Okay, let me break all of this down for you, step by step, like we are sitting in a consultation room. This is going to be a long one, but you need to understand what is happening on your skin before you can fix it.
🧬 PART 1: What is Acne - The Basic Biology
Your skin has tiny structures called pilosebaceous units - that is a hair follicle with a sebaceous (oil) gland attached to it. These are everywhere on your face, chest, and back.
The sebaceous gland produces sebum (oil). Sebum is not bad - it protects your skin barrier, keeps it hydrated, and has antimicrobial properties. But when things go wrong inside that follicle, you get acne.
There are 4 core reasons acne happens, and in your case, all 4 are likely playing a role:
| Factor | What it does |
|---|
| 1. Excess sebum production | Clogs the pore from inside |
| 2. Abnormal shedding of skin cells inside the follicle (hyperkeratosis) | Dead cells don't shed normally, they stick together and block the pore |
| 3. Cutibacterium acnes (C. acnes) bacteria | Lives inside your follicle, feeds on sebum, triggers immune response |
| 4. Inflammation | Immune cells attack, causing redness, swelling, pus |
🔒 PART 2: How Closed Comedones Form (Your Puberty-Onset Pattern)
This is your original acne type - the one you've had since you were 12.
Here's what happens step by step:
Step 1: Androgens (testosterone, DHT) surge at puberty → sebaceous glands grow bigger → more sebum is produced.
Step 2: The cells lining the inside of the follicle canal start shedding abnormally - they clump together with sebum instead of flowing out normally.
Step 3: This forms a microcomedone - a microscopic blockage deep in the pore. You can't see this yet.
Step 4: The pore gets clogged. If the top of the pore is closed over by skin - that is a closed comedone (whitehead/bump with no dark center). If the top is open and oxidizes in air - that becomes a blackhead (not dirt, just oxidized sebum and melanin).
Why you get them when you crash diet: When you suddenly drop calories, your body goes into stress mode. Cortisol (stress hormone) spikes. Cortisol tells sebaceous glands to produce more oil AND it increases follicular hyperkeratosis (that sticky dead cell buildup). More oil + more sticky cells = more closed comedones. This is well documented - the sebaceous gland responds to corticotropin-releasing hormone (CRH), which is produced during stress, including physiological stress from dieting.
🔴 PART 3: How Inflammatory Acne Forms - With AND Without Pus
Once that closed comedone is sitting there, one of two things can happen:
Papule (inflammatory acne WITHOUT pus)
The wall of the blocked follicle gets irritated. C. acnes bacteria inside feeds on the sebum and releases fatty acids. Your immune system detects this and sends in neutrophils (white blood cells). The follicle wall becomes inflamed and red but has NOT ruptured yet. You see a red, tender bump under the skin. This is a papule - no visible pus, just inflammation.
Pustule (inflammatory acne WITH pus)
If the immune response escalates, the neutrophils accumulate and the follicle wall starts breaking down. The "pus" is just a collection of dead white blood cells, dead bacteria, and sebum. When it reaches the surface, the white/yellow center becomes visible. This is a pustule.
Nodule / Cyst
If the follicle wall ruptures deep in the dermis, it spills all that content into surrounding tissue. Your immune system mounts a much bigger response. This is a nodule (hard, painful, deep) or cyst (fluid-filled, softer). These cause the worst scarring and PIH (post-inflammatory hyperpigmentation).
