Difference between median nerve vs c6c7 root involved
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
I now have all the information needed for a comprehensive comparison. Here is the complete breakdown:
Median Nerve Lesion vs. C6/C7 Root Involvement
The key challenge: the median nerve carries C6 and C7 fibers, so symptoms can overlap. The distinguishing features lie in the distribution of weakness, sensory loss, reflexes, and associated findings.
1. Anatomy: Why They Overlap
The median nerve is formed from the lateral cord (C6, C7) and medial cord (C8, T1) of the brachial plexus. So C6 and C7 root pathology will produce deficits in muscles/areas partially served by the median nerve — but the root lesion will additionally affect muscles innervated by other nerves that share those roots.
2. Sensory Distribution
| Feature | Median Nerve (Carpal Tunnel / Wrist) | C6 Root | C7 Root |
|---|---|---|---|
| Area affected | Palmar surface of digits 1–3 and lateral half of digit 4 | Lateral forearm, lateral hand, digits 1 & 2 | Dorsal hand / lateral forearm, digit 3 (also 4) |
| Dorsum of hand | Spared (palmar cutaneous branch and radial nerve cover it) | May be affected | Affected |
| Thenar skin | Affected (but palmar cutaneous branch spared in CTS) | Affected | Spared |
| Medial forearm | Spared | Spared | Spared |
Key point: In carpal tunnel syndrome (CTS), the palmar cutaneous branch arises proximal to the carpal tunnel and supplies the thenar eminence skin — so thenar skin sensation is preserved despite sensory loss in the digits. In C6 radiculopathy, the entire lateral hand including thenar skin is affected.
3. Motor Weakness
| Muscle | Median Nerve Lesion (at wrist/CTS) | C6 Root | C7 Root |
|---|---|---|---|
| Abductor pollicis brevis (APB) | Weak (classic thenar wasting) | Weak (shares C6) | Spared |
| Opponens pollicis | Weak | Weak | Spared |
| Flexor pollicis longus | Weak if proximal lesion; spared in CTS | Weak | Weak |
| Pronator teres | Spared in CTS (branch arises in forearm) | Weak | Weak |
| Flexor carpi radialis | Spared in CTS | Weak | Weak |
| Biceps brachii | Spared | Weak | Spared |
| Brachioradialis | Spared | Weak (major C6 muscle) | Spared |
| Triceps brachii | Spared | Spared | Weak (classic C7) |
| Wrist extensors (ECRL, ECRB) | Spared | Weak (C6) | Weak (C7) |
| Extensor digitorum | Spared | Spared | Weak |
Critical distinguishing muscles:
- Biceps + Brachioradialis weakness → C6 root (not median nerve)
- Triceps + wrist extensor weakness → C7 root (not median nerve)
- Thenar (APB) wasting alone with no proximal weakness → Median nerve / CTS
4. Reflexes
| Reflex | Median Nerve | C6 Root | C7 Root |
|---|---|---|---|
| Biceps reflex (C5–C6) | Normal | Reduced/absent | Normal |
| Brachioradialis reflex (C5–C6) | Normal | Reduced/absent | Normal |
| Triceps reflex (C7–C8) | Normal | Normal | Reduced/absent |
Reflex loss is one of the most reliable distinguishing signs — median nerve lesions do not affect deep tendon reflexes.
