Epidemiology and prevention and risk factor and rule of halves
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Searching the Web
hypertension "rule of halves" epidemiology awareness treatment control
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive information to deliver a thorough answer on hypertension epidemiology, risk factors, prevention, and the rule of halves. Let me compile the full response.
Hypertension: Epidemiology, Risk Factors, Prevention, and the Rule of Halves
1. Epidemiology
Hypertension is the most common cardiovascular disorder and a major global public health challenge. It is the leading modifiable risk factor for coronary heart disease, stroke, heart failure, atrial fibrillation, chronic kidney disease, and dementia.
Global burden:
- An estimated 1.4 billion adults aged 30-79 years worldwide had hypertension in 2024 - approximately 33% of the population in that age group (WHO Hypertension fact sheet)
- Two-thirds of affected adults live in low- and middle-income countries
- Cardiovascular mortality attributed to hypertension accounts for 20-50% of all deaths
- One-third of all cardiovascular disease deaths could potentially be prevented with elimination of hypertension
USA data (NHANES 2021-2023):
- Prevalence: 47.7% of adults (nearly half the US adult population)
- Higher in men (50.8%) than women (44.6%)
- Increases sharply with age: 23.4% (ages 18-39), 52.5% (40-59), 71.6% (60+)
- Black Americans have the highest prevalence (~56%), rising to >75% after age 65
Blood pressure classification (ACC/AHA 2017 standard):
| Category | Systolic (mmHg) | Diastolic (mmHg) |
|---|---|---|
| Normal | <120 | and <80 |
| Elevated | 120-129 | and <80 |
| Stage I HTN | 130-139 | or 80-89 |
| Stage II HTN | ≥140 | or ≥90 |
Blood pressure in the population is distributed as a continuous bell-shaped curve with no clear threshold - cardiovascular risk rises progressively with BP (Fuster & Hurst's The Heart, 15th Ed, p. 195).
2. Risk Factors
Non-modifiable Risk Factors
(a) Age - BP rises with age in both sexes, more so in those with higher baseline BP. Some primitive societies with low salt/caloric intake show no age-related BP rise.
(b) Sex - Men have higher BP at adolescence through middle age. Post-menopause, the gap narrows and may reverse due to estrogen loss.
(c) Genetic factors - Inheritance is polygenic. Key evidence:
- Children of two normotensive parents: 3% risk of hypertension
- Children of two hypertensive parents: 45% risk
- Monozygotic twins show stronger BP correlation than dizygotic twins
- No significant correlation between adopted children and adoptive parents
(d) Ethnicity - Black populations consistently show higher BP levels than other ethnic groups (difference up to ~20 mmHg by the 6th decade).
Modifiable Risk Factors
(a) Obesity - Central obesity (increased waist-to-hip ratio) is strongly correlated with hypertension. Weight loss consistently lowers BP.
(b) High salt intake - High sodium intake (>7-8 g/day) proportionately raises BP. Reduction to <5-6 g/day lowers BP by 2-8 mmHg.
(c) Alcohol - Excessive intake raises BP. Moderation (≤2 drinks/day men, ≤1 drink/day women) reduces SBP by 2-4 mmHg.
(d) Physical inactivity - Sedentary lifestyle increases risk; regular aerobic exercise reduces SBP by 4-9 mmHg.
(e) Psychological stress - Chronic stress and certain personality traits are associated with elevated BP.
(f) Oral contraceptives - Can raise BP in susceptible women.
(g) Other - Hyperlipidaemia, diabetes, smoking (as overall cardiovascular risk amplifiers).
- Park's Textbook of Preventive and Social Medicine, pp. 425-427
3. The Rule of Halves
The Rule of Halves (originally described by Hart in the early 1970s for hypertension) is a public health concept capturing the cascading inefficiency in the detection and management of hypertension in a community. It illustrates the gap between disease burden and effective control.
Classic formulation:
Of all hypertensives in the community:
- Half are unaware (undiagnosed, asymptomatic)
- Of those who know, only half are on treatment
- Of those on treatment, only half have their BP adequately controlled
This produces an efficiency cascade:
All hypertensives (100%)
→ Only 50% aware
→ Only 50% of those treated = 25% of total
→ Only 50% of treated = 12.5% of total under control
So in the original model, only ~12.5% of all hypertensives in the community were effectively controlled.
