2. H. Pylori positive Gastric Ulcer - treatment regimens precaution 3. Ranitidine - indications, adverse effects precaution 4. Omeprazole in treatment of Zollinger-Ellison Syndrome - pharmacological basis precautions 1. Drugs used in Peptic Ulcer** - classify*, pharmacological basis of use adv effect precaution; Omeprazole* - MOA*, adverse effects precaution uses add diagrams as well answer each toppic in detail 2 mbbs pharmacology refer kdt
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Reading File
Drugs in Peptic Ulcer Disease - 2nd MBBS Pharmacology (KDT Standard)
TOPIC 1: DRUGS USED IN PEPTIC ULCER DISEASE
Pathophysiology - Acid & Defense
Peptic ulcer results from an imbalance between aggressive factors (acid, pepsin, H. pylori, NSAIDs) and defensive factors (mucus, bicarbonate, prostaglandins, mucosal blood flow).
Diagram: Pharmacological Basis of Gastric Acid Regulation
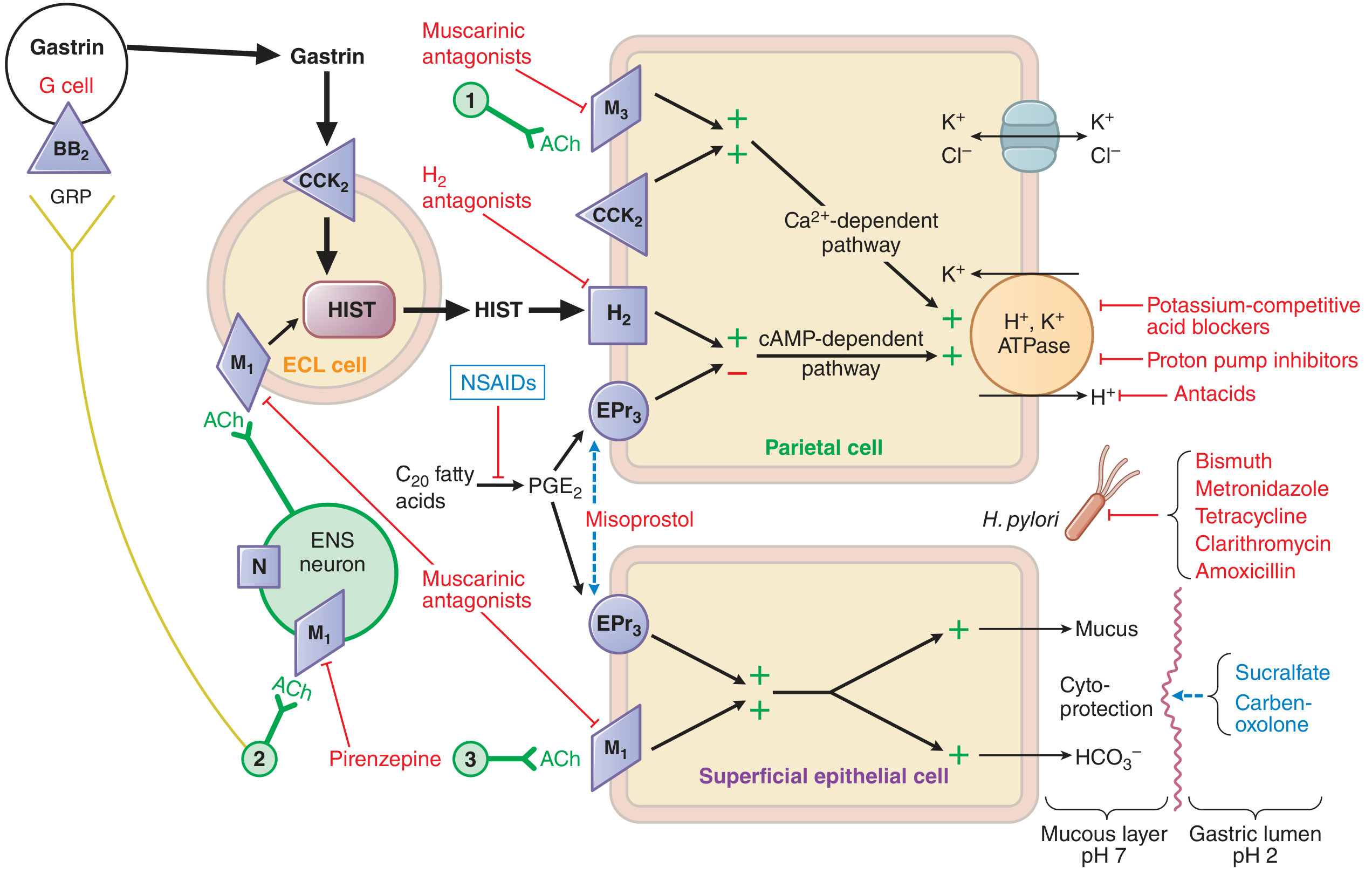
This diagram (from Goodman & Gilman's) shows the ECL cell releasing histamine, G cell releasing gastrin, parietal cell with H+/K+-ATPase, and the sites of action of all anti-ulcer drugs.