5. Pain Distribution
| Median Nerve (CTS) | C6 Root | C7 Root | |
|---|---|---|---|
| Location | Nocturnal wrist/hand pain, digits 1–3 | Lateral arm → dorsal forearm → thumb/index | Posterior arm → dorsal forearm → middle finger |
| Neck pain | Absent | Often present | Often present |
| Scapular pain | Absent | Possible | Subscapular/chest aching (C7) |
6. Additional Distinguishing Features
| Feature | Median Nerve | C6/C7 Root |
|---|---|---|
| Provocative tests | Tinel's sign at wrist, Phalen's test | Spurling's test (neck compression), distraction relief |
| Neck movement pain | Absent | Present |
| Paraspinal muscle tenderness | Absent | May be present |
| Bilateral involvement | Common in CTS | Less common (usually unilateral disc herniation) |
| Associated symptoms | Nocturnal paresthesias, symptom relief with hand shaking ("flick sign") | Radiation from neck, aggravated by Valsalva (cough, sneeze) |
7. Electrodiagnosis (NCS/EMG)
| Median Nerve (CTS) | C6/C7 Radiculopathy | |
|---|---|---|
| Median sensory NCS | Prolonged distal latency or absent across wrist | Normal (root is proximal to DRG in foramina) |
| Median motor NCS | Prolonged distal motor latency | Normal or mildly reduced CMAP amplitude |
| EMG thenar (APB) | Denervation if severe | May show denervation |
| EMG proximal muscles (biceps, brachioradialis, triceps, pronator teres) | Normal | Denervation present |
| Paraspinal muscles | Normal | May show denervation (confirms root level) |
This is the gold standard distinction: In radiculopathy, sensory NCS are normal because the lesion is proximal to the dorsal root ganglion (DRG). In median neuropathy at the wrist, sensory NCS across the wrist are abnormal.
8. Quick Summary Table
| Finding | Median N. (CTS) | C6 Root | C7 Root |
|---|---|---|---|
| Sensory: digits 1–2 | ✓ | ✓ | ✗ |
| Sensory: digit 3 | ✓ | ✗ | ✓ |
| Sensory: dorsum hand | ✗ | ✓ | ✓ |
| Thenar wasting | ✓ | ✓ | ✗ |
| Biceps / BR weakness | ✗ | ✓ | ✗ |
| Triceps weakness | ✗ | ✗ | ✓ |
| Biceps / BR reflex ↓ | ✗ | ✓ | ✗ |
| Triceps reflex ↓ | ✗ | ✗ | ✓ |
| Neck/shoulder pain | ✗ | ✓ | ✓ |
| Tinel's / Phalen's | ✓ | ✗ | ✗ |
