Stroboscopy in detail for 20 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
Finding Sources
Finding Sources
Searching PubMed
laryngeal stroboscopy voice assessment
Searching the Web
stroboscopy laryngoscopy ENT RGUHS 20 marks recent advances vocal cord
Reading File
Reading File
Finding Sources
Reading Web Page
https://pmc.ncbi.nlm.nih.gov/articles/PMC3747974
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Searching PubMed
high speed videoendoscopy stroboscopy vocal fold comparison
STROBOSCOPY - 20 MARKS (RGUHS)
Sources: Cummings Otolaryngology (7th Ed), Scott-Brown's Otorhinolaryngology HNS (8th Ed), K.J. Lee's Essential Otolaryngology, PMC/NIH - Mehta & Hillman 2013
1. DEFINITION AND HISTORICAL BACKGROUND
Stroboscopy (laryngeal videostroboscopy / LVS) is an optical technique that uses a xenon-flash strobe light synchronized to the fundamental frequency of vocal fold vibration to create an apparent slow-motion illusion of vocal fold movement, allowing visualization of mucosal vibration patterns that are otherwise invisible to the naked eye.
- First described by Oertel (1878) using a dental mirror and rotating disc
- Modern videostroboscopy became standard clinical practice in the 1980s-90s
- Currently the gold standard for evaluating vocal fold vibratory pathology
(Cummings Otolaryngology, Ch. 58; Scott-Brown's, Ch. 61)
2. PHYSICAL PRINCIPLE - TALBOT'S LAW
The entire principle of stroboscopy rests on Talbot's Law of Retinal Persistence:
┌─────────────────────────────────────────────────────────────┐
│ TALBOT'S LAW (Retinal Persistence) │
│ │
│ The human retina retains an image for 1/5th of a second │
│ (0.2 seconds) = can only resolve 5 images per second │
│ │
│ Vocal folds vibrate at 75–1000 Hz │
│ (75 to 1000 cycles/second) │
│ │
│ ∴ Vocal fold vibration is INVISIBLE to the naked eye │
└─────────────────────────────────────────────────────────────┘
The Stroboscopic Solution:
┌──────────────────────────────────────────────────────────────────┐
│ STROBOSCOPIC PRINCIPLE │
│ │