Diagram: Parietal Cell - How Drugs Act
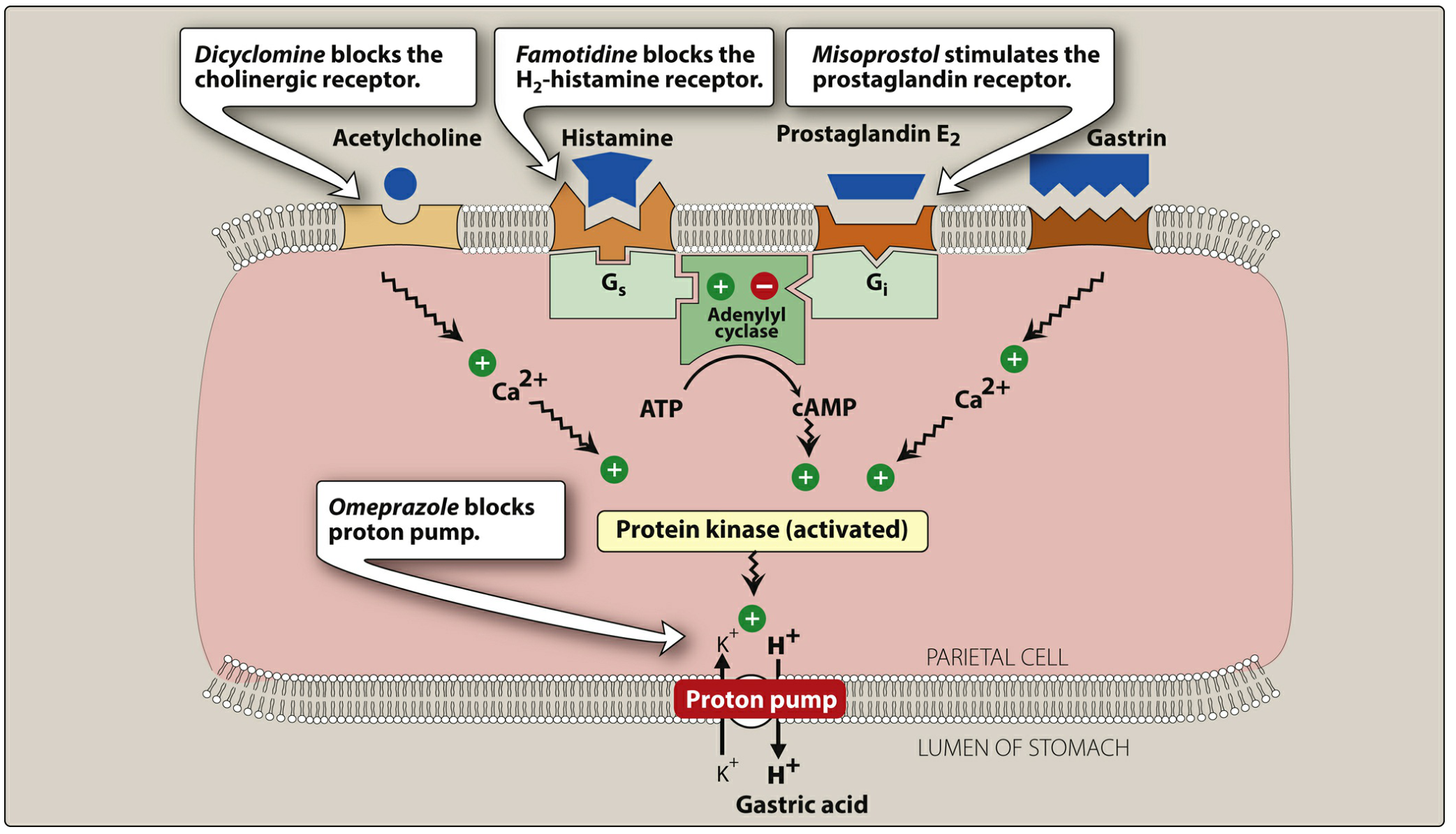
Omeprazole blocks the final proton pump; famotidine/ranitidine block the H2 receptor; misoprostol stimulates the prostaglandin receptor (cytoprotection). Gastric acid secretion is stimulated by acetylcholine (via M3), histamine (via H2, through cAMP), and gastrin (via Ca2+-dependent pathway).