Why this matters: Hypertension is largely a "silent" disease - it causes no symptoms until end-organ damage (stroke, MI, renal failure, retinopathy) has already occurred. The only way to detect it is active screening. The rule of halves quantifies the public health gap created by:
- Lack of screening (unaware cases)
- Poor treatment initiation (under-treated)
- Poor BP control (inadequately treated)
Current real-world data: The concept still holds, though numbers have shifted:
- WHO (2024): ~44% of hypertensives are unaware, ~44% are treated, only ~23% have BP under control
- USA (NHANES 2021-2023): 59.2% aware, ~51% on treatment, only ~21% controlled
- This confirms the "rule of halves" pattern persists globally, though the proportions vary by country and era
Significance for program evaluation: The rule of halves is used to:
- Benchmark the performance of a national hypertension control program
- Identify at which stage the gap is greatest (detection vs. treatment initiation vs. adherence)
- Guide targeted interventions (e.g., community screening vs. adherence programs)
4. Prevention of Hypertension
(Source: Park's Textbook of Preventive and Social Medicine, p. 426-427)
Primary Prevention
The goal is to prevent the onset of hypertension before it develops.
a. Population strategy - Directed at the entire community regardless of individual risk. A small downward shift in the mean BP of a population produces a large reduction in stroke and CHD incidence. Measures include:
- Dietary sodium reduction (target: ≤5 g/day)
- DASH diet (rich in fruits, vegetables, low-fat dairy; reduces SBP 8-14 mmHg)
- Weight reduction (5-20 mmHg per 10 kg lost)
- Regular physical exercise (30 min/day aerobic activity; reduces SBP 4-9 mmHg)
- Alcohol moderation
- Stress reduction, yoga, behavioural changes
- Health education and self-care (home BP monitoring)
b. High-risk strategy - Targeted at individuals with identifiable risk factors (family history, obesity, salt-sensitive subjects). Aims to prevent BP from ever reaching levels requiring pharmacological treatment. Family history and "tracking" of BP from childhood help identify high-risk individuals.
Secondary Prevention
Goal: detect and treat existing hypertension to prevent complications.
(i) Early case detection - Mass screening is the only reliable method since hypertension is asymptomatic. Screening must be linked to follow-up and treatment; isolated screening without care is a "fruitless exercise" (Park's).
(ii) Treatment - Lifestyle modifications + antihypertensive drugs. Modern pharmacotherapy effectively reduces the excess risk of stroke, MI, and renal disease.
(iii) Follow-up - Long-term adherence monitoring, complication surveillance, and BP log-books for patient self-care.
Summary Table
| Aspect | Key Points |
|---|---|
| Global prevalence | ~1.4 billion adults; ~33% aged 30-79 |
| USA prevalence | ~47.7% adults |
| Strongest non-modifiable risk | Age, genetics, ethnicity (Black) |
| Strongest modifiable risk | Obesity, high salt, physical inactivity |
| Rule of halves | 50% unaware → 50% untreated → 50% uncontrolled = only ~12.5% truly controlled |
| Primary prevention | Population + high-risk strategies; lifestyle modifications |
| Secondary prevention | Screening + treatment + sustained follow-up |
| BP reduction per intervention | Weight loss 5-20 mmHg; DASH 8-14 mmHg; Exercise 4-9 mmHg; Salt reduction 2-8 mmHg |
- Park's Textbook of Preventive and Social Medicine, pp. 425-428
- Fuster and Hurst's The Heart, 15th Ed, p. 195-200
- WHO Hypertension Fact Sheet 2025
- NCHS Data Brief, USA NHANES 2021-2023
Tracking of bp
Finding Sources
Searching the Web
blood pressure tracking childhood hypertension epidemiology concept
Reading File
Loading Image
Searching PubMed
"blood pressure tracking" childhood adulthood hypertension
I have everything needed - the textbook definition, the tracking diagram from Park's, and supporting web evidence. Here is the complete answer.
"Tracking" of Blood Pressure
Definition
Tracking is the phenomenon where an individual's blood pressure maintains its relative rank position within the population distribution over time, from childhood through to adult life.
In simple terms:
- Those with low BP in childhood tend to remain at the lower end of the distribution as adults
- Those with high BP in childhood tend to remain at the higher end - and their BP rises more steeply with age
"This phenomenon of persistence of rank order of blood pressure has been described as 'tracking'."
