Nephrotic syndrome
Reading File
Finding Sources
Searching PubMed
"nephrotic syndrome"[MeSH Terms] AND management
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information to compile a thorough answer. Let me put it all together.
Nephrotic Syndrome
Definition
Nephrotic syndrome is a clinical syndrome defined by four cardinal features:
| Feature | Threshold |
|---|---|
| Proteinuria | >3.5 g/day in adults; >50 mg/kg/day or >40 mg/m²/hr in children |
| Hypoalbuminemia | Serum albumin <3 g/dL |
| Generalized edema | Periorbital, peripheral, may progress to anasarca |
| Hyperlipidemia + Lipiduria | Elevated cholesterol, TG, LDL, lipoprotein(a); oval fat bodies/fatty casts in urine |
In practice, many clinicians refer to "nephrotic-range proteinuria" even when the full syndrome is not present. - Goldman-Cecil Medicine, p. 1250
Pathophysiology
The glomerular capillary wall (endothelium + GBM + podocytes) acts as a size and charge barrier. Structural or physicochemical damage increases permeability, allowing plasma proteins to escape into the urine.
Cascade of consequences:
- Heavy proteinuria - depletes serum albumin faster than the liver can compensate; renal catabolism of filtered albumin adds to losses
- Hypoalbuminemia - reduces plasma oncotic pressure
- Edema - two mechanisms coexist:
- Underfill: low oncotic pressure → fluid shifts to interstitium → intravascular volume falls → RAAS activated → Na/water retention (especially in minimal change disease)
- Overfill: primary renal Na retention in distal nephron and TAL, independent of RAAS (more common in other causes)
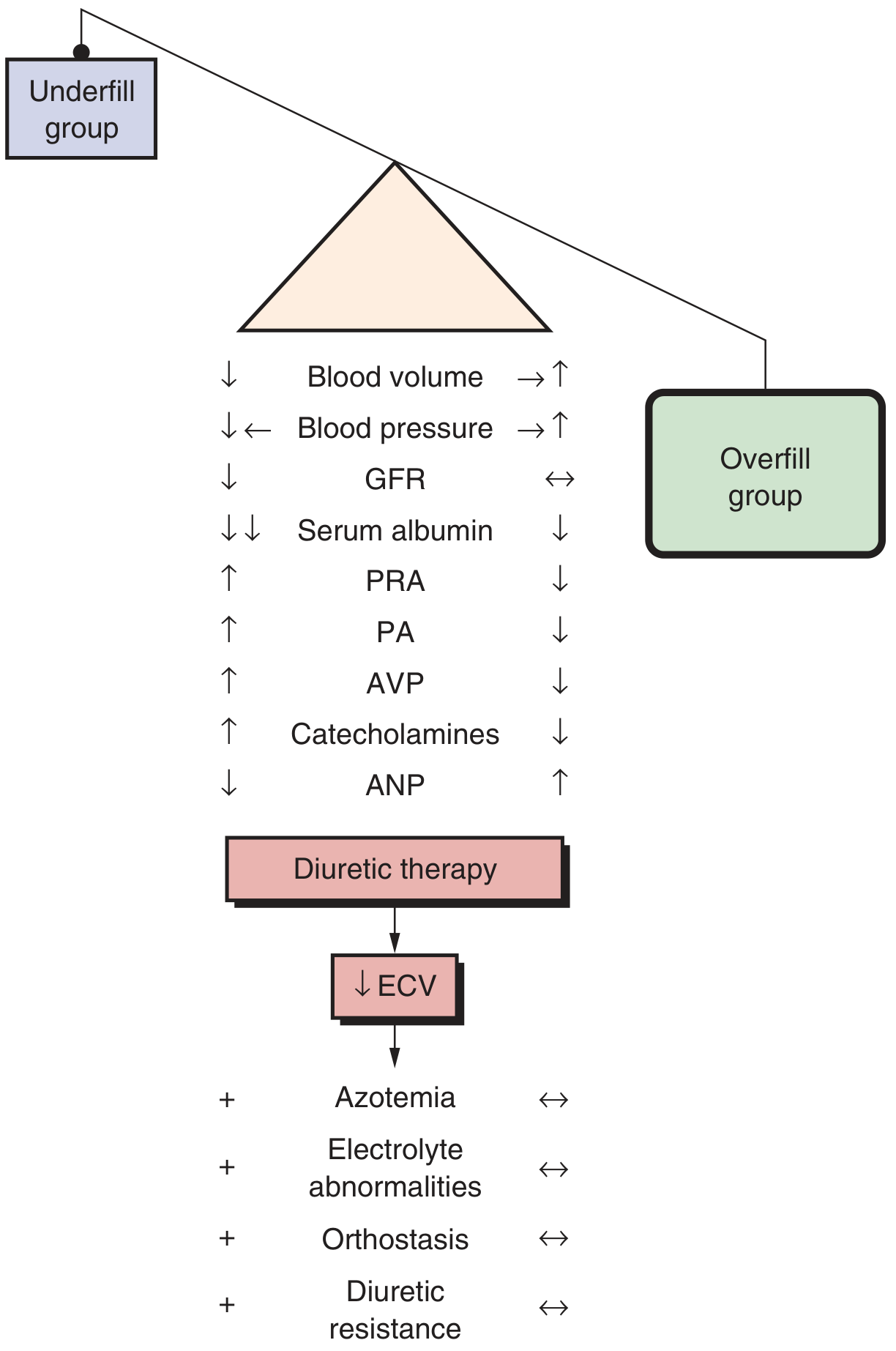
Fig. Underfill vs. overfill groups differ in blood volume, PRA, aldosterone, AVP, catecholamines, and ANP - and have opposite responses to diuresis. - Brenner & Rector's The Kidney
- Hyperlipidemia - low oncotic pressure upregulates hepatic apolipoprotein synthesis; impaired lipid catabolism; elevated cholesterol, TG, VLDL, LDL, lipoprotein(a); HDL may be reduced
- Lipiduria - lipoproteins cross the damaged barrier; appear as free fat, oval fat bodies, or fatty casts
- Robbins & Cotran Pathologic Basis of Disease, p. 844
Causes
Primary (Idiopathic) Glomerular Diseases
| Cause | Children | Adults |
|---|---|---|
| Minimal change disease | ~75% | ~5-10% |
| FSGS | ~10% | ~20-35% |
| Membranous nephropathy | ~3% | ~25-30% |
| MPGN | ~10% | ~5-10% |
| Other proliferative GN (IgA, etc.) | ~2% | ~15-17% |
Primary disease accounts for ~95% of nephrotic syndrome in children and ~60% in adults. - Robbins & Cotran, p. 845
Secondary Causes
Systemic diseases: Diabetes mellitus (most common overall), SLE, amyloidosis (AL/AA)
Infections: Hepatitis B/C, HIV, malaria (especially quartan/P. malariae), syphilis, CMV, EBV, schistosomiasis, filariasis
Drugs/toxins: NSAIDs, gold, penicillamine, mercury, lithium, captopril, heroin, pamidronate, rifampin, contrast media
Malignancies: Hodgkin lymphoma/leukemias (associated with MCD pattern); solid tumors - lung, colon, melanoma (associated with membranous nephropathy)