│ Microphone detects fundamental │
│ frequency (F0) of patient's voice │
│ ↓ │
│ Stroboscope fires xenon flash at │
│ rate SLIGHTLY different from F0 │
│ (flash duration: 1/1000 second) │
│ ↓ │
│ Each flash samples vocal folds at │
│ a DIFFERENT phase of the vibratory cycle │
│ ↓ │
│ Brain fuses successive images (retinal persistence) │
│ ↓ │
│ Creates APPARENT SLOW-MOTION of vocal fold vibration │
└──────────────────────────────────────────────────────────────────┘
Two operating modes:
| Mode | Mechanism | Result |
|---|---|---|
| Slow-motion mode | Flash rate slightly out of phase with F0 (offset by ~0.5-2 Hz) | Apparent slow-motion vibration |
| Frozen/stop mode | Flash rate exactly synchronized with F0 | Vocal folds appear stationary |
(Cummings Otolaryngology, Block 12, p.1076)
3. EQUIPMENT / COMPONENTS
┌─────────────────────────────────────────────────────────────────┐
│ STROBOSCOPY SYSTEM COMPONENTS │
│ │
│ 1. LIGHT SOURCE │
│ • Xenon lamp (KayPENTAX: 5 microsecond flash duration) │
│ • OR LED-based (ATMOS system) │
│ • OR electronic shutter on continuous light (JEDMED) │
│ │
│ 2. FREQUENCY DETECTION │
│ • Contact microphone (on patient's neck) │
│ • OR Electroglottograph (EGG) │
│ │
│ 3. ENDOSCOPE (choice depends on clinical need) │
│ • Rigid 70° or 90° Hopkins rod (better resolution) │
│ • Flexible fiberoptic/chip-tip (for connected speech) │
│ │
│ 4. CAMERA (standard or HD digital/4K) │
│ │
│ 5. MONITOR + DIGITAL RECORDING UNIT │
│ │
│ 6. PRINTER / ARCHIVAL SOFTWARE │
└─────────────────────────────────────────────────────────────────┘
Rigid vs. Flexible Endoscope for Stroboscopy:
| Feature | Rigid (70°/90°) | Flexible |
|---|---|---|
| Image resolution | Excellent | Good (chip-tip better than fiberoptic) |
| Phonation tasks | Sustained vowels only | Connected speech, running speech |
| Topical anesthesia | Not usually required | Required |
| Patient comfort | Less | More tolerable |
| Tongue protrusion | Required | Not required |
| Preferred for | Voice clinic, detailed mucosal assessment | Dysphonia in connected speech, pediatric |