CLASSIFICATION OF DRUGS USED IN PEPTIC ULCER
A. Drugs That Reduce Gastric Acid
1. Antacids (neutralize acid already secreted)
- Aluminum hydroxide, Magnesium hydroxide, Calcium carbonate
- Mechanism: Neutralize HCl → raise gastric pH → inactivate pepsin
- Use: Symptomatic relief, adjunct therapy
- Adverse effects:
- Aluminium - constipation, hypophosphatemia
- Magnesium - diarrhea (so combination "Maalox" balances both)
- Calcium - rebound acid hypersecretion, milk-alkali syndrome
- Precautions: Renal failure (Mg antacids avoided), avoid 2 hours before other drugs (reduces absorption)
2. H2 Receptor Antagonists (antisecretory)
- Cimetidine, Ranitidine*, Famotidine, Nizatidine
- Mechanism: Competitive blockade of H2 receptors on parietal cells → reduces histamine-stimulated acid → reduces basal, nocturnal, and food-stimulated secretion by ~70%
- (Note: Ranitidine was withdrawn from several markets due to NDMA carcinogen contamination; famotidine is now preferred)
3. Proton Pump Inhibitors (PPIs) (most potent antisecretory)
- Omeprazole*, Lansoprazole, Pantoprazole, Rabeprazole, Esomeprazole, Dexlansoprazole
- Mechanism: Irreversible inhibition of H+/K+-ATPase → suppress basal + stimulated acid by >90%
4. Muscarinic Antagonists
- Pirenzepine (M1 selective) - reduces acid secretion via ENS ganglia
- Rarely used now due to atropine-like side effects
B. Drugs That Protect the Mucosa (Cytoprotective)
5. Prostaglandin Analogs
- Misoprostol (PGE1 analog)
- Mechanism: Stimulates EP3 receptor on parietal cells → inhibits acid secretion; stimulates mucus and HCO3- secretion from superficial epithelial cells → cytoprotection
- Use: Prevention of NSAID-induced gastric ulcers
- Adverse effect: Diarrhea (dose-related), uterine contractions
- Contraindication: Pregnancy (causes miscarriage/abortion)
6. Sucralfate
- Mechanism: In acidic pH, polymerizes into a viscous gel that binds to positively charged proteins in ulcer base → forms a protective coating barrier. Also stimulates PG synthesis and binds bile salts.
- Use: Duodenal ulcer, stress ulcer prophylaxis
- Precaution: Take on empty stomach; separate from other drugs by 2 hours (reduces absorption); not effective if gastric pH is raised (avoid combining with antacids/PPIs)
7. Bismuth Compounds
- Bismuth subsalicylate (Pepto-Bismol), Colloidal bismuth subcitrate (CBS)
- Mechanism: Antimicrobial (against H. pylori), inhibits pepsin activity, increases mucus secretion, coats ulcer base
- Use: Component of quadruple therapy for H. pylori; traveler's diarrhea
C. Antibiotics for H. pylori Eradication
- Amoxicillin, Clarithromycin, Metronidazole, Tetracycline (used in combination regimens)
TOPIC 1 (CONTINUED): OMEPRAZOLE - DETAILED
Chemical Nature
Substituted benzimidazole; a weak base (pKa ~4); prodrug.