| NCS: slow across wrist | ✓ | ✗ | ✗ |
| Paraspinal denervation | ✗ | ✓ | ✓ |
Sources:
- Bradley and Daroff's Neurology in Clinical Practice, Ch. 106 (Entrapment Neuropathies) & Table 31.4
- Localization in Clinical Neurology, 8e, Lesions Affecting C6 & C7
- Harrison's Principles of Internal Medicine 22E, Table 19-1 (Cervical Radiculopathy)
- Neuroanatomy through Clinical Cases, 3e, Three Nerve Roots to Remember in the Arm
Approach to management of status epileptic pt
Finding Sources
Searching the Web
status epilepticus management guidelines 2024 2025
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
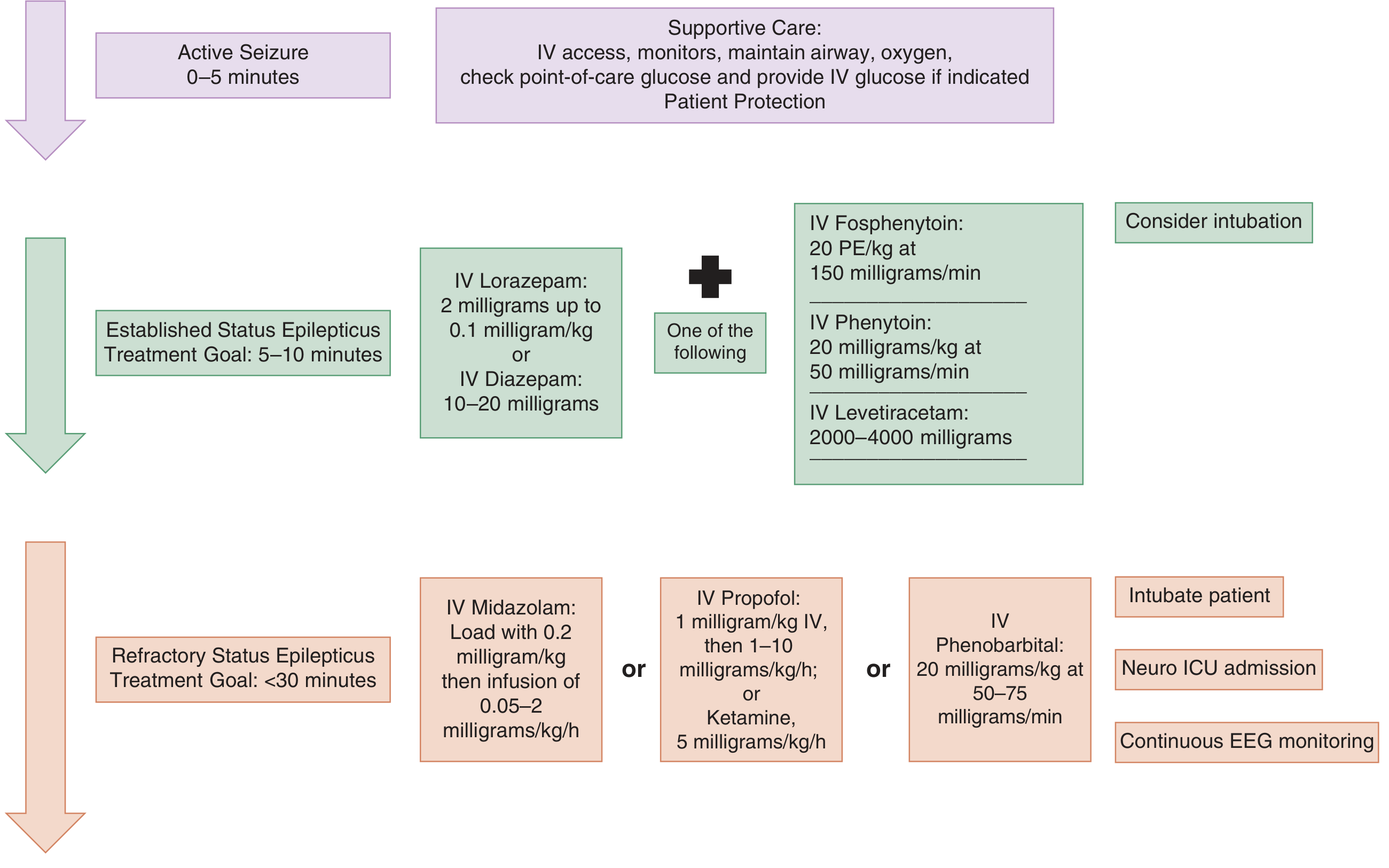
Here is a comprehensive, time-based approach to managing status epilepticus (SE):
Approach to Management of Status Epilepticus
Definition
SE = single seizure ≥5 minutes OR ≥2 seizures without recovery of consciousness between them. After 5 min, seizures are unlikely to self-terminate, increasingly drug-resistant, and begin causing neuronal injury. If sustained >30 min → hypotension, hypoxia, metabolic acidosis, hyperthermia, cardiac dysrhythmias, and pulmonary edema.
Phase 1 — Stabilization (0–5 minutes)
Simultaneous with initial drug therapy:
- Airway: Position patient laterally; suction secretions; give O₂ by mask; prepare for intubation if needed (use short-acting NMB to avoid masking seizure activity)
- Monitoring: Cardiac monitor, pulse oximetry, end-tidal CO₂, continuous BP
- IV/IO access: Large-bore IV; use normal saline (avoid dextrose-containing fluids — incompatible with phenytoin)
- Bedside glucose: Treat hypoglycemia immediately with IV dextrose
- Thiamine: 100 mg IV before glucose if alcoholism or malnutrition suspected
- Temperature: Monitor and actively cool if hyperthermic
Labs to send:
- BMP (Na, Ca, Mg, glucose), renal/liver function
- CBC, lactate
- Anticonvulsant levels (if on AEDs)
- Toxicology screen (urine ± serum)
- Pregnancy test (if applicable)
- Blood cultures if CNS infection suspected
Do NOT do LP during active SE. If meningitis/encephalitis is suspected, start empiric antibiotics/antivirals immediately without waiting.