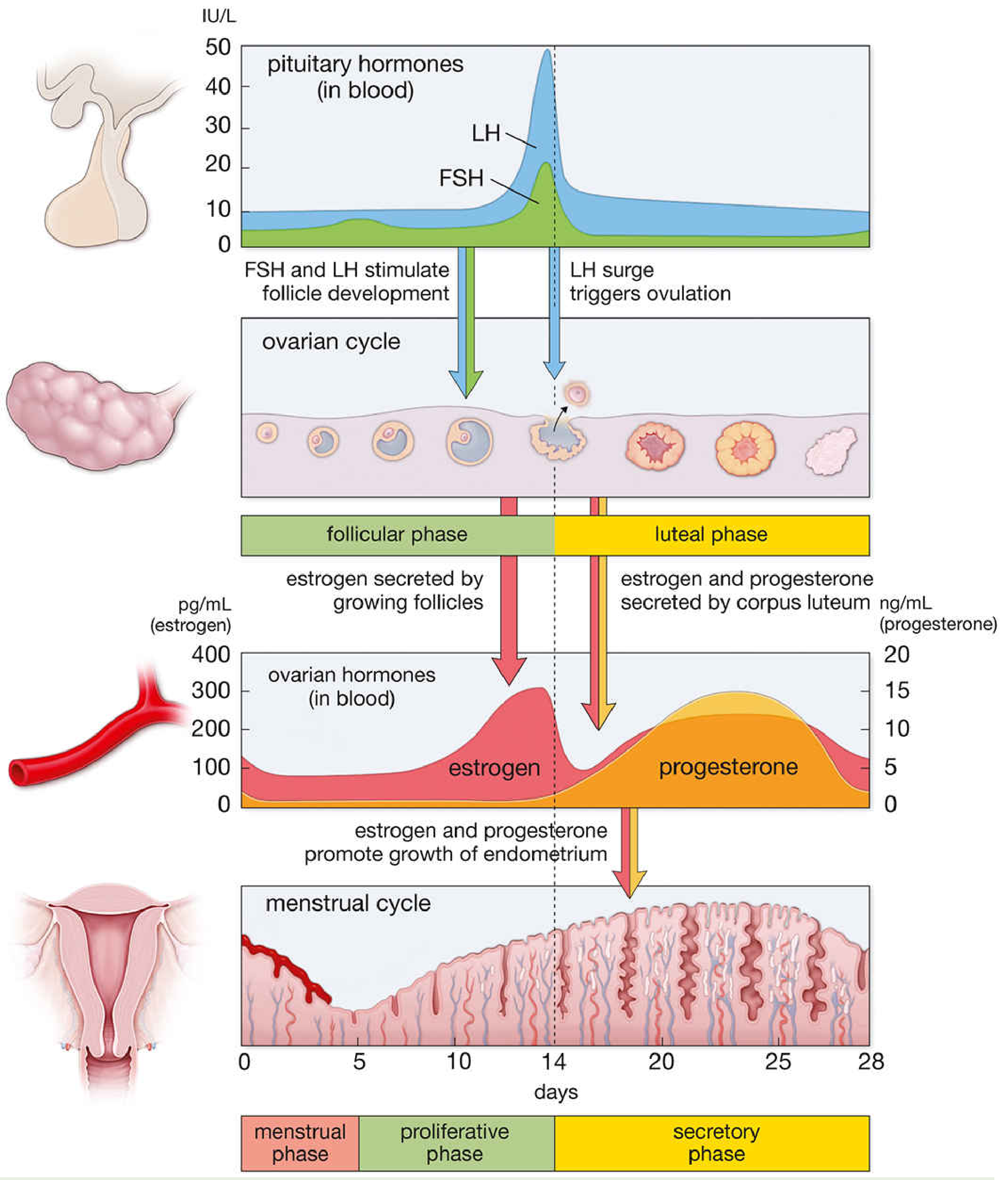
🩸 PART 4: Why Your Acne Worsens Around Your Period (Premenstrual Flares)
This is extremely common. Around 80% of women with acne report premenstrual flares. Here's the hormonal timeline:
Days 1-14 (follicular phase): Estrogen is dominant → estrogen has some anti-inflammatory and anti-sebum effects → skin is relatively calmer.
Around Day 14 (ovulation): Testosterone briefly spikes → sebum increases.
Days 15-28 (luteal phase): Progesterone rises. Progesterone has androgen-like activity and also promotes follicular keratosis. Sebum production goes up. Skin swells slightly due to water retention, which can compress pore openings.
Days 26-28 (just before your period): Estrogen and progesterone both drop sharply. This hormonal withdrawal triggers inflammation. C. acnes counts in the follicle are also highest in this phase. Result: inflammatory papules and pustules appear right before your period.
This is why you get more inflammatory acne (papules, pustules) around your period rather than just comedones - the comedones were already sitting there as microcomedones, and the hormonal shift converts them into inflamed lesions.
🍄 PART 5: Your History of Fungal Acne (Malassezia Folliculitis)
Fungal acne is not true acne at all. It's caused by Malassezia yeast, which normally lives on your skin. When conditions are right (humidity, sweat, disrupted skin barrier, certain ingredients), it overgrows inside follicles and causes folliculitis - small, uniform itchy bumps that look like comedones.
