Asthma
Reading File
Asking for Preferences
Finding Sources
Searching PubMed
asthma pathophysiology mechanisms
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have excellent material from multiple authoritative sources. Let me compile the comprehensive overview.
Asthma: Overview & Pathophysiology
Definition
Asthma is a chronic inflammatory disease of the airways characterized by episodic airway obstruction, airway hyperresponsiveness (AHR), and - in most cases - reversible airflow limitation. In a subset of patients, a component of the obstruction becomes irreversible over time.
"Asthma is a disease characterized by episodic airway obstruction and airway hyperresponsiveness usually accompanied by airway inflammation."
- Harrison's Principles of Internal Medicine 22E (2025), Ch. 298
Epidemiology
-
Approximately 262 million people are affected globally; prevalence in the US is ~7.9%.
-
More prevalent in children (8.4%) than adults (7.7%); in childhood, boys are affected 2:1 over girls, with this ratio reversing in adulthood.
-
Prevalence is rising, linked to urbanization (the "hygiene hypothesis").
-
In the US, Black race and Puerto Rican ethnicity carry higher prevalence and morbidity.
-
Asthma mortality has declined since the 1990s, largely attributed to wider use of inhaled corticosteroids (ICS).
-
Harrison's Principles of Internal Medicine 22E, Ch. 298
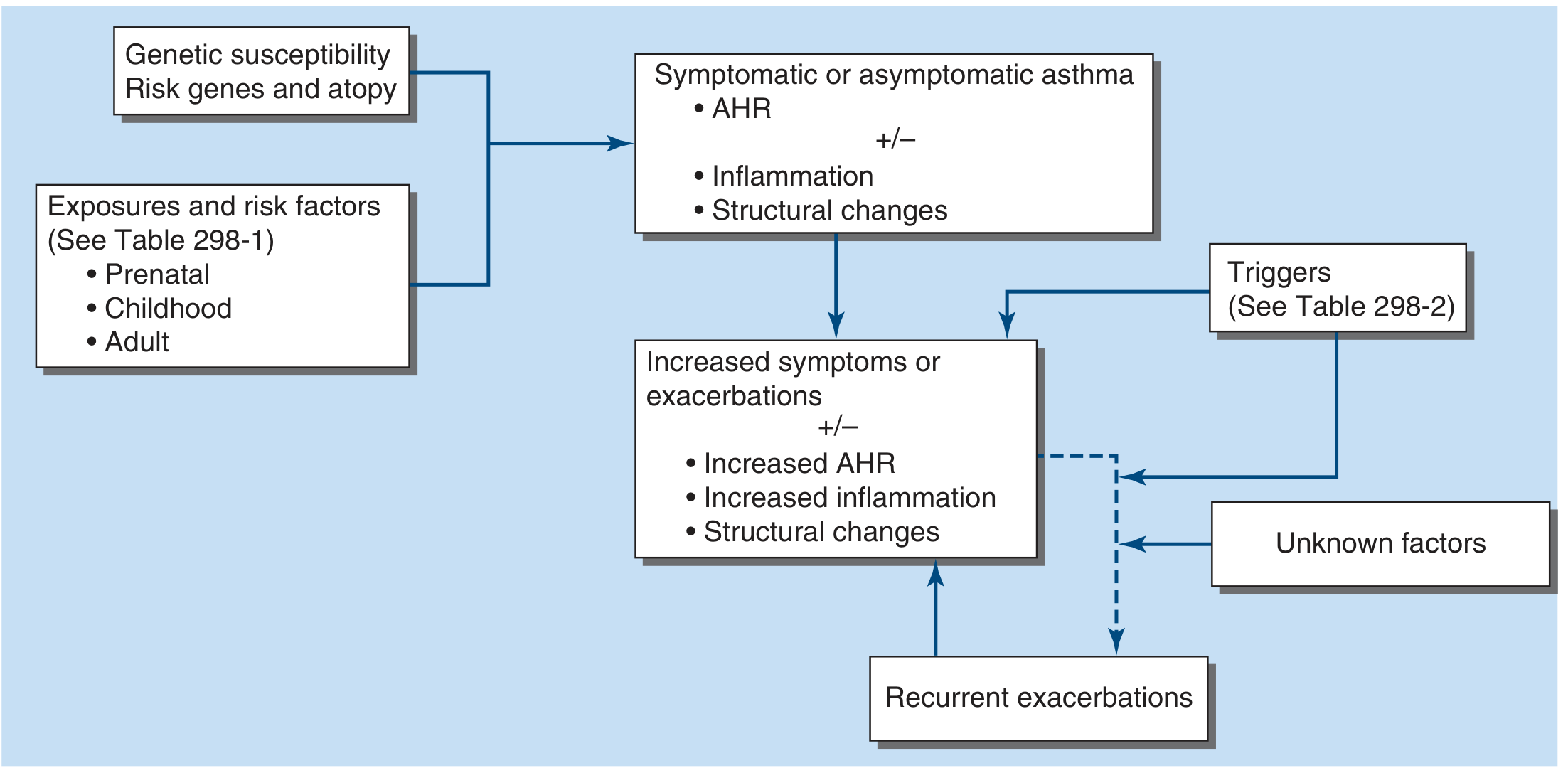
The Asthma Development Pathway
The development of asthma results from an interaction between genetic susceptibility (risk genes, atopy) and environmental/developmental exposures across the lifespan. Once disease is established, ongoing triggers drive exacerbations and structural progression.