Hereditary/metabolic: Alport syndrome, Fabry disease, sickle cell, genetic podocytopathies (mutations in nephrin/NPHS1, podocin/NPHS2, WT1, APOL1)
Other: Obesity (adaptive FSGS), preeclampsia, chronic allograft nephropathy, renal artery stenosis, reflux nephropathy
Major Histological Subtypes
1. Minimal Change Disease (MCD)
- LM: Normal glomeruli (hence the name)
- EM: Diffuse effacement (fusion) of podocyte foot processes - the hallmark
- IF: Negative (no immune deposits)
- Pathogenesis: Circulating factor (possibly T-cell-derived) damages the negative charge on the GBM; recent evidence points to anti-nephrin autoantibodies
- Most common cause in children; strongly associated with Hodgkin lymphoma and NSAID use in adults
- Excellent response to steroids (>80-90% remission in children)
2. Focal Segmental Glomerulosclerosis (FSGS)
- LM: Segmental sclerosis (obliteration) of portions of some (not all) glomeruli
- EM: Foot process effacement
- Variants: NOS, tip, perihilar, cellular, collapsing (most aggressive - associated with HIV/COVID nephropathy)
- APOL1 risk alleles (G1/G2) strongly increase risk in individuals of African descent
- Adaptive forms: obesity-related FSGS, remnant kidney, reflux nephropathy
- Steroid resistance is common; may progress to ESKD
3. Membranous Nephropathy (MN)
- LM: Diffuse thickening of glomerular capillary walls; "spike and dome" pattern on silver stain
- EM: Subepithelial electron-dense deposits
- IF: Granular IgG and C3 along capillary loops
- Pathogenesis: Autoantibodies against podocyte surface antigens - most commonly anti-PLA2R (~60% of primary MN); less often NELL1, THSD7A, EXT1/2, NCAM1/CD10
- ~75% primary; ~25% secondary (HBV, SLE, solid tumors, drugs)
- Most common cause of nephrotic syndrome in older adults (especially Whites)
- Anti-PLA2R antibodies serve as diagnostic and prognostic markers
4. Membranoproliferative GN (MPGN)
- Mixed nephritic-nephrotic pattern; low complement levels
- LM: "Tram-track" (double contour) of GBM due to mesangial interposition
- Classified by IF/EM into immune complex-mediated vs. complement-mediated (C3 glomerulopathy)
Complications
| Complication | Mechanism |
|---|---|
| Infection (pneumococcal, staphylococcal, peritonitis) | Loss of IgG, complement factors, opsonins in urine |
| Thromboembolism (DVT, PE, renal vein thrombosis) | Loss of antithrombin III, protein C, protein S; elevated fibrinogen, factor VIII; hypercoagulability |
| Atherosclerosis/CVD | Persistent hyperlipidemia, elevated LDL, lipoprotein(a) |
| AKI | Volume depletion, diuretic excess, thrombosis, or interstitial nephritis |
| Malnutrition/growth failure | Ongoing protein wasting |
| Drug toxicity | Altered albumin binding changes free drug levels |
Renal vein thrombosis - once thought to cause nephrotic syndrome - is now recognized as a consequence of the hypercoagulable state, especially in membranous nephropathy. - Robbins & Cotran, p. 844
Diagnosis
Initial workup:
- 24-hr urine protein (or urine protein/creatinine ratio)
- Serum albumin, lipid panel, BMP/CBC
- ANA, anti-dsDNA - for lupus
- Fasting glucose, HbA1c - for diabetes