Phase 2 — First-Line: Benzodiazepines (5–20 minutes)
Benzodiazepines terminate SE in ~70% of cases. Delay >10 min is associated with higher mortality and longer seizure duration.
| Route | Drug | Dose |
|---|---|---|
| IV (preferred) | Lorazepam | 0.1 mg/kg IV (2–4 mg); may repeat once in 5 min |
| IV (alternative) | Diazepam | 5–10 mg IV (0.15–0.2 mg/kg); shorter duration |
| IM (no IV access) | Midazolam | 10 mg IM (0.2 mg/kg); non-inferior to IV lorazepam in trials |
| Intranasal/buccal | Midazolam | 0.3–0.5 mg/kg (max 10 mg) — useful prehospital/pediatric |
| Rectal | Diazepam | 0.2–0.5 mg/kg — prehospital alternative |
Lorazepam is preferred over diazepam when IV access is available — slower onset (3 min vs. 2 min) but far longer duration (12–24 h vs. 15–60 min), fewer seizure recurrences.
Watch for: Respiratory depression and hypotension (especially with alcohol, barbiturates, narcotics).
Phase 3 — Second-Line: Non-Benzodiazepine AEDs (20–40 minutes)
Start a second-line agent simultaneously or immediately after benzodiazepine. One of the following — no strong evidence favors one over another (ESETT trial 2019):
| Drug | Dose | Notes |
|---|---|---|
| Levetiracetam | 60 mg/kg IV (max 4,500 mg) over 10 min | Preferred if liver disease, pregnancy, metabolic disorder. Minimal cardiac/respiratory side effects |
| Fosphenytoin | 20 PE/kg IV at 150 PE/min | Preferred over phenytoin — water-soluble, can give IM, less cardiotoxic, fewer infusion-site reactions |
| Valproate | 40 mg/kg IV (max 3,000 mg) | Contraindicated: liver disease, thrombocytopenia, suspected metabolic disease, pregnancy |
| Phenytoin | 20 mg/kg IV at ≤50 mg/min | Cardiac monitor required; infusion-site necrosis risk; avoid in glucose solutions |
| Lacosamide | 400 mg IV slow bolus | Monitor ECG (prolongs PR interval); good tolerability |
| Phenobarbital | 20 mg/kg IV at 50–75 mg/min | Highly effective but prolonged sedation, respiratory depression, hypotension |
If seizures persist after first second-line agent → try a second second-line agent before declaring refractory.
Phase 4 — Refractory SE (>30–60 minutes despite 2 agents)
Definition: SE continuing after adequate doses of 1 benzodiazepine + 1–2 AEDs.
Mandatory:
- Intubate the patient
- Neuro-ICU admission
- Continuous EEG monitoring (cEEG) — especially after neuromuscular blockade, to monitor for ongoing electrical seizures
Anesthetic infusions — titrate to EEG burst suppression:
| Drug | Loading Dose | Infusion | Notes |
|---|---|---|---|
| Midazolam | 0.2 mg/kg IV | 0.05–2 mg/kg/h | Accumulates in fat; prolonged recovery with renal failure |
| Propofol | 1 mg/kg IV | 1–10 mg/kg/h | Short half-life; rapid neurologic recovery. Risk: propofol infusion syndrome at doses >40 mg/kg/h (metabolic acidosis, rhabdomyolysis, cardiac failure) |
| Phenobarbital | 20 mg/kg IV | — | Third-line; prolonged sedation, hypotension |
| Pentobarbital | Bolus then drip | — | Most effective for burst suppression; most hemodynamic instability |
| Ketamine | 0.5–4.5 mg/kg bolus | Up to 5 mg/kg/h | NMDA antagonist — useful because GABA receptors are internalized in refractory SE; increasingly used |
Current recommendation: Propofol or midazolam as first/second choice in refractory SE; barbiturates (pentobarbital) as third-line.