Key risk factors for developing asthma:
- Allergen exposure in atopic individuals
- Occupational exposures
- Air pollution & tobacco
- Viral/Mycoplasma infections
- Obesity
- Diet
- High-intensity exercise (elite athletes)
- Fungi (allergic airway mycoses)
Pathophysiology
1. The Three Core Mechanisms of Airflow Obstruction
Airflow obstruction arises from three simultaneous processes:
| Mechanism | Description |
|---|---|
| Bronchoconstriction | Smooth muscle contraction narrows the lumen |
| Airway wall inflammation and edema | Mucosal swelling further reduces lumen area |
| Excess mucus secretion | Plugs small airways and impairs clearance |
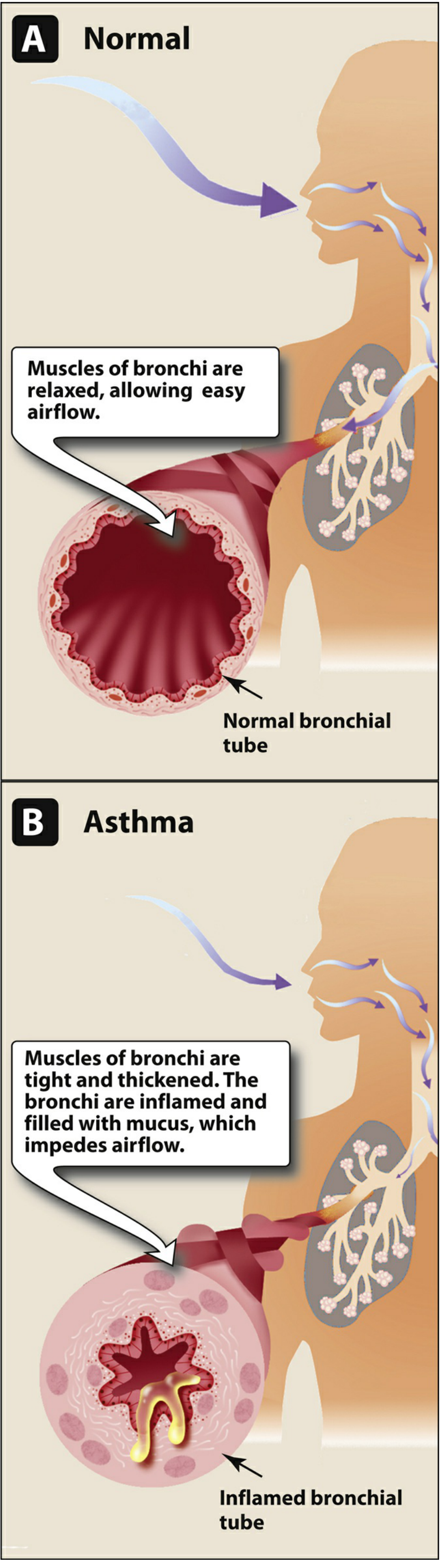
- Lippincott Illustrated Reviews: Pharmacology, Ch. 41
2. Airway Hyperresponsiveness (AHR)
AHR is the physiological hallmark of asthma - an exaggerated narrowing response to stimuli that do not affect normal airways. It arises from two sources:
- Direct smooth muscle hyperresponsiveness - the muscle itself contracts excessively (demonstrable with histamine or methacholine challenge)
- Indirect hyperresponsiveness - stimulation of inflammatory cells releases direct bronchoconstrictors (histamine, leukotrienes, prostaglandins) and sensory nerve activation further amplifies smooth muscle contraction
- Structural contribution - thickened airway walls (from hypertrophy, fibrosis, edema) mean that any given degree of muscle contraction produces disproportionately greater luminal narrowing
"A major therapeutic objective in asthma is to decrease the degree of airway hyperresponsiveness."
