10 most common ecg diagnosis and findings
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Loading Image
Here is a thorough, textbook-grounded breakdown of the 10 most common ECG diagnoses and findings:
10 Most Common ECG Diagnoses and Findings
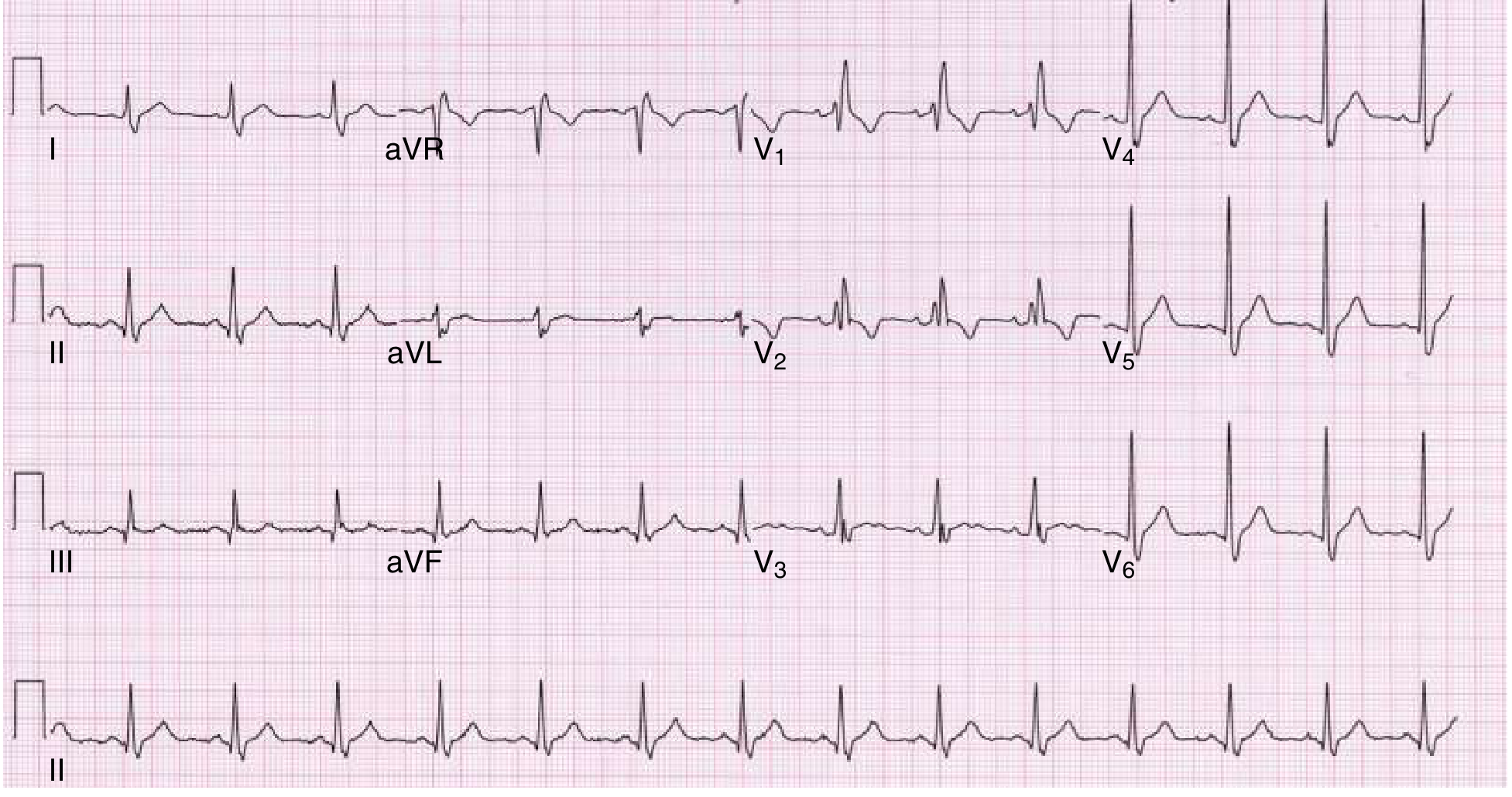
1. Normal Sinus Rhythm (Baseline Reference)
Before recognizing pathology, every ECG is assessed against normal:
- Rate: 60-100 bpm
- P wave: upright in leads I and II, precedes every QRS
- PR interval: 120-200 ms
- QRS: <120 ms, axis -30° to +90°
- QT interval: <450 ms (men), <470 ms (women)
2. Sinus Tachycardia
- Rate: >100 bpm with a normal P-QRS-T sequence
- P waves are upright and precede each QRS (1:1 relationship)
- Most common dysrhythmia seen on ECG overall - present in ~40% of emergency patients with acute illness (e.g. PE, thyrotoxicosis, sepsis)
- Not a primary arrhythmia - always look for the underlying cause
3. Atrial Fibrillation (AF)
One of the most clinically important and frequently encountered diagnoses:
- Absent P waves - replaced by irregular, chaotic fibrillatory (f) waves, best seen in V1
- Irregularly irregular ventricular response (RR intervals vary with no pattern)
- Narrow QRS unless aberrant conduction or bundle branch block co-exists
- When AF is associated with pulmonary hypertension, the ECG may show: R/S ratio in V1 >1, right axis deviation, and ST depressions in V1-V3 (Tintinalli's Emergency Medicine)
- Common in mitral stenosis: ECG shows AF, left atrial enlargement, or right axis deviation
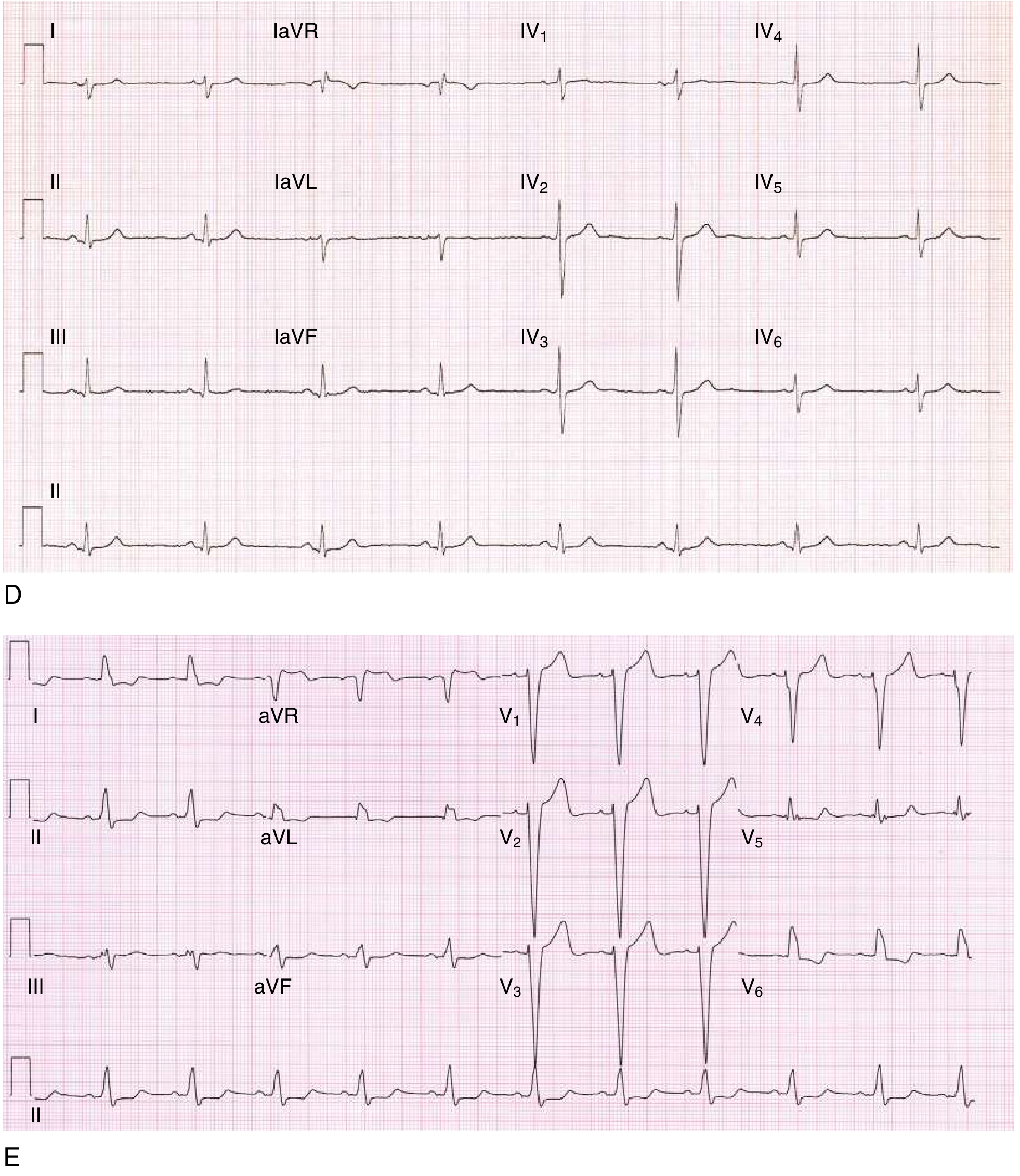
4. Left Ventricular Hypertrophy (LVH)
The most common ECG finding in hypertensive patients and dilated cardiomyopathy:
- Voltage criteria - Several exist; all have poor sensitivity (30-50%) but good specificity (85-95%)
- Cornell criterion: S in V3 + R in aVL >28 mm (men) or >20 mm (women)
- Sokolow-Lyon: S in V1 + R in V5 or V6 >35 mm
- Associated with ST depression and T wave inversion in lateral leads ("strain pattern")
- LV hypertrophy + left atrial enlargement are the most common findings in dilated cardiomyopathy (Tintinalli's)