Mechanism of Action (MOA) - MOST IMPORTANT
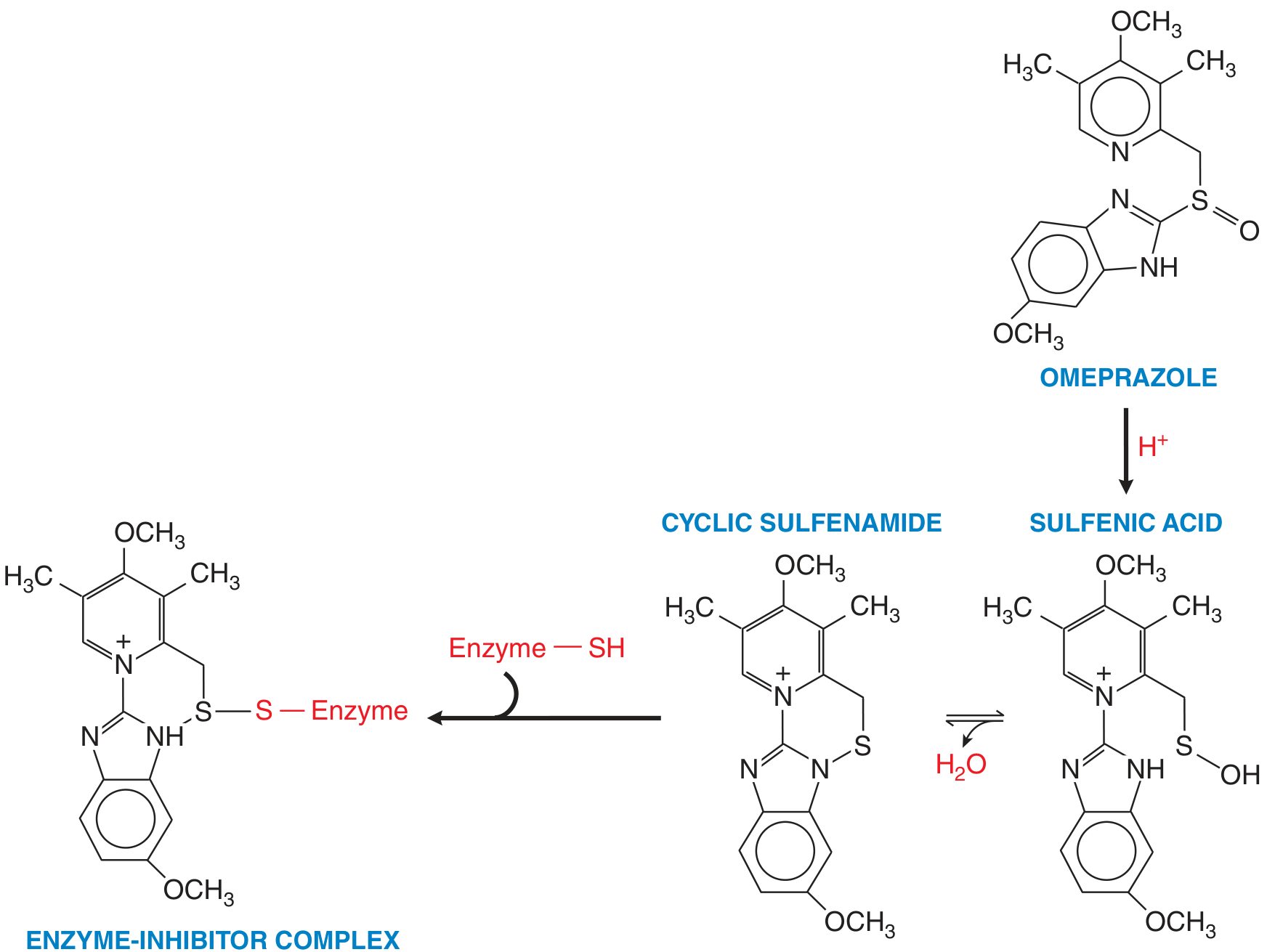
Omeprazole is a PRODRUG. The sequence of activation:
- Oral administration - Enteric-coated capsule (protects from premature degradation in stomach acid)
- Absorbed in the small bowel (alkaline duodenum dissolves enteric coat)
- Transported via bloodstream to parietal cell
- Concentrated in the acidic secretory canaliculus of the parietal cell (acid environment, pH <4)
- Converted to active sulfenamide intermediate (via sulfenic acid)
- Active sulfenamide forms a covalent disulfide bond with the cysteine -SH groups of H+/K+-ATPase
- Irreversible inhibition of the proton pump
- Acid secretion suppresses for 24-48 hours until NEW enzyme is synthesized
Key fact for exams: PPIs are prodrugs; activation requires acid; they bind covalently (irreversibly) to H+/K+-ATPase; should be taken 30-60 min BEFORE meals for maximum effect (food stimulates acid production which activates the drug in the canaliculus).
Effect: Inhibits both basal and stimulated acid secretion by >90% (far superior to H2 blockers at 70%).