- Park's Textbook of Preventive and Social Medicine, p. 425
The Tracking Diagram
Each curve in this diagram represents an individual's BP trajectory over time. Notice how the curves run roughly parallel - a person who starts high stays high, and the higher curves diverge more steeply with age:
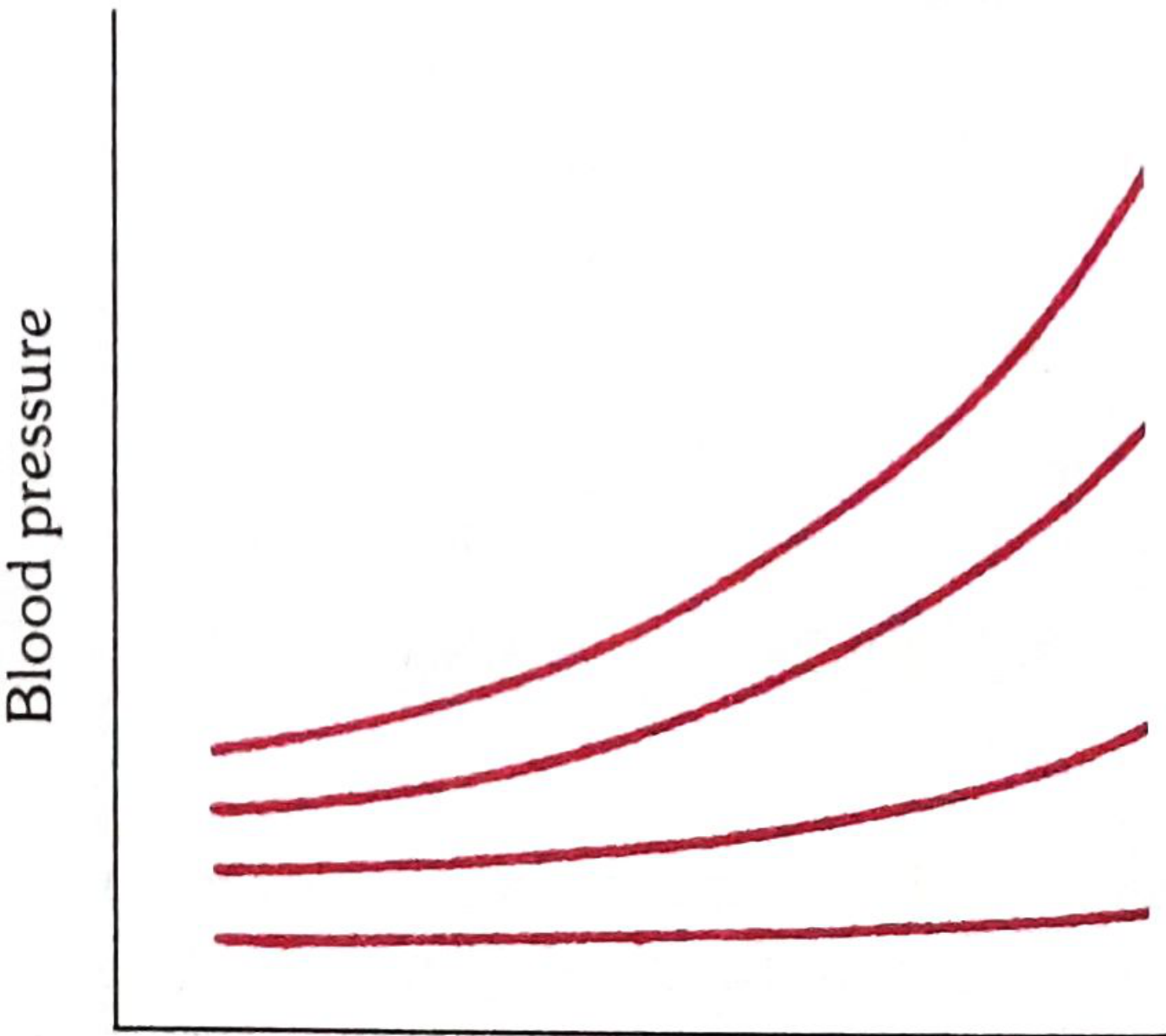
Fig: Tracking of blood pressure (Park's Textbook of Preventive and Social Medicine)
Key Features of BP Tracking
| Feature | Detail |
|---|---|
| Direction | Always positive - higher childhood BP predicts higher adult BP |
| Correlation strength | Moderate in childhood; strengthens with age and repeated measurements |
| Both components | Tracks for both systolic and diastolic BP |
| Timeframe | Observed from early childhood through adolescence into adulthood |
| Population groups | Demonstrated across multiple ethnic groups and countries |
Mechanism / Why It Occurs
Tracking reflects a combination of:
- Genetic programming - polygenic inheritance of BP regulation is set early in life
- Environmental stability - dietary habits (salt intake, calorie intake), activity levels, and obesity tend to persist within families
- Vascular remodelling - early sustained high BP leads to arterial stiffening, which then sustains and amplifies the elevation
- Neurohumoral patterns - sympathetic tone and renin-angiotensin sensitivity established in childhood tend to persist
Significance in Preventive Medicine
The concept of tracking has major implications:
1. Identifying high-risk individuals early
Family history of hypertension + a child's own BP percentile can be used to flag those at risk of adult hypertension - before it manifests. This is the basis of the high-risk strategy in hypertension prevention (Park's, p. 426).