(Cummings, Block 11; Scott-Brown's Ch. 61)
4. VOCAL FOLD VIBRATION PHYSIOLOGY (Basis for Interpretation)
Understanding the body-cover model (Hirano, 1974) is essential:
┌──────────────────────────────────────────────────────────────┐
│ VOCAL FOLD BODY-COVER MODEL │
│ │
│ COVER: Epithelium + Superficial Lamina Propria (SLP) │
│ (pliable, responsible for mucosal wave) │
│ │
│ TRANSITION: Intermediate + Deep Lamina Propria │
│ (vocal ligament) │
│ │
│ BODY: Thyroarytenoid (vocalis) muscle │
│ (stiffer, sets tension) │
│ │
│ VIBRATION occurs via aerodynamic-myoelastic mechanism: │
│ Bernoulli effect + mucosal elasticity drive oscillation │
└──────────────────────────────────────────────────────────────┘
Phases of one vibratory cycle (visible on stroboscopy):
A-Closed phase B-Opening phase C-Open phase D-Closing phase
┌─────────────┐ ┌─────────────┐ ┌─────────────┐ ┌─────────────┐
│ ▓▓▓▓▓▓▓▓ │ │ ▓▓┐ ┌▓▓ │ │ ▓▓ ▓▓ │ │ ▓▓┐ ┌▓▓ │
│ ▓▓▓▓▓▓▓▓ │ ─────► │ ▓▓│ │▓▓ │ ─────► │ ▓▓ ▓▓ │ ─────► │ ▓▓│ │▓▓ │
│ (glottis │ │ (inferior │ │ (glottis │ │ (superior │
│ closed) │ │ lips open) │ │ open) │ │ lips close)│
└─────────────┘ └─────────────┘ └─────────────┘ └─────────────┘
↑ ↑ ↑ ↑
Subglottic Lower lip leads Max lateral Upper lip leads
pressure builds upper lip excursion closure
The diagram above (from Cummings/Hirano & Bless 1993) shows the frontal section (left) and top-down view (right) through phases A-J of a complete vibratory cycle.
5. DIAGRAM: VOCAL FOLD VIBRATION PHASES
The following is the actual textbook diagram from Cummings Otolaryngology (Fig. 58.5), showing vocal fold vibration in frontal section (left column) and from above (right column):
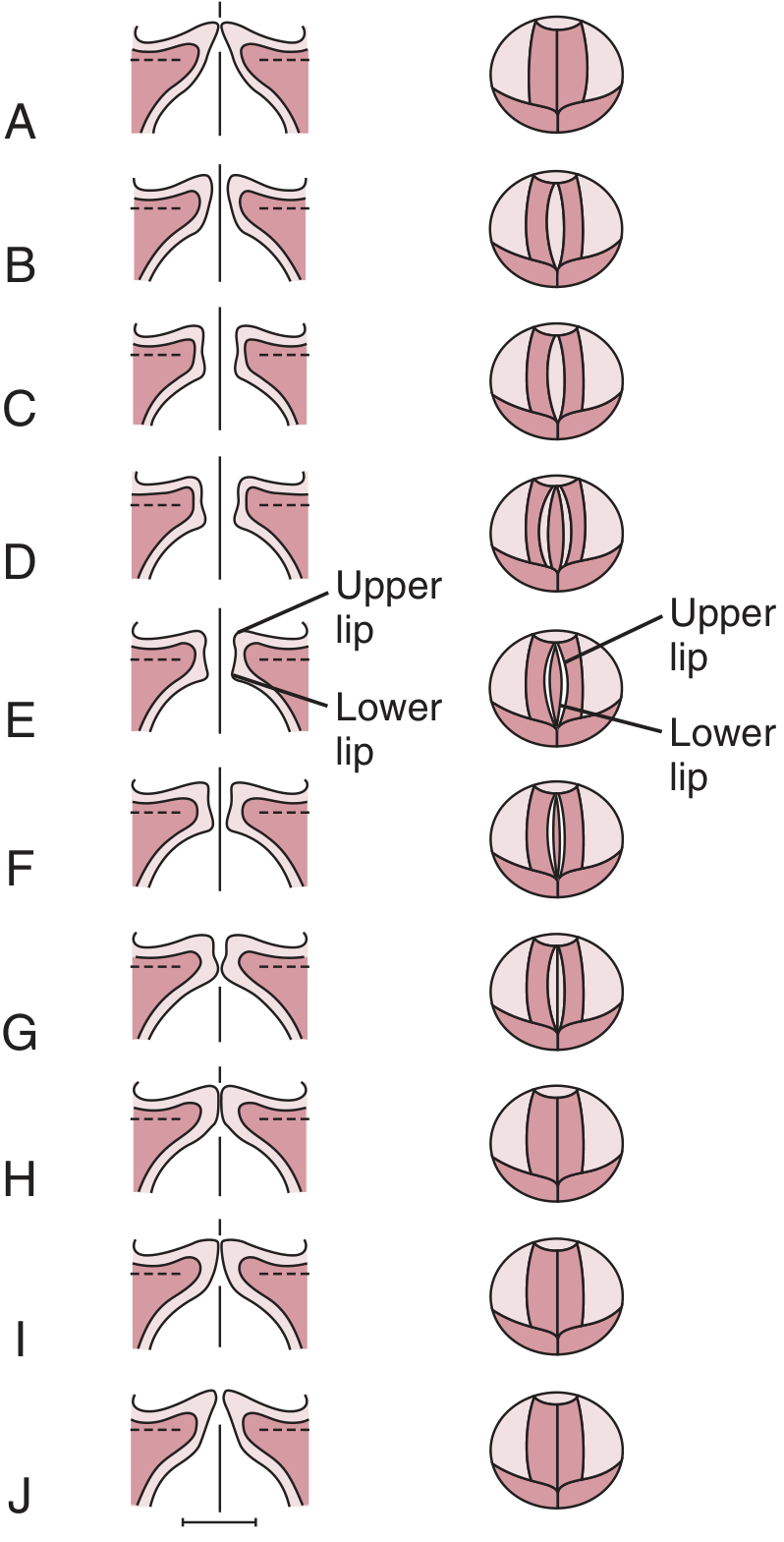
Fig. 58.5 - Cummings Otolaryngology: Vocal fold vibration. Frontal section (left) and view from above (right). Panels A-J show successive phases of one complete vibratory cycle, demonstrating the vertical phase difference between upper (superior) and lower (inferior) lips of the vocal fold.