Pharmacokinetics:
- Metabolized by hepatic CYP2C19 and CYP3A4
- Asians have higher frequency of "poor metabolizer" CYP2C19 genotype → higher drug levels
- Half-life: 1-2 hours (plasma), but effect lasts 24-48 h (enzyme turnover dependent)
- IV formulation available (omeprazole sodium, pantoprazole IV)
- Dose reduction needed in severe hepatic disease
Therapeutic Uses of Omeprazole
| Indication | Details |
|---|---|
| Peptic ulcer disease (DU + GU) | Drug of choice; heals ulcers faster than H2 blockers |
| GERD / Erosive esophagitis | Drug of choice, especially when H2 blockers fail |
| H. pylori eradication | Combined with antibiotics in triple/quadruple regimens |
| Zollinger-Ellison Syndrome | Drug of choice (see Topic 4 below) |
| NSAID-induced ulcers | Prevention and treatment |
| Stress ulcer prophylaxis | ICU patients |
| Barrett's esophagus | Long-term acid suppression |
Adverse Effects of Omeprazole
| Effect | Mechanism/Notes |
|---|---|
| Headache, nausea, diarrhea, abdominal pain | Most common, mild |
| Hypomagnesemia | Chronic use (>1 year); may cause tetany, arrhythmia |
| Vitamin B12 deficiency | Long-term use; requires acid for B12 absorption from food |
| Iron deficiency | Reduced absorption of non-heme iron |
| Clostridium difficile colitis | Hypochlorhydria allows colonization |
| Community-acquired pneumonia | Loss of gastric acid bactericidal barrier |
| Osteoporosis / Bone fractures | Reduced Ca2+ absorption; long-term use increases hip fracture risk |
| Rebound acid hypersecretion | On stopping chronic therapy; hypergastrinemia |
| Subacute myopathy, interstitial nephritis, skin rashes | Rare |
Drug Interactions (Precautions)
- Clopidogrel: Omeprazole inhibits CYP2C19 → reduced activation of clopidogrel → reduced antiplatelet effect. AVOID combining omeprazole/esomeprazole with clopidogrel. Use pantoprazole instead (least CYP2C19 inhibition).
- Warfarin, Diazepam, Phenytoin: Increased plasma levels due to CYP inhibition
- Atazanavir, Ketoconazole, Itraconazole: Reduced absorption (require acidic pH)
- Methotrexate: Delayed clearance
Precautions
- Take on an empty stomach, 30-60 min before meals
- Not for immediate (rapid) symptom relief - antacids are faster
- Long-term use: monitor Mg2+, B12, bone density
- Reduce dose in severe liver disease
- Do not crush or chew enteric-coated capsules
TOPIC 2: H. PYLORI POSITIVE GASTRIC ULCER - TREATMENT REGIMENS
Why Eradicate H. pylori?
Without eradication: ulcer recurrence rate is 60-100% per year.
With successful eradication: recurrence falls to <15%.
Diagnosis of H. pylori
Diagnostic methods include:
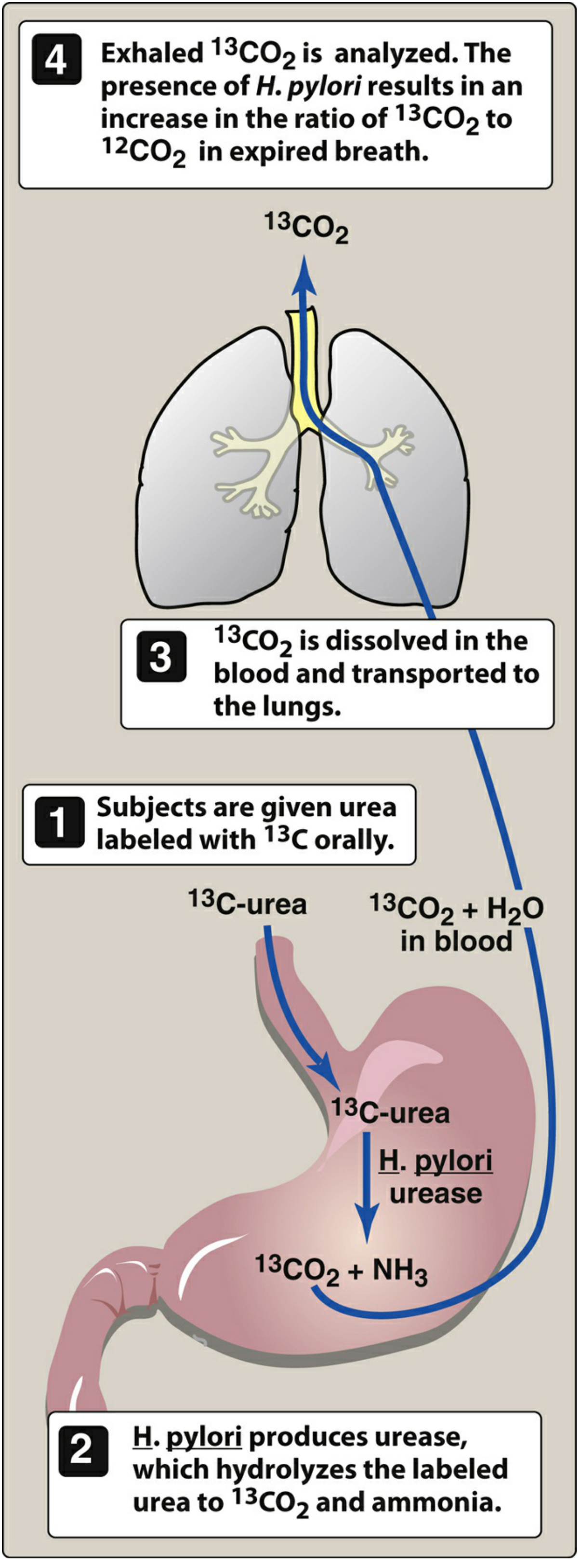