2. Justification for childhood BP screening
Since a child in the upper BP percentiles is likely to become a hypertensive adult, routine BP measurement in children and adolescents is warranted - not just for diagnosing childhood hypertension, but for predicting and preventing adult disease.
3. Primary prevention window
The tracking concept means that intervening early (in childhood/adolescence) - through diet, weight control, physical activity - is more likely to be effective than waiting for adult hypertension to declare itself.
4. Target organ damage starts early
Research confirms that children with elevated BP show early signs of left ventricular hypertrophy and increased carotid intima-media thickness, meaning the clock on end-organ damage starts ticking in childhood. The Bogalusa Heart Study was one of the landmark studies demonstrating this.
Tracking Correlation Coefficients (Evidence)
Studies show tracking correlations are:
- Moderate in early childhood (r ≈ 0.3-0.4)
- Stronger in adolescence (r ≈ 0.5-0.6)
- Stronger still in adulthood (r ≈ 0.6-0.7)
A 2025 meta-analysis published in JAMA Pediatrics confirmed that children and adolescents with elevated BP or hypertension were over twice as likely to have elevated BP/hypertension as adults, with a 16-63% absolute probability of tracking to adult hypertension depending on severity.
Summary
The tracking concept bridges paediatric and adult medicine. It tells us that hypertension prevention must start in childhood - not at age 40 when the damage is already accumulating. Family history of hypertension and a child's current BP percentile are the two simplest tools to identify who will need the closest follow-up over their lifetime.
- Park's Textbook of Preventive and Social Medicine, p. 425
Definition of diabetes mellitus and types and obesity classification and prevention and control
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have all the material needed for a comprehensive answer. Let me compile the full response.
Diabetes Mellitus & Obesity: Definition, Types, Classification, Prevention and Control
PART 1: DIABETES MELLITUS
Definition
"The term diabetes describes a group of metabolic disorders characterized and identified by the presence of hyperglycaemia in the absence of treatment. The heterogeneous aetio-pathology includes defects in insulin secretion, insulin action, or both, and disturbances of carbohydrate, fat and protein metabolism."
- Park's Textbook of Preventive and Social Medicine, p. 443
Long-term complications include:
- Microvascular: Retinopathy, nephropathy, neuropathy
- Macrovascular: Heart disease, peripheral arterial disease, cerebrovascular disease
- Other: Cataracts, erectile dysfunction, non-alcoholic fatty liver disease, increased susceptibility to infections (especially tuberculosis)
Lower limb amputations are at least 10 times more common in diabetics than non-diabetics. Age-adjusted mortality in diabetics is 1.5 to 2.5 times higher than the general population.