6. PARAMETERS ASSESSED ON STROBOSCOPY
This is the core examinable content - six standard parameters (Hirano & Bless checklist; Sataloff's criteria):
┌────────────────────────────────────────────────────────────────────┐
│ STROBOSCOPIC PARAMETERS FOR ASSESSMENT │
│ (Standardized Checklist) │
│ │
│ 1. SYMMETRY 5. MUCOSAL WAVE │
│ 2. AMPLITUDE 6. GLOTTAL CLOSURE │
│ 3. PERIODICITY (+ Non-Vibrating Segment if applicable) │
│ 4. VERTICAL PHASE │
└────────────────────────────────────────────────────────────────────┘
6.1 Symmetry
- Refers to whether both vocal folds are mirror images of each other
- Normal: symmetrical, in-phase
- Abnormal: asymmetry of phase, amplitude, or mucosal wave
- Caused by differences in: mass, tension, pliability, position, or inflammation
6.2 Amplitude of Vibration
- Lateral excursion of the midmembranous portion during vibration
- Normal: 1/3 to 1/2 of the width of the visible fold
- Affected by: pitch (high pitch → reduced amplitude), intensity, lesions
- Decreased amplitude = stiffness, scar, mass lesion
6.3 Periodicity (Regularity)
- Assessed in freeze mode: synchronize flash to F0 → folds appear still
- Any perceived motion = aperiodicity
- Described as: completely periodic, mostly periodic, mostly aperiodic, completely aperiodic
- Aperiodicity = rough voice quality, pathological vibration
6.4 Mucosal Wave
- Most diagnostically important parameter
- Has two components:
- Vertical phase (medial surface): visualized as upper/lower lip separation; vertical phase difference = time lag between closure of lower lip vs. upper lip
- Horizontal phase (superior surface): "ripple of light across the superior surface" of the vocal fold - a wave traveling medial to lateral
- Normal mucosal wave: present, symmetric, traveling from inferior to superior and medial to lateral
- Stiff/scarred fold: mucosal wave absent or greatly reduced
- Lesions in SLP: wave reduced but may persist
- Lesions infiltrating the vocal ligament: wave absent
6.5 Glottal Closure Patterns
┌─────────────────────────────────────────────────────────┐
│ GLOTTAL CLOSURE PATTERNS ON STROBOSCOPY │
│ │
│ COMPLETE ────────────── (Normal in men) │
│ │
│ SMALL POSTERIOR GAP ─── (Normal in up to 70% of women)│
│ ↑ Gap at cartilaginous glottis only = NORMAL │
│ │
│ LARGE POSTERIOR GAP │
│ SLIT PATTERN ─────────── (Bowing, presbylaryngis) │
│ ELLIPTIC ─────────────── (Bilateral bowing) │
│ HOURGLASS ────────────── (Bilateral nodules) │
│ ASYMMETRIC HOURGLASS ─── (Unilateral lesion) │
│ IRREGULAR ─────────────── (Scar, cancer) │
│ │
│ Most efficient glottal output: folds ~1 mm apart │
│ at vocal process (Berry et al.) │
└─────────────────────────────────────────────────────────┘
6.6 Non-Vibrating Segment
- A region of complete adynamic (non-vibrating) tissue
- Indicates: scar, sulcus vocalis, infiltrating malignancy, or fibrous lesion
- Location noted (anterior, middle, posterior third)
7. INDICATIONS FOR STROBOSCOPY
┌────────────────────────────────────────────────────────────┐
│ INDICATIONS FOR STROBOSCOPY │
│ │
│ PRIMARY INDICATIONS: │
│ • Dysphonia / hoarseness (all cases) │
│ • Professional voice users (baseline + follow-up) │
│ • Subtle vocal fold lesions not clearly visible on WLE* │
│ • Pre- and post-phonosurgery evaluation │
│ • Sulcus vocalis / vocal fold scar │
│ • Vocal fold paresis / paralysis │
│ • Early glottic malignancy screening │
│ • Muscle tension dysphonia assessment │
│ │
│ SPECIFIC VALUE: │
│ • Changes diagnosis in 30-47% of patients vs WLE alone │
│ • Adds detail to existing diagnosis in additional 32% │
│ *(WLE = white light endoscopy) │
└────────────────────────────────────────────────────────────┘
(Cummings, Block 11 - "Assessment with Stroboscopy")
8. FLOWCHART: CLINICAL APPROACH TO STROBOSCOPY