- Harrison's, Ch. 298
3. Inflammatory Cells and Mediators
Asthma is driven by a type 2 (T2) immune response, orchestrated by:
| Cell Type | Role |
|---|---|
| Th2 lymphocytes | Drive eosinophilic inflammation; produce IL-4, IL-5, IL-13 |
| ILC2s (innate type 2 lymphocytes) | Amplify type 2 inflammation independently of allergen sensitization |
| Mast cells | Activated by allergens (via IgE) and physical stimuli; release histamine, LTD4, PGD2 causing immediate bronchoconstriction |
| Eosinophils | Main effector cells in chronic airway inflammation; present in most asthmatics |
| Dendritic cells | Orchestrate Th2 polarization; regulate IgE production by B cells |
| Neutrophils | Predominant in severe/refractory asthma and T2-low phenotype |
Key mediators released:
- Histamine - immediate bronchoconstriction, vasodilation, mucosal edema
- Leukotrienes (LTC4, LTD4, LTE4) - potent bronchoconstrictors; also increase mucus secretion
- Prostaglandin D2 (PGD2) - bronchoconstriction, eosinophil recruitment
- IL-4, IL-13 - promote IgE synthesis, airway mucus production, smooth muscle hypertrophy
- IL-5 - eosinophil survival and recruitment
"Mast cell activation by allergens and physical stimuli releases bronchoconstrictor mediators, such as histamine, leukotriene D4 and prostaglandin D3, which cause airway smooth muscle contraction, vasodilation, microvascular leakage, and plasma exudation."
- Goodman & Gilman's Pharmacological Basis of Therapeutics, Ch. 44
4. Airway Remodeling
Prolonged or untreated inflammation leads to structural changes (remodeling) that partially explain irreversible obstruction in some patients:
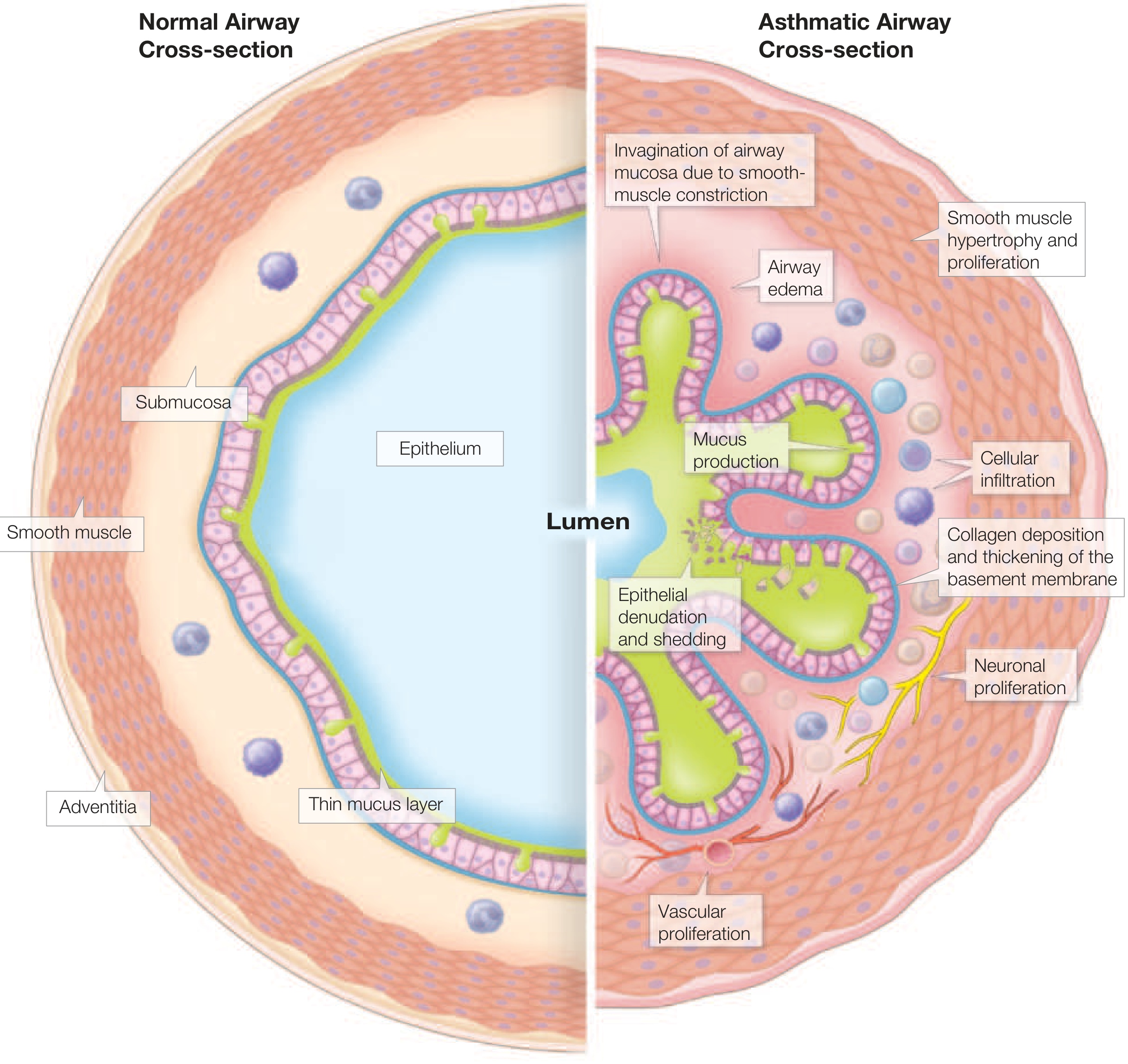
The diagram above shows the key structural changes:
- Smooth muscle hypertrophy and hyperplasia - thickens the wall, increases contractile mass
- Subepithelial collagen/matrix deposition - repair-type collagens (tenascin, periostin, fibronectin, osteopontin) deposited by myofibroblasts; stiffens airways and reduces capacity to dilate
- Epithelial denudation and shedding - exposes sensory nerve endings, increasing responsiveness to triggers; disrupts barrier function
- Goblet cell metaplasia/hyperplasia - contributes to excess mucus
- Vascular proliferation (angiogenesis) - contributes to edema and airway wall thickening
- Neuronal proliferation - amplifies bronchoconstrictor neural signals