- Hepatitis B/C serology, HIV
- Serum complement (C3/C4) - low in SLE, MPGN, cryoglobulinemia; normal in MCD, FSGS, MN
- SPEP/UPEP - for amyloidosis/myeloma
- Anti-PLA2R antibody - for primary MN (avoids biopsy in some cases)
- ANCA, anti-GBM - if overlap with nephritic features
Kidney biopsy is usually required in adults to confirm diagnosis, determine prognosis, and guide treatment. It is generally not done in children with the classic MCD presentation (first presentation, age 1-8, full nephrotic syndrome without hematuria/hypertension/renal impairment), as empirical steroid treatment is standard.
Treatment
General/Supportive Measures
- Edema: Low-sodium diet (<2 g/day) + loop diuretics (furosemide) as first-line; spironolactone can be added. IV albumin + furosemide for severe, refractory cases with volume depletion
- Proteinuria reduction: ACE inhibitors or ARBs reduce proteinuria, preserve GFR, and ameliorate edema and hyperlipidemia regardless of cause
- Hyperlipidemia: Statins - though evidence for benefit specifically from nephrotic-hyperlipidemia is limited
- Anticoagulation: Warfarin if thrombotic complications occur; also recommended in membranous nephropathy with albumin <2.8 g/dL and low bleeding risk. DOACs data remain insufficient
- Infection prophylaxis: Pneumococcal vaccination
Disease-Specific Immunosuppression
| Condition | First-line | Second-line/Resistant |
|---|---|---|
| MCD | Prednisone 1 mg/kg/day (adults); high remission rate | Cyclophosphamide, CNIs (tacrolimus/cyclosporine) for frequent relapsers |
| FSGS (primary) | High-dose prednisone | Cyclosporine, tacrolimus, mycophenolate, rituximab (for steroid-resistant) |
| Membranous nephropathy | Conservative (ACE/ARB) for low-risk; Rituximab (preferred for moderate/high risk); KDIGO supports rituximab as first-line | Cyclosporine + steroids; cyclophosphamide + steroids |
| Secondary causes | Treat underlying disease | - |
| Diabetic nephropathy | RAAS blockade; SGLT2 inhibitors (reduced proteinuria and progression); GLP-1 RA | - |
Nephrotic vs. Nephritic Syndrome - Key Distinction
| Feature | Nephrotic | Nephritic |
|---|---|---|
| Proteinuria | Massive (>3.5 g/day) | Mild-moderate |
| Hematuria | Absent or minimal | Prominent (RBC casts) |
| Edema | Marked | Present but less severe |
| Hypertension | Variable | Prominent |
| GFR/Azotemia | Usually preserved | Often reduced |
| Complement | Normal (MCD, FSGS, MN) | Low (post-strep GN, SLE, MPGN) |
Some diseases (MPGN, lupus nephritis, IgA nephropathy) can present with a mixed nephrotic-nephritic picture.
Recent evidence note: A 2025 Cochrane systematic review (PMID 40337980) specifically examined interventions for idiopathic steroid-resistant nephrotic syndrome in children, confirming ongoing uncertainty about optimal immunosuppression in this difficult subgroup.
Sources: Brenner & Rector's The Kidney | Robbins & Cotran Pathologic Basis of Disease | Goldman-Cecil Medicine | Comprehensive Clinical Nephrology, 7th ed.
This is a shared conversation. Sign in to Orris to start your own chat.