PATIENT WITH DYSPHONIA
│
▼
┌────────────────────────┐
│ History + Physical │
│ Examination │
└──────────┬─────────────┘
│
▼
┌────────────────────────┐
│ White Light Endoscopy │
│ (Continuous light) │
│ - Structure │
│ - Gross movement │
│ - Arytenoid motion │
│ - Vascularity, mucus │
└──────────┬─────────────┘
│
┌───────────┴────────────┐
│ │
┌─────────▼──────┐ ┌──────────▼──────────┐
│ Gross lesion │ │ Subtle/no lesion, │
│ clearly visible │ │ mucosal pathology │
│ (cancer, polyp) │ │ suspected │
└─────────┬──────┘ └──────────┬──────────┘
│ │
│ ┌─────────▼──────────┐
│ │ STROBOSCOPY │
│ │ (assess vibration) │
│ └─────────┬──────────┘
│ │
│ ┌──────────────┼──────────────┐
│ ▼ ▼ ▼
│ Symmetry + Mucosal wave Glottal closure
│ Amplitude assessment pattern
│ │ │ │
│ └──────────────┼───────────────┘
│ │
│ ┌─────────▼──────────┐
│ │ DIAGNOSIS & │
│ │ DOCUMENTATION │
│ └─────────┬──────────┘
│ │
└────────────────────────┘
│
┌────────────────────┼───────────────────┐
▼ ▼ ▼
Voice Therapy Phonosurgery Observation /
(if functional) (if structural) Interval exam
9. CLINICAL FINDINGS ON STROBOSCOPY IN SPECIFIC CONDITIONS
| Condition | Symmetry | Amplitude | Mucosal Wave | Closure | Periodicity |
|---|---|---|---|---|---|
| Normal | Symmetric | Normal (1/3-1/2) | Present, symmetric | Complete / small post. gap | Regular |
| Vocal nodules | Symmetric | Decreased | Decreased at lesion; present elsewhere | Hourglass | Regular |
| Vocal polyp | Asymmetric | Asymmetric | Disrupted at lesion | Asymmetric hourglass | Irregular |
| Vocal fold cyst | Asymmetric | Decreased unilateral | Absent over cyst | Incomplete | Variable |
| Sulcus vocalis | Asymmetric | Markedly decreased | Absent or minimal | Incomplete (slit) | Irregular |
| Reinke's edema | Asymmetric | Increased | Increased wave amplitude | Variable | Irregular |
| Glottic carcinoma | Asymmetric | Absent unilateral | Absent over tumor | Incomplete | Aperiodic |
| Vocal fold paralysis | Asymmetric | Absent on paralyzed side | Absent paralyzed side | Incomplete (lateral gap) | Aperiodic |
| Muscle tension dysphonia | Symmetric | Decreased | Present but reduced | Compressed / excess | Regular |
| Vocal fold scar | Asymmetric | Markedly reduced | Absent | Incomplete | Irregular |
(Cummings Otolaryngology; Scott-Brown's, Ch. 61; K.J. Lee's Essential Otolaryngology)
10. TECHNIQUE OF EXAMINATION
Step-by-step Protocol (Cummings / Sataloff):
┌─────────────────────────────────────────────────────────────┐
│ STROBOSCOPY EXAMINATION PROTOCOL │
│ │
│ PREPARATION: │
│ 1. Detailed history - voice complaint, duration, usage │
│ 2. Perceptual voice assessment (GRBAS scale) │
│ 3. Equipment check - calibrate microphone/strobe │
│ │
│ PATIENT POSITION: │
│ Rigid: Lean slightly forward, chin up, tongue out │
│ Flexible: Seated upright, no tongue protrusion needed │
│ │
│ EXAMINATION SEQUENCE: │
│ Step 1: White light endoscopy first │
│ - Anatomy, lesions, arytenoid motion │
│ Step 2: Switch to STROBOSCOPY mode │
│ Step 3: Patient phonates sustained /ee/ (rigid) │
│ or running speech (flexible) │
│ Step 4: Assess at MULTIPLE pitches: │
│ - Modal register (habitual speaking pitch) │
│ - High pitch │
│ - Low pitch │
│ - Falsetto (if appropriate) │
│ Step 5: Assess at DIFFERENT intensities │
│ Step 6: Freeze mode to assess periodicity │
│ Step 7: Record and document findings systematically │
└─────────────────────────────────────────────────────────────┘
Why multiple pitches? At high pitch, the cover thins 3-dimensionally (cricothyroid tension), reducing the vertical phase difference. Small lesions or stiffness that are invisible at modal pitch become apparent at elevated pitch - critical in professional voice patients. (Cummings, p.1077)