Phase 5 — Super-Refractory SE (>24 hours despite anesthetic therapy)
Consider (with neurology/epilepsy input):
- Ketamine infusion escalation
- Inhaled anesthetics (isoflurane)
- Immunotherapy (IVIG, steroids, plasmapheresis) if autoimmune encephalitis suspected
- Hypothermia
- Ketogenic diet
- Surgical options (resection, corpus callosotomy) in selected cases
Management Algorithm
Nonconvulsive SE (NCSE)
- Suspect in: prolonged postictal state, fluctuating altered consciousness, subtle twitching/eye deviation, unexplained coma
- Diagnosis by EEG — often missed clinically
- Treatment same as convulsive SE, but less urgency — start at lower doses more cautiously
- Absence SE: treat with benzodiazepine → IV valproate; long-term with ethosuximide or valproate
Identify and Treat the Cause
Always search for and correct the underlying cause in parallel:
| Category | Examples |
|---|---|
| Metabolic | Hypoglycemia, hyponatremia, hypocalcemia, hypomagnesemia, uremia |
| AED non-compliance | Check drug levels |
| CNS infection | Bacterial meningitis, viral encephalitis, abscess |
| Structural | Stroke, hemorrhage, tumor, trauma |
| Toxic | Alcohol withdrawal, cocaine, isoniazid (give pyridoxine), theophylline |
| Autoimmune | Anti-NMDA receptor encephalitis, LGI1, CASPR2 |
| Anoxic/hypoxic | Post-cardiac arrest |
Key Time Targets
| Time | Action |
|---|---|
| 0–5 min | ABC stabilization, glucose check, IV access |
| 5–10 min | Benzodiazepine (1st dose) |
| 10–15 min | Repeat benzodiazepine if seizure continues |
| 20 min | 2nd-line AED started |
| 30–60 min | If refractory → intubate, anesthetic infusion, ICU |
| >60 min | Super-refractory SE — multidisciplinary approach |
Sources:
- Tintinalli's Emergency Medicine, 9e, Ch. 171 (Status Epilepticus)
- Rosen's Emergency Medicine, 9e, Ch. 169
- Katzung's Basic and Clinical Pharmacology, 16e, Ch. 24 (Antiseizure Drugs)
- Surgical Critical Care SE Guidelines 2025
Search for clinical images of SE complications (rhabdomyolysis, propofol syndrome)
Searching Images
rhabdomyolysis urine dark myoglobinuria clinical
Searching Images
propofol infusion syndrome metabolic acidosis ECG
Searching Images
rhabdomyolysis muscle necrosis histology creatine kinase elevation
Searching Images
propofol infusion syndrome green urine lipemia triglyceride
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Here are the clinical images retrieved, organized by complication:
SE Complication Images
Rhabdomyolysis
1. Myoglobinuria — "Coca-Cola" Urine (specimen bottle)
Classic dark reddish-black urine with surface froth (indicating proteinuria/myoglobinuria). This is the hallmark sign of rhabdomyolysis and poses high risk for acute kidney injury via pigment nephropathy.

