Total Abdominal Hysterectomy with Bilateral Salpingo-Oophorectomy.
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
Reading File
Searching PubMed
"total abdominal hysterectomy" outcomes complications
Loading Image
Loading Image
Reading File
Searching PubMed
hysterectomy surgical approach outcomes
That covers TAH-BSO comprehensively. Here's a quick orientation to each section:
- Indications — separated into malignant (where BSO is mandatory) vs. benign (where ovarian conservation decisions are nuanced), plus prophylactic BSO for high-risk genetics
- Surgical technique — step-by-step with intraoperative images from Sabiston and Schwartz's showing the key pedicle divisions
- Complications — organized intraoperatively vs. postoperatively, including the long-term hormonal sequelae unique to BSO in premenopausal women
- Perioperative care — covers the full continuum from NPO to discharge to activity restrictions
- Route comparison — contextualizes when open TAH remains appropriate vs. minimally invasive alternatives, supported by the 2023 Cochrane review
Let me know if you'd like to go deeper on any specific aspect — e.g., management of ureteral injury, hormonal considerations post-BSO, oncologic staging procedures, or the laparoscopic technique.
Bartholin cyst
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Searching PubMed
"Bartholin" cyst treatment
Excellent — I have everything needed. Here is the comprehensive overview:
Bartholin Cyst (Bartholin Duct Cyst & Abscess)
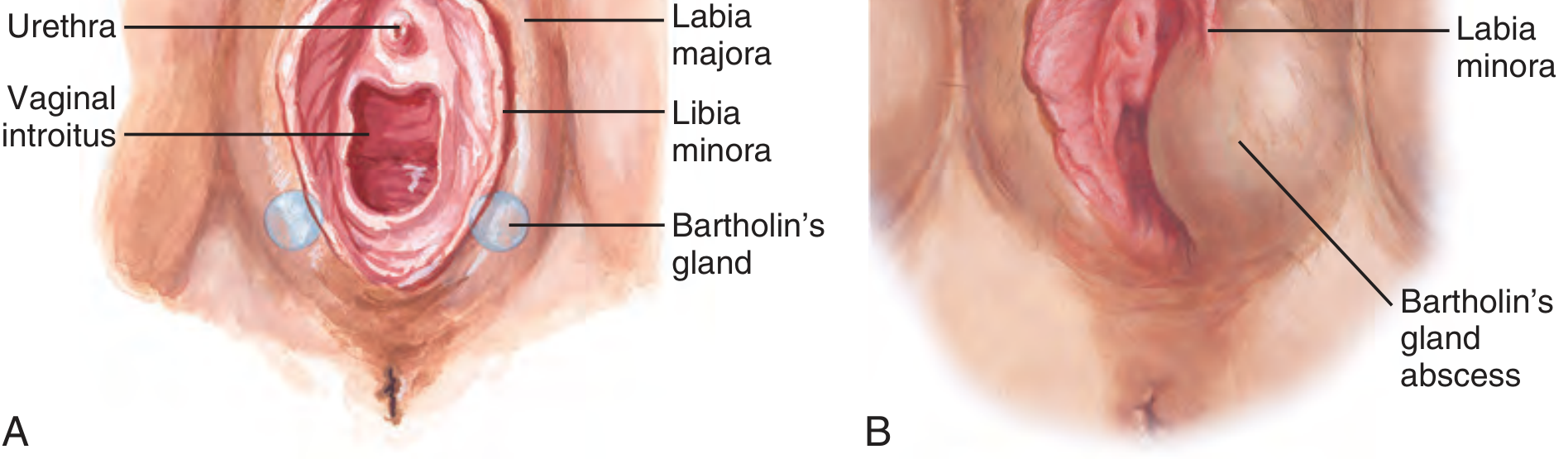
Anatomy
The Bartholin glands (greater vestibular glands) are paired, pea-sized, mucus-secreting glands located bilaterally in the posterior labia minora. Their ducts drain into the vaginal vestibule at the 4 o'clock and 8 o'clock positions (some sources describe this as 5 and 7 o'clock). They begin functioning at puberty — providing vestibular moisture/lubrication — and involute after menopause. In the normal state they are not palpable.
Pathophysiology
Obstruction of the Bartholin duct — most often by an inflammatory process — causes mucus accumulation, producing a cyst. If the stagnant secretions become infected, the gland fills with pus, forming a Bartholin abscess. Importantly, an abscess can develop without a preceding cyst.