5. Right Bundle Branch Block (RBBB)
ECG hallmarks (from Goldman-Cecil and Braunwald's):
- QRS duration ≥120 ms
- rsR' pattern ("M-shape") in V1 - the classic finding
- Wide, slurred terminal S wave in leads I, V5, V6
- ST-segment downsloping and T wave inversion in right precordial leads (V1-V3) - discordant with QRS
- Normal axis; septal Q waves present in lateral leads
- Can be isolated or combined with left anterior fascicular block (bifascicular block)
6. Left Bundle Branch Block (LBBB)
ECG hallmarks:
- QRS duration ≥120 ms
- Broad, notched (M-shaped) complex in I, aVL, and left precordial leads (V5-V6)
- Small r waves and broad, deep S waves in right precordial leads (V1-V3)
- ST and T waves discordant (opposite to) the QRS throughout the precordium
- Axis usually normal or deviated left
- New LBBB in a patient with chest pain is treated as a STEMI equivalent
7. ST-Elevation Myocardial Infarction (STEMI)
The highest-stakes ECG diagnosis:
- ST elevation ≥1 mm in ≥2 contiguous limb leads, or ≥2 mm in ≥2 contiguous precordial leads
- Reciprocal ST depression in opposite leads
- Hyperacute T waves - earliest finding (tall, broad, asymmetric)
- Pathological Q waves - develop within hours to days (>40 ms wide or >25% of R wave height)
- Localizing territory:
- Inferior (II, III, aVF) = RCA occlusion
- Anterior (V1-V4) = LAD occlusion
- Lateral (I, aVL, V5-V6) = LCx occlusion
- STEMI management target: door-to-balloon <90 min; primary PCI preferred over thrombolysis (Textbook of Family Medicine)
- New LBBB or posterior STEMI (ST depression V1-V3 with tall R waves) are STEMI equivalents
8. Non-Specific ST-T Wave Changes
The most common "abnormal" finding on routine ECGs:
- ST depression or T wave inversion that does not meet ischemia criteria
- T wave flattening or subtle inversion
- Causes are extensive: ischemia, LVH strain, electrolyte disturbance (hypokalemia), digoxin effect, myocarditis, pericarditis, cardiomyopathy
- Must always be interpreted in clinical context
- Sinus tachycardia + nonspecific ST-T changes are the most common ECG findings in pulmonary embolism - they do NOT confirm or exclude the diagnosis