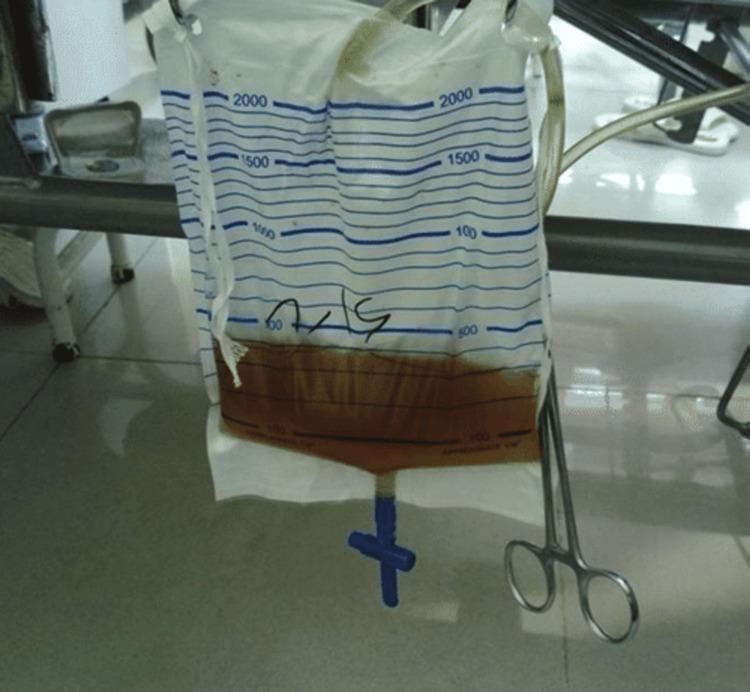
2. Myoglobinuria — Urinary Catheter Bag
Dark brownish-amber urine collected in a catheter drainage bag at the bedside — typical ICU presentation of rhabdomyolysis complicating prolonged SE.
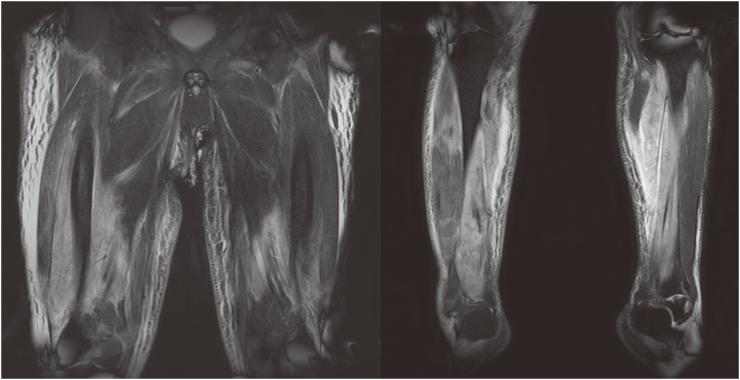
3. MRI — Bilateral Muscle Edema (T2/STIR)
Coronal MRI of lower extremities showing bilateral, patchy, high-signal intensity in multiple muscle compartments of thighs and calves — consistent with extensive intramuscular edema and inflammation in severe rhabdomyolysis. The symmetrical but heterogeneous distribution distinguishes systemic muscle injury (as seen in SE) from localized trauma.
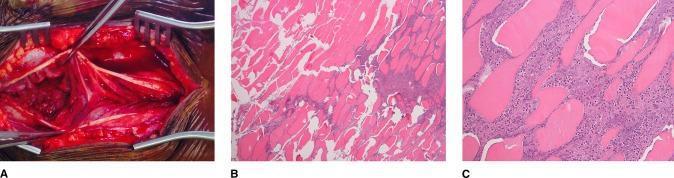
4. Histopathology — Muscle Necrosis (H&E)
- (A) Intraoperative photo showing dusky, gray, devitalized muscle vs. healthy red tissue — ischemia and necrosis
- (B) 40× H&E — hypereosinophilic sarcoplasmic fragmentation, loss of nuclei, interstitial acute inflammatory infiltrate (neutrophils)
- (C) 200× H&E — detailed view of myonecrosis with neutrophilic infiltration and necrotic debris
5. Ultrasound — Right Biceps in Rhabdomyolysis
Point-of-care MSKUS showing:
- ★ (star) — anechoic fluid pockets surrounding muscle bundles
- ▷ (open arrow) — disorganized, heterogeneous muscle fascicles (necrosis)
- ▶ (closed arrow) — hypoechoic regions (edema/inflammation)
- △ (arrowhead) — hyperechoic areas (hypercontracted/injured fibers)
External muscle boundary remains intact, distinguishing this from a tear.