- Non-invasive: Urea breath test (UBT) with ¹³C-labeled urea, fecal antigen test, serology
- Invasive (endoscopy): Rapid urease test, histology, culture
In the UBT: H. pylori urease splits ¹³C-urea → ¹³CO₂ + NH₃. ¹³CO₂ is absorbed into blood, exhaled, and detected by mass spectrometry.
Treatment Regimens
1. Standard Triple Therapy (7-14 days)
PPI + Amoxicillin + Clarithromycin
- Omeprazole 20 mg BD + Amoxicillin 1 g BD + Clarithromycin 500 mg BD
- Preferred when clarithromycin resistance is low (<15%) and no prior macrolide use
- Eradication rate: 70-80% (declining due to resistance)
2. Bismuth Quadruple Therapy - FIRST LINE (10-14 days)
PPI + Bismuth subsalicylate + Metronidazole + Tetracycline
- Omeprazole 20 mg BD + Bismuth 525 mg QDS + Metronidazole 250-500 mg QDS + Tetracycline 500 mg QDS
- Eradication rate: >90% - recommended as preferred first-line in high-resistance areas
- Also used in penicillin-allergic patients
3. Sequential Therapy (10 days)
- Days 1-5: PPI + Amoxicillin
- Days 6-10: PPI + Clarithromycin + Metronidazole/Tinidazole
- Eradication rate: ~90%; evidence suggests superiority over standard triple therapy
4. Concomitant Therapy (5-7 days)
- PPI + Amoxicillin + Clarithromycin + Metronidazole all together
- Good eradication rates in high-resistance settings
5. Levofloxacin-based Rescue Therapy (2nd line)
- PPI + Levofloxacin + Amoxicillin (for failed first-line treatment)
Role of PPI in H. pylori Regimens
- Raises gastric pH → enhances antibiotic stability (amoxicillin is pH sensitive) and efficacy
- Promotes bacteriostatic conditions by raising pH above minimum inhibitory concentration
Precautions in H. pylori Treatment
- Check eradication 4-8 weeks after completing treatment (UBT or fecal antigen test)
- Antibiotic resistance: Clarithromycin resistance is rising globally; in high-resistance areas, use bismuth quadruple therapy
- Compliance: 14-day courses improve eradication rates
- NSAIDs: Avoid during treatment; both H. pylori and NSAIDs cause ulcers
- Penicillin allergy: Replace amoxicillin with metronidazole or tetracycline
- Test-of-cure UBT should be done at least 4 weeks after completing antibiotics and 2 weeks after stopping PPI (to avoid false negatives)
TOPIC 3: RANITIDINE - DETAILED
Note for exam context: Ranitidine was removed from markets (FDA 2020; other regulators followed) due to detection of N-nitrosodimethylamine (NDMA), a potential human carcinogen, in ranitidine products. This was an intrinsic instability issue with the ranitidine molecule itself (not a manufacturing issue). Famotidine is now the preferred H2 blocker. However, ranitidine pharmacology is still relevant for exams as it represents the class.