Important distinction: Malassezia feeds on fatty acids from certain oils and skincare ingredients. If you were ever using products with high oleic acid oils or certain emollients during that period, it could have triggered it.
💊 PART 6: Your Current Actives - What Each One Does and How to Use Them
Tazarotene (your current retinoid)
Tazarotene is a third-generation synthetic retinoid - it is stronger than tretinoin in comedolytic potency and has greater anti-inflammatory effects. It works by:
- Normalizing follicular keratinocyte differentiation - breaks up that sticky dead cell plug
- Preventing new microcomedones from forming
- Reducing inflammation around existing lesions
- Has some effect on PIH over time
Key fact: Tazarotene is the most potent topical retinoid and therefore the most irritating, especially on dry/sensitive skin. It is an upgrade from tretinoin in terms of strength. Because you have dry sensitive skin, retinoid irritation ("retinoid dermatitis" - dryness, peeling, stinging) is your main challenge.
When to use: PM only, after moisturizer (called the sandwich method or buffer method for sensitive skin: moisturize first → wait 10 min → apply tazarotene → moisturize again on top or the next morning). Never use on wet skin.
Benzoyl Peroxide (BPO)
BPO is a bactericidal agent - it kills C. acnes by releasing free oxygen radicals into the follicle. It also has mild comedolytic and anti-inflammatory effects.
- Works best at 2.5-5% concentration (same efficacy as 10%, less irritation)
- Important: do not layer BPO on top of vitamin C - they oxidize each other and cancel out
- BPO can bleach fabrics and hair - use on clean white pillowcases
- For dry sensitive skin: use as a spot treatment or short-contact wash, not a leave-on all over the face
Azelaic Acid (your Anua product)
Azelaic acid is underrated and perfect for your skin type. It does three things simultaneously:
- Antibacterial - kills C. acnes
- Comedolytic - normalizes keratinocyte turnover mildly
- Inhibits tyrosinase - fades PIH and is safe for melasma (one of the only topicals with good evidence for melasma and inflammatory acne at the same time)
- Anti-inflammatory
- Does NOT increase photosensitivity
This is the one active that is safe during breakouts AND helps with your dark spots/melasma. Using it only during breakouts is actually fine as a spot approach, but you could use it more broadly if you aren't getting irritation.
🧴 PART 7: Your Current Routine - What's Working, What Needs Adjusting
Let me go through your actual routine:
Morning Routine (AM)
You described: Vitamin C serum (Belo 15%) → Celimax toner → Azelaic acid (during breakouts) → LRP Mela B3 serum → CeraVe Moisturizing Cream → Y.O.U Sunscreen (blue cap)
Issues to address:
1. Vitamin C (Belo 15% L-ascorbic acid) + Niacinamide (LRP Mela B3)
There is a common concern that vitamin C and niacinamide together form nicotinic acid (niacin flush compound). In reality, at normal concentrations and normal skin temperature, this conversion is minimal and not clinically significant for most people. They can be layered - but if you notice flushing or pilling, separate them. Apply vitamin C first (it needs a low pH environment to penetrate), wait a few minutes, then apply the niacinamide serum.
2. Azelaic acid positioning: You are currently using it "only during breakouts." That's fine for spot treatment. But for consistent PIH and melasma management alongside your acne, you could use it as a leave-on over the whole face in the AM routine, between vitamin C and LRP Mela B3.
3. Celimax toner - what is it doing? If it's a hydrating toner (rice/centella type), it can go right after cleansing, before actives - that's fine. If it's an exfoliating toner (AHA/BHA), do NOT combine that with your retinoid nights and be cautious stacking exfoliation.
4. Sunscreen - your most important step. You have mild melasma + PIH. Without high SPF protection every single morning, ALL your actives (vitamin C, azelaic acid, retinoid, niacinamide) are fighting uphill. Every UV exposure deepens your melasma. The Y.O.U sunscreen (blue cap - their Aqua Mineral SPF 50) is a reasonable choice.
