ involved, or rapidly deteriorating DIC
- Transfer if hematologic expertise is unavailable (especially for APML)
- Repeat labs every 6-8 hours in critically ill patients
- Early hematology consultation for complex/refractory cases
11. PEARLS FOR THE EMERGENCY PHYSICIAN
- Think DIC in any patient with: Sepsis + bleeding from IV sites + thrombocytopenia + elevated PT/PTT
- The trend beats the single value - repeat labs every 6-8 hours; rapidly worsening labs = DIC until proven otherwise
- Normal fibrinogen does NOT exclude DIC - it's an acute-phase reactant; it may start high and fall
- D-dimer markedly elevated in DIC vs. only mildly elevated in liver disease or primary fibrinolysis
- Don't transfuse for lab values alone - only transfuse for active bleeding or high-risk procedures
- Heparin is harmful in trauma/abruption - only use when thrombosis dominates
- APML is the one malignancy requiring emergent hematology - ATRA can be life-saving before DIC worsens
- Obstetric DIC = delivery is the treatment - support coagulation until the uterus is emptied
- TTP/HUS mimics DIC but PT/aPTT are typically normal in TTP - check ADAMTS13
- 2025 ISTH update: DIC now has early/pre-clinical phase detection - SIC score ≥4 in sepsis patients warrants close monitoring even before overt DIC criteria are met
12. EPIDEMIOLOGY & PROGNOSIS (ISTH 2025 Meta-analysis)
From the
2025 ISTH SSC systematic review and meta-analysis (PMID 40383152,
J Thromb Haemost 2025):
| Underlying Disease | Pooled Raw Mortality | Odds Ratio for Mortality vs. No DIC |
|---|
| Sepsis | 42% | 3.15× |
| Trauma | 36% | 4.80× |
| Leukemia | 28% | - |
| Heat stroke | 32% | - |
| Snakebite | 8% | - |
Critical finding: No clear yearly trend of improvement in mortality has been observed despite decades of treatment efforts - underscoring the importance of early recognition and treating the underlying cause.
Key References
- Harrison's Principles of Internal Medicine, 22nd Edition (2025), Chapter 121 - Disseminated Intravascular Coagulation
- Tintinalli's Emergency Medicine, 9th Edition, Chapter 233 - Disseminated Intravascular Coagulation
- Rosen's Emergency Medicine, 10th Edition, Chapter 111 - Disseminated Intravascular Coagulation
- Iba T, et al. Updated definition and scoring of DIC in 2025: ISTH SSC communication. J Thromb Haemost. 2025;23(7):2356-62
- Umemura Y, et al. Mortality, diagnosis, and etiology of DIC - systematic review and meta-analysis, ISTH 2025. J Thromb Haemost. 2025 (PMID 40383152)
- Yamakawa K, et al. Japan 2024 DIC Guidelines Part 1: Sepsis (GRADE 1B antithrombin + thrombomodulin). Int J Hematol. 2025 (PMID 39676120)
- Hayakawa M, et al. Japan 2024 DIC Guidelines Part 4: Trauma, burns, obstetrics. Int J Hematol. 2025 (PMID 39890756)