9. First-Degree AV Block (and Fascicular Blocks)
First-degree AV block:
- PR interval >200 ms (>5 small squares)
- Every P wave conducts to a QRS - no beats dropped
- Often benign; seen in athletes, with inferior MI, or drug effect (beta-blockers, digoxin)
Fascicular blocks are also very common:
- Left anterior fascicular block (LAFB): Left axis deviation (around -60°), normal QRS duration, small Q waves in I/aVL, small R waves in II/III/aVF
- Left posterior fascicular block (LPFB): Right axis deviation (~+120°), delayed R-wave progression, requires exclusion of other causes of right axis deviation
10. Ventricular / Atrial Premature Beats
- Premature Ventricular Complexes (PVCs): Wide, bizarre QRS (>120 ms), no preceding P wave, full compensatory pause. Very common - seen in up to 30% of monitored patients. Usually benign in isolation but complex forms (couplets, bigeminy, multifocal) warrant evaluation
- Premature Atrial Complexes (PACs): Early, narrow QRS preceded by an abnormal P wave; often conducted with a slight PR change or blocked entirely
- Both are documented in ECG recording tables from Braunwald's Heart Disease and Goldman-Cecil as top findings in long-term Holter monitoring
Summary Table
| # | Diagnosis | Key ECG Feature |
|---|---|---|
| 1 | Normal sinus rhythm | Rate 60-100, regular P-QRS-T |
| 2 | Sinus tachycardia | Rate >100, normal morphology |
| 3 | Atrial fibrillation | No P waves, irregularly irregular RR |
| 4 | LVH | Increased voltage ± strain pattern |
| 5 | RBBB | rSR' in V1, wide S in I/V5/V6 |
| 6 | LBBB | Broad notched R in I/aVL/V6, deep S in V1 |
| 7 | STEMI | ST elevation ≥1-2 mm in contiguous leads |
| 8 | Nonspecific ST-T changes | ST depression/T inversion, nondiagnostic |
| 9 | First-degree AV block / fascicular blocks | PR >200 ms / axis deviation |
| 10 | PVCs / PACs | Wide bizarre QRS / early narrow QRS |
Sources: Goldman-Cecil Medicine, Braunwald's Heart Disease, Tintinalli's Emergency Medicine, Textbook of Family Medicine - all via the medical textbook library.
This is a shared conversation. Sign in to Orris to start your own chat.