"Obstruction of the duct may result in a cyst or abscess. A cyst does not need to be present before an abscess can develop." — Tintinalli's Emergency Medicine
Histology: Cysts are lined by transitional or squamous epithelium. They can grow up to 3–5 cm in diameter.
Epidemiology
- Occur at all ages, predominantly in reproductive-age women
- Bartholin abscesses affect approximately 2% of women
- Uncommon after menopause (gland involutes); any Bartholin gland mass in a woman >40 years must raise suspicion for malignancy
Microbiology (Abscess)
Bartholin abscesses are typically polymicrobial:
| Organism | Notes |
|---|---|
| Escherichia coli | Most common isolate |
| Staphylococcus aureus (incl. MRSA) | Culture purulent fluid |
| Streptococcus spp. | Polymicrobial mix |
| Neisseria gonorrhoeae | Less common; treat if suspected |
| Chlamydia trachomatis | Less common; treat if suspected |
Clinical Features
Bartholin Duct Cyst
- Unilateral, smooth, fluctuant mass at the posterior vestibule (4 or 8 o'clock)
- Often asymptomatic if small
- Larger cysts cause local pressure, discomfort, dyspareunia
- No erythema or warmth (unless infected)
Bartholin Abscess
- Rapidly enlarging, extremely painful mass at same location
- Induration, erythema, fluctuance
- Patient may have difficulty walking or sitting
- Systemic symptoms (fever, chills) are rarely present — their absence does not exclude an abscess
- Develops over several days (or longer if preceded by a cyst)
Diagnosis
Primarily clinical — based on history and examination:
- Characteristic location at posterior introitus (labia minora transecting the mass)
- Fluctuance confirms abscess
Ultrasound can confirm a discrete fluid collection when the diagnosis is uncertain or if the abscess is not clearly defined.
Caution: Distinguish a Bartholin abscess from an abscess of the labia majora, which requires gynecologic consultation. Any solid component or atypical appearance in a woman >40 warrants biopsy to exclude carcinoma.
Treatment
Management depends on whether it is a cyst or abscess, and on recurrence:
1. Asymptomatic Cyst
- No treatment required — observation is appropriate for small, asymptomatic cysts
2. Symptomatic Cyst or Abscess — First-line: Word Catheter
The Word catheter (a small catheter with an inflatable balloon tip) is the most widely used office/ED procedure.
Technique:
- Patient in dorsal lithotomy position; identify abscess at 5 or 7 o'clock with labia minora transecting it
- Analgesia: 2–4 mL 1% lidocaine infiltrated through the mucosal surface (not skin surface); IV opioids/procedural sedation for severe pain
- #11 scalpel — stab incision on the mucosal surface of the vestibule, just lateral to the hymenal ring, where fluctuance is maximal. Incision must be large enough for catheter, but not so large the balloon is displaced
- Alternatively: stabilize abscess with thumb/index finger and "skewer" onto a hemostat for entry
- Drain pus (expect a palpable pop and free flow of pus); insert Word catheter to the hilt
- Inflate balloon with 2–4 mL saline; tuck catheter end into vagina
- Catheter remains in place 4–6 weeks to allow epithelialization of a new permanent duct opening
- Send pus for culture (including MRSA, GC, chlamydia)
- Prescribe analgesics; antibiotics after drainage are of no proven value routinely (cover GC/CT if suspected)
3. Recurrent Cyst/Abscess — Marsupialization
The preferred definitive procedure for recurrent disease. Performed under local, spinal, or general anesthesia.