11. STROBOSCOPY INTERPRETATION CHECKLIST
(Modified from Hirano & Bless, 1993 - Standardized format as used in Cummings Table 58.1)
┌───────────────────────────────────────────────────────┐
│ LARYNGOSTROBOSCOPY INTERPRETATION │
│ CHECKLIST │
├─────────────────────┬─────────────────────────────────┤
│ PARAMETER │ FINDINGS │
├─────────────────────┼─────────────────────────────────┤
│ Symmetry │ Normal / Side-to-side │
│ │ Teeter-totter / Vertical │
│ │ R>L / L>R │
├─────────────────────┼─────────────────────────────────┤
│ Amplitude (R & L) │ Normal / Decreased / Increased │
│ │ Consistent / Inconsistent │
├─────────────────────┼─────────────────────────────────┤
│ Periodicity │ Regular / Irregular │
│ │ Periodic / Aperiodic │
├─────────────────────┼─────────────────────────────────┤
│ Mucosal Wave (R&L) │ Normal / Decreased / Absent │
│ │ Abnormal pattern │
│ │ Adynamic segment (location) │
├─────────────────────┼─────────────────────────────────┤
│ Glottal Closure │ Complete / Slit / Elliptic │
│ │ Hourglass / Asymmetric │
│ │ Small/Large posterior gap │
├─────────────────────┼─────────────────────────────────┤
│ Supraglottic │ None / Antero-posterior squeeze │
│ Activity │ Lateral compression │
│ │ Complete compression (all 3) │
├─────────────────────┼─────────────────────────────────┤
│ Vertical Phase │ Present / Absent / Reduced │
├─────────────────────┼─────────────────────────────────┤
│ Image Quality │ 1 (poor) to 4 (excellent) │
│ Verbal Diagnosis │ │
└─────────────────────┴─────────────────────────────────┘
12. LIMITATIONS OF STROBOSCOPY
┌─────────────────────────────────────────────────────────────┐
│ LIMITATIONS OF STROBOSCOPY │
│ │
│ TECHNICAL LIMITATIONS: │
│ • Requires a periodic (regular) voice signal │
│ - Cannot assess aperiodic/severely dysphonic voices │
│ - Cannot work if F0 cannot be detected │
│ • Captures only ONE PHASE per cycle (sampling artifact) │
│ - True mucosal wave details may be missed │
│ • Images are a composite across multiple cycles │
│ - Cycle-to-cycle variation is averaged out │
│ • Cannot visualize pharyngeal motion or abduction │
│ │
│ CLINICAL LIMITATIONS: │
│ • Subjective interpretation │
│ • Poor intra-rater and inter-rater reliability │
│ • Cannot determine depth of invasion in malignancy │
│ (Colden et al.) │
│ • Not useful for pediatric patients (gag reflex, rigid) │
│ • Limited in patients with severe aphonia │
│ (~63% of aperiodic patients unstroboscopable) │
│ (Patel et al.) │
└─────────────────────────────────────────────────────────────┘
(Cummings, Block 12, p.1078; Block 11)
13. FLOWCHART: STROBOSCOPY FINDINGS AND MANAGEMENT
STROBOSCOPY FINDINGS
│
┌───────────────┼────────────────┐
▼ ▼ ▼
MUCOSAL WAVE GLOTTAL PERIODICITY
ABNORMALITY CLOSURE APERIODIC
│ DEFECT │
│ │ │
┌────▼────┐ ┌──────▼──────┐ ┌──────▼────────┐
│Absent / │ │ Incomplete │ │ Asymmetric │
│Reduced │ │ closure │ │ vibration │
│mucosal │ │ │ │ │
│wave │ └──────┬──────┘ └──────┬────────┘
└────┬─────┘ │ │
│ │ │
┌────▼──────────┐ ┌──▼──────────┐ ┌───▼──────────┐
│• Stiffness │ │• Bowing │ │• Paralysis │
│• Scar │ │• Atrophy │ │• Paresis │
│• Sulcus │ │• Paralysis │ │• Scar │
│• Infiltrating │ │• Nodules │ │• Mass │
│ malignancy │ │ (hourglass)│ │ asymmetry │
└───────────────┘ └─────────────┘ └──────────────┘
│ │ │
▼ ▼ ▼
Voice therapy Injection Phonosurgery
Fat injection augmentation (LEMM/MLT)
Phonosurgery (medialization) EMG / NLR
(LEMM, grafts) or thyroplasty
14. ROLE IN PROFESSIONAL VOICE USERS (Scott-Brown's / Sataloff)
- Mandatory investigation in all professional voice users (singers, actors, teachers, lawyers)
- Scott-Brown's explicitly states: "Stroboscopy (either rigid or via a chip-tip endoscope) is mandatory in the vocal professional. Video archiving is imperative."