Pharmacology
- Class: H2 receptor antagonist (2nd generation after cimetidine)
- Structure: Contains a furan ring (unlike cimetidine's imidazole ring)
- Potency: 4-10 times more potent than cimetidine; fewer drug interactions
Mechanism of Action
Competitive, reversible blockade of H2 receptors on the parietal cell basolateral membrane → reduces histamine-mediated stimulation of adenylyl cyclase → reduces cAMP → reduces activation of protein kinase → reduces H+/K+-ATPase activity → reduces gastric acid secretion by approximately 70%.
Acts on:
- Basal acid secretion
- Food-stimulated acid secretion
- Nocturnal acid secretion (most effectively suppressed)
Indications (Therapeutic Uses)
| Indication | Notes |
|---|---|
| Duodenal ulcer | Heals most DUs in 4-8 weeks |
| Gastric ulcer | Heals gastric ulcers; but PPI preferred |
| GERD / Heartburn | Mild-moderate cases |
| Acute stress ulcers | IV infusion in ICU patients |
| Erosive esophagitis | Less effective than PPIs |
| Zollinger-Ellison Syndrome | High doses; PPIs now preferred |
| Pre-anaesthesia | Reduces risk of Mendelson's syndrome (acid aspiration) |
| Pathological hypersecretory states | Mastocytosis, basophilic leukemia |
Adverse Effects of Ranitidine
| Effect | Notes |
|---|---|
| Generally well tolerated | Fewer ADRs than cimetidine |
| Headache, dizziness, diarrhea, constipation | Common but mild |
| CNS: Confusion, altered mentation | Especially in elderly and with IV administration |
| No antiandrogenic effects | (Unlike cimetidine - no gynecomastia, galactorrhea) |
| No significant CYP inhibition | (Unlike cimetidine - fewer drug interactions) |
| NDMA carcinogen issue | Intrinsic molecular instability - reason for market withdrawal |
| Thrombocytopenia | Rare |
| Hepatotoxicity | Rare |
Cimetidine vs. Ranitidine - Key Comparison
| Property | Cimetidine | Ranitidine |
|---|---|---|
| Potency | 1x (reference) | 4-10x more potent |
| CYP450 inhibition | YES (multiple isoenzymes) | Minimal |
| Antiandrogenic effects | YES (gynecomastia, galactorrhea) | No |
| CNS effects | Yes (confusion in elderly) | Less |
| Drug interactions | Many (warfarin, phenytoin) | Fewer |
| Ring structure | Imidazole | Furan |
Pharmacokinetics of Ranitidine
- Oral bioavailability ~50% (first-pass metabolism)
- Widely distributed including CSF, breast milk, placenta
- Excreted mainly by kidneys (renal dose adjustment needed)
- Half-life: ~2-3 hours
Precautions
- Renal impairment: Reduce dose (renally excreted); risk of CNS effects
- Elderly: Risk of confusion with IV administration
- H. pylori-associated ulcers: H2 blockers alone are insufficient - require antibiotic co-therapy; high recurrence without eradication
- NSAID users: PPIs are superior to H2 blockers for both treatment and prevention
- Masking of malignancy: Symptom relief without H. pylori eradication may mask gastric cancer
- Drug interactions with itraconazole/ketoconazole (reduced absorption due to raised pH)
- Can be given IV in acute upper GI bleeding (less effective than high-dose PPI)
TOPIC 4: OMEPRAZOLE IN ZOLLINGER-ELLISON SYNDROME - PHARMACOLOGICAL BASIS & PRECAUTIONS
What is Zollinger-Ellison Syndrome (ZES)?
ZES is caused by a gastrinoma - a gastrin-secreting neuroendocrine tumor (usually in the pancreas or duodenal wall, part of the gastrinoma triangle). Since gastrin is continuously secreted without physiological feedback control, there is massive, continuous stimulation of parietal cells, leading to:
- Extreme hyperacidity (basal acid output >15 mEq/hr; normally <5)
- Multiple, refractory peptic ulcers (often in unusual locations - jejunum, multiple)
- Diarrhea (60-70% of patients) due to acid inactivation of pancreatic enzymes and direct mucosal damage
- Heartburn (20%)
- Elevated fasting serum gastrin levels (>1000 pg/mL diagnostic; normal <100)
Why Omeprazole (PPI) is the Drug of Choice in ZES
Pharmacological Basis:
-
Acts at the final common pathway: The H+/K+-ATPase is the terminal step of acid secretion - it is activated regardless of which stimulus (gastrin, histamine, ACh) drives parietal cells. In ZES, the driver is continuously elevated gastrin. Blocking the final step (proton pump) is more effective than blocking upstream receptors (H2 blockers).