WHO Classification of Diabetes (2019)
| Type | Brief Description | Key Feature |
|---|---|---|
| Type 1 diabetes | Beta-cell destruction (mostly immune-mediated); absolute insulin deficiency | Onset in childhood/early adulthood; requires insulin |
| Type 2 diabetes | Most common; varying degrees of beta-cell dysfunction + insulin resistance | Associated with overweight/obesity; usually adult onset |
| Hybrid forms | ||
| - Slowly evolving immune-mediated diabetes of adults | Similar to Type 1 in adults; features of metabolic syndrome; single GAD autoantibody; retains greater beta-cell function | Previously called LADA (Latent Autoimmune Diabetes of Adults) |
| - Ketosis-prone Type 2 | Presents with ketosis and insulin deficiency but later does not require insulin; not immune-mediated | Episodic ketosis |
| Monogenic diabetes | Caused by specific gene mutations | Neonatal DM; MODY subtypes |
| Diseases of exocrine pancreas | Trauma, tumour, inflammation, pancreatectomy | Secondary DM |
| Endocrine disorders | Excess counter-regulatory hormones | Cushing's, acromegaly, phaeochromocytoma |
| Drug or chemical-induced | Glucocorticoids, thiazides, antiretrovirals, etc. | Iatrogenic |
| Gestational diabetes mellitus (GDM) | Diabetes first diagnosed in pregnancy | High risk to mother and foetus |
- Park's Textbook of Preventive and Social Medicine, p. 443 (WHO 2019 Classification)
WHO Diagnostic Criteria for Diabetes (2019)
| Measurement | Diagnostic Cut-off |
|---|---|
| Fasting plasma glucose (venous or capillary) | ≥ 7.0 mmol/L (126 mg/dL) |
| 2-hour post-load venous plasma glucose | ≥ 11.1 mmol/L (200 mg/dL) |
| 2-hour post-load capillary plasma glucose | ≥ 12.2 mmol/L (220 mg/dL) |
| Random plasma glucose | ≥ 11.1 mmol/L (200 mg/dL) |
| HbA1c | ≥ 6.5% (48 mmol/mol) |
Impaired Fasting Glucose (IFG): Fasting glucose 6.1-6.9 mmol/L Impaired Glucose Tolerance (IGT): 2-hour glucose 7.8-11.0 mmol/L These are "pre-diabetic" states representing high risk for progression to Type 2 DM.
Prevention and Control of Diabetes
1. Primary Prevention
a. Population Strategy - Directed at the entire community:
- Promote healthy diets (reduce caloric density, increase fibre, reduce refined carbohydrates)
- Prevent and correct overweight/obesity (BMI 18.5-24.9)
- Increase physical activity - reduces insulin resistance
- Reduce alcohol consumption (alcohol indirectly increases diabetes risk)
- Health education and awareness campaigns
- Avoid diabetogenic drugs (e.g., oral contraceptives, glucocorticoids) in high-risk individuals
b. High-Risk Strategy - Targeted at susceptible individuals:
- No specific primary prevention for Type 1 (genetic counselling not yet practical)
- For Type 2: Target those with IGT/IFG, obesity, family history, sedentary lifestyle
- Correct sedentary habits, over-nutrition, and obesity
- Reduce atherosclerosis risk factors (smoking cessation, BP control, lipid management)
- Avoid diabetogenic medications in at-risk persons
High-risk groups for screening:
- Age ≥ 40 years
- Family history of diabetes
- Obese individuals
- Women who delivered a baby weighing > 4.5 kg (or > 3.5 kg in constitutionally small populations)
- Women with excess weight gain in pregnancy
- Patients with premature atherosclerosis
2. Secondary Prevention (Treatment and Complication Prevention)
- Goal: Maintain blood glucose as close to normal as practicable + maintain ideal body weight
- Treatment modalities: (a) Diet alone; (b) Diet + oral antidiabetic drugs; (c) Diet + insulin
- Monitoring: Regular blood sugar, urine for protein/ketones, BP, visual acuity, weight, foot examination
- Glycosylated haemoglobin (HbA1c): Reflects glycaemic control over the preceding 2-3 months; target < 6.5-7%
- Primary health care is the cornerstone - most diabetic care is delivered at this level
PART 2: OBESITY
Definition
"Obesity may be defined as an abnormal growth of the adipose tissue due to an enlargement of fat cell size (hypertrophic obesity) or an increase in fat cell number (hyperplastic obesity) or a combination of both."
- Park's Textbook of Preventive and Social Medicine, p. 448
Obesity is expressed primarily in terms of Body Mass Index (BMI) = Weight (kg) / Height² (m²).
WHO Classification of Obesity by BMI
| Classification | BMI (kg/m²) | Risk of Comorbidities |
|---|---|---|
| Underweight | < 18.50 | Low (but other clinical risks increased) |
| Normal range | 18.50 - 24.99 | Average |
| Overweight (Pre-obese) | 25.00 - 29.99 | Increased |
| Obese Class I | 30.00 - 34.99 | Moderate |
| Obese Class II | 35.00 - 39.99 | Severe |
| Obese Class III (Morbid) | ≥ 40.00 | Very severe |
BMI values are age-independent and the same for both sexes. Risks are continuous and graded and begin above BMI 25.
Important caveat: BMI does not distinguish fat mass from muscle mass. In Asian populations (including Indians), obesity-related metabolic complications occur at lower BMI thresholds - the WHO suggests a lower cut-off of BMI ≥ 27.5 (some guidelines use 23 for overweight in Asians).