- A baseline stroboscopy when the voice is healthy allows comparison during dysphonic episodes
- Interval stroboscopy tracks effects of behavioral, medical, and surgical interventions
- Detects subtle lesions (hemorrhage, early sulcus, early polyp) missed by white light alone
- Documents recovery trajectory post-phonosurgery
15. ELECTROGLOTTOGRAPHY (EGG) - Complementary Investigation
- Low-voltage, high-frequency current passed between two electrodes on the sides of the thyroid cartilage
- Records the opening and closing rates of the vocal folds (not visualized well on stroboscopy)
- Provides: F0, open quotient, speed quotient
- Helps synchronize stroboscopic flash more accurately
(Cummings, Block 12 - "Electroglottography")
16. RECENT ADVANCES IN STROBOSCOPY (2013-2026)
A. High-Definition (HD) and 4K Stroboscopy
- KayPENTAX HD system: 1920 × 1080 pixels vs standard 720 × 480
- Significant improvement in mucosal surface detail, vasculature visualization
- Expected to enhance diagnostic capability for subtle lesions, vascularity
B. Chip-on-Tip (Distal Chip) Flexible Endoscopes
- CCD sensor at the tip (vs. glass fiber bundles in fiberoptic scopes)
- Near-equivalent resolution to rigid scopes
- Allows stroboscopy during running speech - superior for MTD and functional dysphonia
- Scott-Brown's recommends chip-tip for professional voice assessment
C. High-Speed Videoendoscopy (HSV/LHSV)
- Records 2,000-10,000 frames per second (vs stroboscopy's composite sampling)
- Captures true cycle-by-cycle variation
- Works even in aperiodic/severely dysphonic voices where stroboscopy fails
- Limitation: Large data files, no real-time audio-visual feedback, expensive
- Current status: Research instrument - future clinical tool (Cummings; PMC3747974)
┌────────────────────────────────────────────────────────────────┐
│ STROBOSCOPY vs HIGH-SPEED VIDEOENDOSCOPY │
│ │
│ Feature Stroboscopy HSV │
│ ───────────────────────────────────────────────── │
│ Frame rate Composite 2,000-10,000 fps │
│ Periodic voices ✓ Excellent ✓ Excellent │
│ Aperiodic voices ✗ Failed (63%) ✓ Works always │
│ Cycle-to-cycle data ✗ Averaged ✓ Complete │
│ Real-time review ✓ ✗ Post-processing │
│ Cost Moderate High │
│ Clinical standard Gold standard Research tool │
└────────────────────────────────────────────────────────────────┘
(Cummings Otolaryngology, Block 11, "Laryngeal High-Speed Videoendoscopy"; Mehta & Hillman, Current Role of Stroboscopy in Laryngeal Imaging, Curr Opin Otolaryngol HNS, 2013)
D. Narrow-Band Imaging (NBI)
- Uses blue (415 nm) and green (540 nm) light - absorbed by hemoglobin
- Highlights surface vasculature without dye
- Useful for: Identifying abnormal vessels in recurrent papillomatosis, screening for malignancy, guiding biopsy
- Can be combined with stroboscopy in same examination session
E. Simulated Stroboscopy from HSV (kymographic reconstruction)
- Kymography extracted from HSV data can simulate stroboscopy images
- Studies show simulated stroboscopy has fewer asynchronous sequences and better inter-rater reliability than acoustic-based LVES (Cummings, Block 11)
F. Optical Coherence Tomography (OCT)
- Cross-sectional microstructural imaging of vocal fold layers
- Can differentiate epithelium from SLP, identify sub-surface lesions and scar
- Emerging research tool for phonosurgery planning
G. mHealth and Telemedicine
- Smartphone-attached laryngoscopes and portable stroboscopy units
- App-based voice analysis as adjunct
- Scoping review (du Toit et al., J Voice 2026, PMID: 41881756) documents growing role of mobile technologies in voice disorder assessment
H. AI/Machine Learning for Stroboscopy Analysis