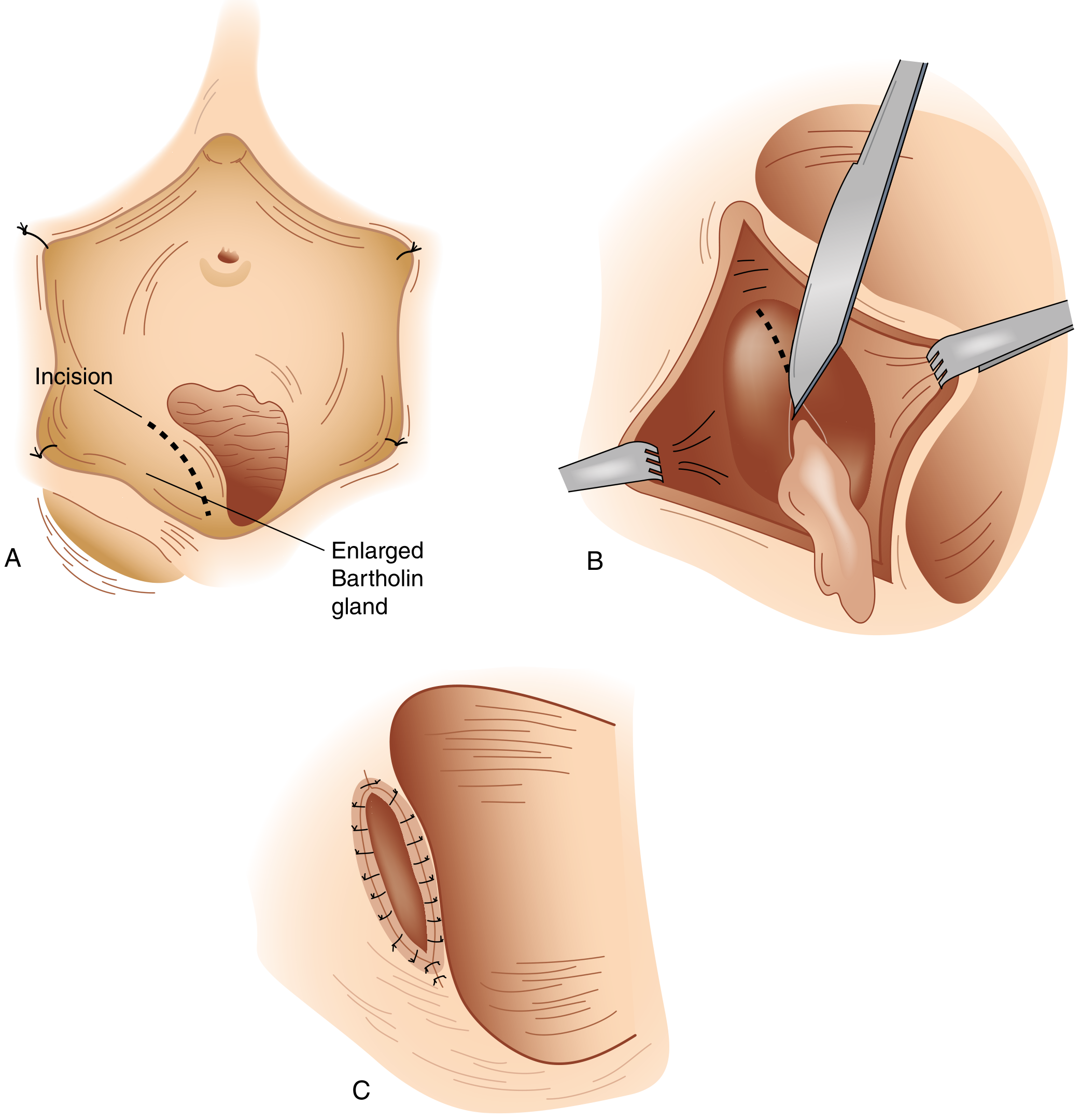
Technique:
- Patient in dorsal lithotomy; local anesthetic (2% lidocaine ± epinephrine) or pudendal block
- Retract labium laterally; identify incision site internal to the hymenal ring (mucosa, not skin)
- Longitudinal fusiform incision 1–2 cm wide over the cyst wall; excise an ellipse of mucosa
- Grasp cyst wall with two hemostats before segment is removed; cyst will decompress
- Break up any loculations with small hemostats; irrigate with normal saline
- In patients >40 years: inspect interior for neoplastic-appearing epithelium; send for biopsy
- Suture cyst wall edge to adjacent vaginal mucosa with interrupted 4-0 Vicryl — this is the marsupialization step, suturing the cavity open permanently
- Minimum gap of ≥1 cm across the open marsupialization
- No dressing required; sitz baths daily for 3–4 days
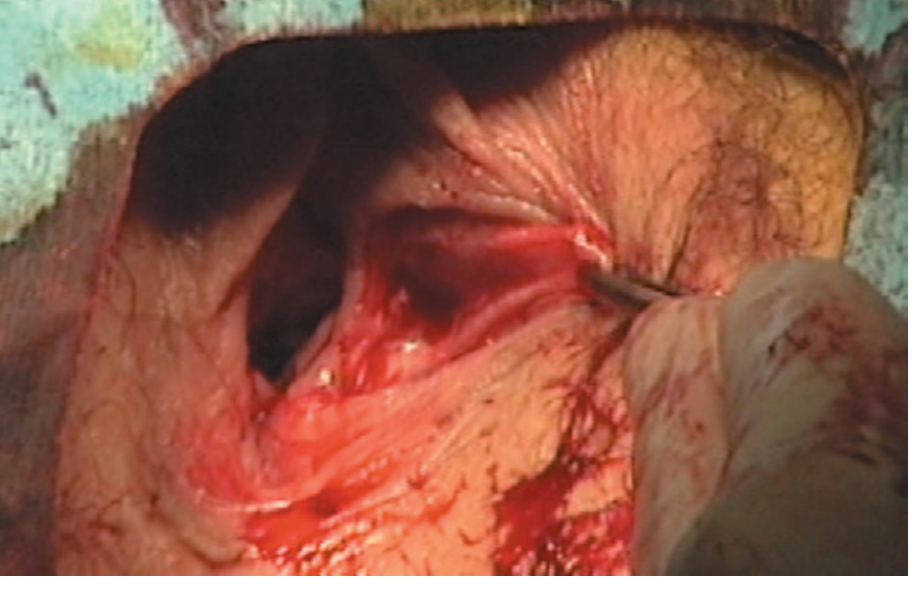
4. Failed/Persistent Cases — Complete Gland Excision
Reserved for cysts or abscesses that fail to resolve after drainage, recurrent disease not amenable to marsupialization, or suspicion of malignancy.
- Technically more demanding; risks include hemorrhage and hematoma
- A common surgical error is making the incision on the lateral vulvar skin rather than the vestibular mucosa
CPT / Procedure Codes
| Procedure | CPT |
|---|---|
| I&D of vulvar/perineal abscess | 56405 |
| I&D of Bartholin's gland cyst/abscess | 56420 |
| Marsupialization of Bartholin's gland cyst | 56440 |
| Excision of Bartholin's gland | 56740 |
Bartholin Gland Carcinoma
Although rare, carcinoma can arise from the Bartholin gland. Types include:
- Squamous cell carcinoma (most common)
- Adenocarcinoma