-
Maximal acid suppression (>90%): PPIs suppress both basal and stimulated acid far more than H2 blockers (~70%). In ZES, massive continuous acid output requires this potent suppression.
-
Duration of action: One dose suppresses acid for 24-48 hours (until new enzyme synthesis). This makes management practical.
-
H2 blockers are insufficient in ZES:
- Require very high doses (ranitidine 6-12 g/day was required historically)
- Tolerance (tachyphylaxis) develops with H2 blockers, further reducing efficacy
- These problems are overcome by PPIs
-
Dose of omeprazole in ZES: Higher than standard - typically 60-360 mg/day depending on acid output. Dose is titrated to maintain basal acid output <10 mEq/hr (or <5 mEq/hr if prior esophageal surgery).
-
Long-term use is safe: Prospective studies (Maton et al., Gastroenterology 1989) confirmed safety and efficacy of long-term omeprazole in ZES.
Diagram: Why PPI beats H2 Blockers in ZES
Gastrinoma → Continuous Gastrin ↑↑↑
↓
Gastrin → G-cell → ECL cell → Histamine↑
↓ ↓
Parietal Cell (CCK2R) H2 Receptor
↓ ↓
Ca2+ pathway →→→→→→→→→ cAMP pathway
↓↓↓↓↓↓↓↓↓
H+/K+-ATPase (Proton Pump) ← OMEPRAZOLE blocks HERE
↓
H+ → Lumen
H2 blockers only block the cAMP branch.
Omeprazole blocks the FINAL step = blocks ALL acid regardless of stimulus.
Additional Treatments in ZES
- Surgery: Localization and resection of gastrinoma (curative if single tumor, no mets)
- Somatostatin analogs: Octreotide (suppresses gastrin release, used when surgery not feasible)
- Chemotherapy: For malignant gastrinomas with metastases
Precautions with Omeprazole in ZES
- Higher doses needed - titrate to acid output; dose far exceeds standard 20-40 mg/day
- Long-term monitoring for:
- Hypomagnesemia (may cause tetany, cardiac arrhythmia)
- Vitamin B12 and iron deficiency (monitor annually with long-term use)
- Bone density (long-term PPI - increase hip fracture risk; supplement calcium + Vitamin D)
- Hypergastrinemia (PPIs raise gastrin further by removing acid-negative feedback - but this is secondary and managed as part of the underlying disease)
- ECL cell hyperplasia (from gastrin trophic effects - theoretical concern; not clinically significant at PPI doses used)
- Do not stop abruptly in ZES - rebound acid hypersecretion and risk of ulcer perforation/bleeding
- Drug interactions: Avoid co-prescription of clopidogrel with omeprazole (use pantoprazole instead for antiplatelet patients); monitor warfarin INR
SUMMARY TABLE: Anti-Ulcer Drugs at a Glance
| Drug | MOA | Acid Reduction | Key Use | Key ADR |
|---|---|---|---|---|
| Antacids | Neutralize HCl | Symptomatic | Rapid relief | Constipation (Al), Diarrhea (Mg) |
| Ranitidine (H2 blocker) | H2 receptor competitive block | ~70% | DU, GERD, stress ulcer | CNS (elderly), NDMA concern |
| Cimetidine | Same | ~70% | DU, GU | Gynecomastia, CYP inhibitor |
| Omeprazole (PPI) | Irreversible H+/K+-ATPase inhibition | >90% | DU, GU, GERD, ZES, H. pylori | Hypomagnesemia, B12 deficiency, C. diff |
| Misoprostol | PGE1 analog → cytoprotection + acid reduction | Moderate | NSAID ulcer prevention | Diarrhea, abortion |
| Sucralfate | Mucosal barrier | None | DU, stress ulcer | Constipation, drug chelation |
| Bismuth | Antimicrobial + cytoprotective | None | H. pylori quadruple therapy | Black stools, tongue staining |
Sources: Lippincott Illustrated Reviews: Pharmacology (9781975170561); Goodman & Gilman's The Pharmacological Basis of Therapeutics (9781264258079); Goodman & Gilman covers KDT-equivalent standard for 2nd MBBS pharmacology.
This is a shared conversation. Sign in to Orris to start your own chat.