- Automated parameter extraction (mucosal wave amplitude, symmetry, closure)
- Reducing inter-rater variability
- Early detection of subtle pre-malignant changes
17. STROBOSCOPY IN SPECIFIC RGUHS-RELEVANT CONTEXTS
Sulcus Vocalis (Medically important to RGUHS)
- Stroboscopy shows: absent/markedly reduced mucosal wave, slit closure, adynamic segment
- Often missed on white-light endoscopy alone
- Stroboscopy is the only modality that reliably diagnoses sulcus vocalis pre-operatively
Glottic Carcinoma
- Stroboscopy demonstrates absence of mucosal wave over the tumor (infiltration)
- Limitation: Stroboscopy cannot determine depth of invasion or distinguish atypia from invasive cancer (Colden et al.) - confirmed by Cummings
- Therefore, stroboscopy is NOT a substitute for biopsy in suspected malignancy
18. SUMMARY TABLE FOR QUICK REVISION (20 Marks)
| Topic | Key Fact |
|---|---|
| Inventor | Oertel, 1878 |
| Principle | Talbot's law - retinal persistence (5 images/sec max) |
| Light source | Xenon flash (1/1000 s duration) |
| F0 detection | Contact microphone or EGG |
| Standard parameters | Symmetry, Amplitude, Periodicity, Mucosal wave, Closure, Vertical phase |
| Mucosal wave | Most diagnostically important parameter |
| Normal amplitude | 1/3 to 1/2 of visible fold width |
| Normal closure | Complete (men); small posterior gap (up to 70% of women) |
| Key indication | Dysphonia, professional voice users, pre/post phonosurgery |
| Diagnostic advantage | Changes diagnosis in 30-47% vs white light alone |
| Main limitation | Cannot assess aperiodic voices (fails in ~63%) |
| Cancer limitation | Cannot determine depth of invasion |
| Recent advance | HD stroboscopy, HSV, NBI, OCT, AI-assisted analysis |
| Complementary test | EGG (for opening/closing rates) |
| HSV status | Research instrument - complements stroboscopy |
REFERENCES
- Cummings Otolaryngology Head and Neck Surgery, 7th Ed - Chapter 54 (Videoendoscopy & Stroboscopy), Chapter 58 (Professional Voice) - Sataloff RT
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, 8th Ed - Chapter 61 (Assessment and Examination of the Larynx), Chapter 62 (Evaluation of the Voice)
- K.J. Lee's Essential Otolaryngology, 11th Ed - Vocal Fold Lesions (Stroboscopy findings)
- Hirano M, Bless DM - Videostroboscopic Examination of the Larynx, Singular Publishing Group, 1993 (the foundational text cited across all references)
- Mehta DD, Hillman RE - Current role of stroboscopy in laryngeal imaging, Curr Opin Otolaryngol Head Neck Surg. 2012; PMC3747974
- Dhingra PL - Diseases of Ear, Nose and Throat & HNS, 7th Ed - Larynx chapter (Stroboscopy under laryngeal examination)
- Hazarika P - Textbook of ENT and HNS, 3rd Ed - Laryngeal examination
- Stell & Maran's Head and Neck Surgery - Laryngoscopy and voice assessment
- Zakir Hussain - Clinical ENT - Laryngeal stroboscopy (Indian ENT reference)
- Medeiros N et al. - Surgical Treatments for Sulcus Vocalis and Vocal Fold Scar, Laryngoscope 2022 - PMID: 34057225
Note for RGUHS Exam (20 Marks): Structure your answer as: Definition + Historical note (2 marks) → Principle/Talbot's law (2 marks) → Equipment (2 marks) → Physiology of VF vibration (2 marks) → Parameters assessed (4 marks - this is the core) → Technique + Clinical applications (3 marks) → Limitations (2 marks) → Recent advances (3 marks). Include the vocal fold vibration diagram above and at least one flowchart. The mucosal wave, closure patterns, and comparison with HSV are high-yield for RGUHS. Sulcus vocalis and professional voice are common clinical application sub-questions.
This is a shared conversation. Sign in to Orris to start your own chat.