Evening Routine (PM)
You didn't fully list your PM routine, but you are on tazarotene. Here's what it should look like:
Recommended PM order:
- Gentle cleanser (something like CeraVe Hydrating Cleanser - no foaming strips)
- Hydrating toner (Celimax - if hydrating)
- CeraVe Moisturizing Cream (buffer)
- Tazarotene - apply to DRY skin, thin layer, avoid eye area and corners of mouth
- Optional: second thin layer of CeraVe over the top if very dry
Do NOT use BPO and tazarotene on the same night - that doubles irritation. You can alternate: BPO nights vs tazarotene nights, or use BPO as a morning spot treatment only.
📋 PART 8: Suggested Revised Routine for You
AM (Morning)
| Step | Product | Why |
|---|
| 1. Cleanser | Gentle, non-stripping | Prep |
| 2. Toner | Celimax (hydrating) | Hydration before actives |
| 3. Vitamin C | Belo 15% | Antioxidant, brightening, fades PIH |
| 4. Azelaic Acid | Anua (daily, whole face) | Acne + PIH + melasma - workhorse |
| 5. Niacinamide serum | LRP Mela B3 | Further PIH/melasma correction |
| 6. Moisturizer | CeraVe Moisturizing Cream | Barrier repair - critical for dry skin |
| 7. Sunscreen | Y.O.U blue cap SPF 50 | NON-NEGOTIABLE - protects melasma |
PM (Evening)
| Step | Product | Why |
|---|
| 1. Double cleanse | Oil cleanser + gentle cleanser | Remove sunscreen properly |
| 2. Toner | Celimax | Hydration |
| 3. Moisturizer | CeraVe (thin layer first - buffer) | Reduces tazarotene irritation |
| 4. Tazarotene | Thin pea-size for whole face | Comedolytic + anti-inflammatory |
| BPO | Use on alternate nights OR spot-treat only | Anti-bacterial |
⚠️ PART 9: Special Notes for Your Situation
During your period:
- Inflammatory acne is expected due to hormonal changes - do NOT panic-spot-treat with everything at once
- Stick to azelaic acid + BPO spot treatment on active pustules
- Do NOT increase retinoid frequency - your skin is already sensitized
- Keep barrier repair as priority: CeraVe is your best friend these days
During or after a crash diet:
- Cortisol rises → sebum rises → closed comedones appear within 2-3 weeks
- The fix is not more actives - it is eating enough, especially healthy fats (omega-3s) and reducing refined sugar and high glycemic index foods (evidence links high GI diet to acne flares)
- Consistent retinoid use prevents the comedones from forming in the first place
For your melasma:
- Mild forehead melasma responds well to: daily SPF (primary treatment), azelaic acid, niacinamide
- The LRP Mela B3 serum (niacinamide-based) is a smart addition
- Do NOT skip sunscreen even on cloudy or indoor days - visible light and heat also trigger melasma
- Tazarotene over time also helps with mottled pigmentation (off-label use for melasma is established)
Fungal acne (if it comes back):
- Malassezia folliculitis looks like uniform, slightly itchy bumps, usually same size
- Avoid products with high oleic-acid oils (coconut oil, olive oil) if Malassezia is active
- Azelaic acid and BPO are NOT effective against Malassezia - antifungal treatment is needed
- If it returns, see a dermatologist for topical ketoconazole or ciclopirox
🔑 Quick Summary
- Your acne history makes total sense: hormonal onset → closed comedones → hormonal/diet triggers → inflammatory flares perimenstrually
- Tazarotene is your strongest tool - use it consistently at night, buffered with moisturizer
- BPO is for bacterial targeting - use it carefully, not nightly with tazarotene
- Azelaic acid (Anua) is your daily workhorse - safe for melasma, acne, and PIH simultaneously
- Vitamin C AM + Niacinamide (LRP Mela B3) AM are a good brightening stack - can be layered with a gap
- Sunscreen daily is not optional - it is the most important thing you can do for your melasma
- Do NOT use more actives during a breakout - you need less, not more, on sensitized skin
(Clinical references: Dermatology 2-Volume Set 5e, Ch. 36 "Acne Vulgaris"; Katzung's Pharmacology 16e "Retinoic acid/Tazarotene"; Goodman & Gilman's Pharmacology "Acne")
Is there any specific part you want me to go deeper on - like the period-acne link, how to layer your products exactly, or whether tazarotene is right for your skin type?