Propofol Infusion Syndrome (PRIS)
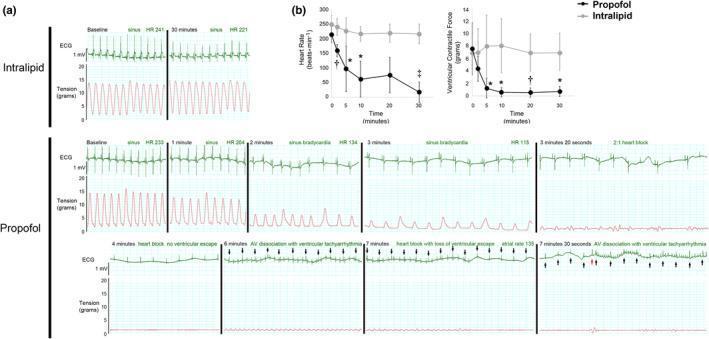
6. PRIS — Cardiac Electrophysiology (Isolated Heart Model)
This experimental panel directly demonstrates the cardiotoxic mechanism of high-dose propofol:
- Intralipid (control): Stable sinus rhythm and ventricular contractile force throughout 30 minutes
- Propofol group — sequential progression:
- Sinus bradycardia (1–3 min)
- 2:1 heart block (3.3 min)
- Complete heart block, no ventricular escape (4 min)
- AV dissociation with ventricular tachyarrhythmia (6–7.5 min)
- Near-total loss of contractile force
Panel (b) quantifies the time-dependent, statistically significant drop in HR and contractility — illustrating why PRIS carries a mortality >30%.
Summary of SE Complications Illustrated
| Complication | Key Image Findings |
|---|---|
| Rhabdomyolysis | Cola-colored urine (myoglobinuria), MRI muscle edema, H&E myonecrosis + neutrophilic infiltrate, MSKUS disorganized fascicles |
| Propofol Infusion Syndrome | Progressive bradycardia → complete heart block → ventricular tachyarrhythmia → cardiac failure on ECG/tension tracings |
Clinical reminder: PRIS risk is highest with propofol doses >40 mg/kg/h sustained >48 h. Monitor for unexplained metabolic acidosis, elevated CK, triglycerides, and new ECG changes (Brugada-like pattern) in any ICU patient on propofol infusion for refractory SE.
Pt kco epilepsy not taken drug for 2 days now presented with status epilepticus now what to do
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
I have all the necessary information. Here is the complete, clinically practical approach for this specific scenario:
Known Epileptic + 2-Day AED Non-Compliance → Status Epilepticus
What Makes This Case Special
- Cause is known → subtherapeutic AED levels (most common precipitant of SE)
- No need to spend time chasing a new structural/metabolic cause initially
- The same AED the patient was on is your best second-line agent — reload it IV
- Prognosis is generally better than SE from acute structural causes
Step-by-Step Management
Phase 1 — Immediate Resuscitation (0–5 min)
| Action | Detail |
|---|---|
| Airway | Position lateral, suction, O₂ by mask; prepare for intubation if needed |
| IV access | Large-bore IV × 2; send bloods immediately |
| Monitor | ECG, SpO₂, end-tidal CO₂, BP every 5 min |
| Glucose | Bedside glucose stat → give 50 mL of 50% dextrose if hypoglycaemic |
| Bloods | Electrolytes, Ca, Mg, glucose, LFTs, RFTs, CBC, lactate, AED drug level, arterial blood gas |
| Toxic screen | Urine toxicology (rule out co-ingestion) |
💡 Key difference in this case: Order the specific AED drug level (e.g., valproate, phenytoin, levetiracetam, carbamazepine) immediately — this confirms the cause and guides reload dose.