"If untreated, asthma may cause airway remodeling, resulting in increased severity and incidence of asthma exacerbations and/or death."
- Lippincott Pharmacology, Ch. 41
5. Common Triggers
| Category | Examples |
|---|---|
| Allergens | Dust mites, pollen, animal dander, moulds |
| Irritants | Smoke, strong odours, chemicals |
| Infections | Rhinovirus (most common), RSV, Mycoplasma |
| Physical | Exercise, cold/dry air |
| Drugs | Aspirin/NSAIDs, beta-blockers |
| Environmental | Air pollution, occupational agents |
| Hormonal | Pregnancy, menstrual cycle changes |
| Other | Emotional stress, gastro-oesophageal reflux |
6. Asthma Phenotypes
Modern understanding recognises distinct biological phenotypes (endotypes):
| Phenotype | Key Features |
|---|---|
| Allergic (T2-high) | Atopic; IgE-mediated; eosinophilic; onset often in childhood; responds well to ICS |
| Eosinophilic non-allergic (T2-high) | Adult-onset; non-atopic but eosinophilic; driven by ILC2s and cytokines |
| T2-low (neutrophilic/paucigranulocytic) | Severe; often associated with obesity, smoking, or infections; less responsive to corticosteroids |
| Mixed (eosinophilic + neutrophilic) | Most severe phenotype |
- Murray & Nadel's Textbook of Respiratory Medicine; Harrison's Ch. 298
Clinical Manifestations
Classic presenting symptoms:
- Episodic dyspnoea (shortness of breath)
- Wheeze (polyphonic, usually expiratory)
- Cough (often nocturnal or early morning)
- Chest tightness
- Mucus production
Symptoms may resolve spontaneously or with treatment. Airway obstruction is most severe during expiration because dynamic compression worsens during forced exhalation. Severe episodes (exacerbations) may require emergency care and can be fatal.
Summary Diagram
The full picture of asthma can be summarized as a self-reinforcing cycle:
Trigger exposure → Mast cell activation & Th2/ILC2 response → Acute bronchoconstriction + edema + mucus (symptoms) → Chronic eosinophilic inflammation → Airway remodeling → greater AHR → easier triggering → cycle continues
Sources: Harrison's Principles of Internal Medicine 22E (2025) Ch. 298; Goodman & Gilman's Pharmacological Basis of Therapeutics Ch. 44; Lippincott Illustrated Reviews: Pharmacology Ch. 41; Murray & Nadel's Textbook of Respiratory Medicine
This is a shared conversation. Sign in to Orris to start your own chat.