Other Methods of Assessing Obesity
| Method | Description |
|---|---|
| BMI (Quetelet's Index) | Weight (kg) / Height² (m) - most widely used |
| Brocca Index | Height (cm) - 100 = Ideal weight in kg |
| Lorentz formula | Ht(cm) - 100 - [Ht(cm)-150]/2 (women) or /4 (men) |
| Ponderal Index | Height (cm) / ∛Body weight (kg) |
| Corpulence Index | Actual weight / Desirable weight (should not exceed 1.2) |
| Skinfold thickness | Harpenden callipers; sum < 40 mm (boys), < 50 mm (girls) |
| Waist circumference | Reflects central/abdominal fat; cut-offs: ≥ 102 cm (men), ≥ 88 cm (women) for high risk |
| Waist-to-hip ratio | > 0.9 (men), > 0.85 (women) = abdominal obesity |
Central/Abdominal Obesity and Metabolic Risk
Intra-abdominal (visceral) fat is metabolically distinct - it has:
- Higher blood flow and more glucocorticoid receptors
- Greater catecholamine-induced lipolysis
- Direct portal drainage to the liver → increases non-esterified fatty acid flux
This drives insulin resistance and the metabolic syndrome (hyperinsulinaemia + dyslipidaemia + glucose intolerance + hypertension), linking abdominal obesity to CHD.
Health Hazards of Obesity
| Risk Level | Associated Conditions |
|---|---|
| Greatly increased | Type 2 diabetes, gall bladder disease, dyslipidaemia, insulin resistance, breathlessness, sleep apnoea |
| Moderately increased | Coronary heart disease, hypertension, osteoarthritis (knees), hyperuricaemia/gout |
| Slightly increased | Breast cancer (postmenopausal), endometrial cancer, colon cancer, PCOS, impaired fertility, low back pain, anaesthetic risk, foetal defects from maternal obesity |
The Framingham Heart Study showed dramatic increases in sudden death among men >20% overweight compared to those at normal weight.
Prevention and Control of Obesity
Goal: Maintain BMI 18.5-24.9 throughout adulthood; prevent weight gain of >5 kg; aim for 5-10% reduction in existing overweight as the initial target.
Prevention should begin in early childhood - obesity is harder to treat in adults.
(a) Dietary changes:
- Reduce energy-dense foods (fats, refined sugars)
- Increase fruits, vegetables, and dietary fibre
- Avoid high-fat, high-sugar processed foods
- Eat smaller, more frequent balanced meals
(b) Physical activity:
- Regular aerobic exercise promotes weight loss and improves insulin sensitivity
- At least 30-60 minutes of moderate exercise on most days of the week
(c) Behavioural modification:
- Cognitive-behavioural therapy, self-monitoring, food diaries
- Stress management (stress promotes cortisol-driven fat accumulation)
(d) Pharmacological treatment (for BMI > 30, or > 27 with comorbidities):
- Orlistat (lipase inhibitor), GLP-1 receptor agonists (semaglutide), etc.
(e) Surgical treatment (for BMI > 40, or > 35 with comorbidities):
- Bariatric surgery (gastric bypass, sleeve gastrectomy)
(f) Community/policy level:
- Food labelling laws, sugar taxes, built environments promoting physical activity
- School-based nutrition and physical education programmes
Quick Summary
| Topic | Key Point |
|---|---|
| DM definition | Metabolic disorder with hyperglycaemia due to defects in insulin secretion/action |
| Type 1 | Immune-mediated beta-cell destruction; absolute insulin deficiency |
| Type 2 | Beta-cell dysfunction + insulin resistance; linked to obesity/sedentary lifestyle |
| New hybrid type | Slowly evolving immune-mediated DM of adults (former LADA) |
| DM diagnostic cut-off | FPG ≥ 126 mg/dL, 2-hr PG ≥ 200 mg/dL, HbA1c ≥ 6.5% |
| Obesity definition | Abnormal growth of adipose tissue (hypertrophic and/or hyperplastic) |
| Normal BMI | 18.5 - 24.99 |
| Obese | BMI ≥ 30; Class I (30-34.9), Class II (35-39.9), Class III (≥40) |
| DM prevention | Population strategy + high-risk strategy; weight control, exercise, diet |
| Obesity prevention | Starts in childhood; diet + exercise + behaviour modification |
- Park's Textbook of Preventive and Social Medicine, pp. 443-453
This is a shared conversation. Sign in to Orris to start your own chat.