Phase 2 — First-Line: Benzodiazepine (5–10 min)
Same as any SE — benzodiazepines FIRST regardless of cause:
| Route | Drug | Dose |
|---|---|---|
| IV | Lorazepam | 0.1 mg/kg (2–4 mg); repeat once after 5 min if seizure continues |
| IM (no IV) | Midazolam | 10 mg IM |
| Intranasal/buccal | Midazolam | 0.2–0.5 mg/kg (max 10 mg) |
Phase 3 — Second-Line: Reload the Patient's OWN AED (within 20 min)
This is the most important nuance in this case. After benzodiazepines, the priority is to rapidly restore therapeutic levels of the patient's existing AED — this treats the cause and prevents recurrence:
If Patient Was on Valproate (VPA)
- IV Valproate: 20–40 mg/kg IV at 3–6 mg/kg/min (max 3,000 mg)
- Also effective for both generalized and partial seizures
- Avoid if: liver disease, thrombocytopenia, pregnancy, suspected metabolic disease
If Patient Was on Phenytoin / Fosphenytoin
- Fosphenytoin (preferred over phenytoin): 20 PE/kg IV at 150 PE/min
- Check drug level before deciding dose; if level is zero/very low → full 20 mg/kg load
- Cardiac monitor mandatory during infusion (bradycardia, hypotension)
If Patient Was on Levetiracetam (LEV)
- IV Levetiracetam: 60 mg/kg IV (max 4,500 mg) over 10 min
- Safest profile — no cardiac effects, no hepatic metabolism, no drug interactions
- Excellent choice if patient was on oral LEV and is non-compliant
If Patient Was on Carbamazepine / Oxcarbazepine
- No IV formulation available → use a different second-line agent (fosphenytoin, VPA, or LEV) acutely
- Restart oral carbamazepine/oxcarbazepine once seizure is controlled and patient can swallow
If Patient Was on Phenobarbital
- IV Phenobarbital: 20 mg/kg IV at 50–75 mg/min
- Longer-acting; significant sedation and respiratory depression — monitor closely
Phase 4 — After Seizure Termination
Once SE is controlled:
Immediate Actions
- Restart the patient's home AED at their usual dose — do not wait
- If subtherapeutic level confirmed → adjust dose (consult neurology)
- Check drug level at 1–2 hours post-loading and again at 24 hours to confirm therapeutic range
- Continue IV AED until oral route is confirmed safe (patient awake, swallowing)
- Transition IV → oral same drug once patient is alert
Monitoring (next 24–48 hours)
- Continuous EEG if altered consciousness persists (rule out subclinical/nonconvulsive SE)
- Monitor for rhabdomyolysis: urine output, urine colour, CK levels, serum creatinine
- Temperature, BP, glucose, electrolytes
- Chest X-ray (aspiration pneumonia)
Phase 5 — Identify and Address Why the Drug Was Stopped
| Reason | Action |
|---|---|
| Forgot / ran out | Counselling, pill organiser, prescription refill |
| Side effects | Reassess drug, consider switch/dose reduction |
| Financial / access | Social work referral, generic options |
| Felt "cured" | Education about lifelong epilepsy management |
| Drug interaction causing subtherapeutic levels | Review all co-medications |
| Intercurrent illness (vomiting, diarrhoea) | Address illness; consider IV/IM bridging |
Phase 6 — Before Discharge
- Neurology review mandatory before discharge
- Confirm AED level is in therapeutic range
- Written counselling: never stop AED abruptly — taper only under medical supervision
- Counsel on driving restrictions (varies by jurisdiction — typically no driving for 3–12 months after SE)
- Rescue medication prescription (buccal/nasal midazolam) for carers
- Seizure diary, follow-up plan
Quick Summary Card for This Scenario
0–5 min: ABC → IV access → glucose → bloods (inc. AED level)
5–10 min: Lorazepam 0.1 mg/kg IV (repeat once)
10–20 min: Reload patient's own AED IV (VPA / fosphenytoin / LEV)
>30 min: Refractory → intubate + anesthetic infusion (midazolam/propofol)
Post-SE: Restart home AED, check levels, counsel on compliance
EEG monitoring, rhabdomyolysis screening, neurology follow-up
Sources: Tintinalli's Emergency Medicine 9e (Ch. 138, 171); Katzung's Pharmacology 16e (Ch. 24); Bradley & Daroff's Neurology in Clinical Practice (Ch. 106)
This is a shared conversation. Sign in to Orris to start your own chat.