- Adenoid cystic carcinoma (characteristically slow-growing, perineural invasion)
- Transitional cell carcinoma
Key rule: A biopsy with histologic evaluation is indicated for all cases with a palpable or visible solid mass within a Bartholin cyst or abscess, and in all instances where a presumed Bartholin gland lesion occurs in women over 40 years of age. — Berek & Novak's Gynecology
Special Considerations
| Situation | Action |
|---|---|
| Large abscess, uncertain diagnosis, significant cellulitis | Gynecology consultation |
| Unstable vitals, bleeding dyscrasia, immunocompromised | Gynecology to manage (possibly OR) |
| Abscess not yet walled-off | Broad-spectrum antibiotics + warm sitz baths + close follow-up; I&D when fluctuant |
| N. gonorrhoeae / C. trachomatis suspected | Treat per STI guidelines (ceftriaxone + doxycycline) |
| MRSA on culture | Treat with appropriate antibiotics (TMP-SMX, clindamycin) |
| Woman >40 years | Biopsy to exclude malignancy |
| Postmenopausal new Bartholin mass | Malignancy until proven otherwise |
Summary Algorithm
Bartholin lesion
│
├── Asymptomatic cyst → Observe
│
├── Symptomatic cyst or abscess (1st episode)
│ → Word catheter (4–6 weeks)
│
├── Recurrent cyst/abscess
│ → Marsupialization
│
├── Failed marsupialization / persistent
│ → Complete gland excision
│
└── Solid mass / age >40 / postmenopausal
→ Biopsy to exclude carcinoma
Sources: Tintinalli's Emergency Medicine | Robbins & Cotran Pathologic Basis of Disease | Berek & Novak's Gynecology | Sabiston Textbook of Surgery | Schwartz's Principles of Surgery | Roberts & Hedges' Clinical Procedures in Emergency Medicine | Pfenninger & Fowler's Procedures for Primary Care
This is a shared conversation. Sign in to Orris to start your own chat.