ASSIGNMENT ON Diseases of heart valves -Infective endocarditis.
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Reading File
DISEASES OF HEART VALVES: INFECTIVE ENDOCARDITIS
1. DEFINITION
Infective endocarditis (IE) is a microbial infection of the endocardial surface of the heart, primarily affecting the cardiac valves, leading to the formation of vegetations composed of thrombotic debris, inflammatory cells, and microorganisms, often associated with destruction of the underlying cardiac tissue. The aorta, aneurysmal sacs, other blood vessels, prosthetic devices, and cardiovascular implantable electronic devices (e.g., pacemakers) may also be involved.
Although fungi, rickettsiae (agents of Q fever), and chlamydial species can cause endocarditis, the vast majority of cases are bacterial. - Robbins & Kumar Basic Pathology, p. 368
2. CLASSIFICATION
IE is traditionally classified based on the tempo and severity of the clinical course:
| Feature | Acute IE | Subacute IE |
|---|---|---|
| Onset | Rapid (days) | Insidious (weeks to months) |
| Causative organism | S. aureus (highly virulent) | Viridans streptococci (low virulence) |
| Valve involved | Previously healthy or damaged | Previously damaged/deformed |
| Destructiveness | Highly destructive | Relatively less destructive |
| Mortality | High, even with treatment | Lower; most recover with antibiotics |
Note: A clear delineation between acute and subacute endocarditis is not always possible; many cases fall along the spectrum. Modern classification also considers causative organism, involved valve, and "pace" of clinical disease.
- Robbins & Kumar Basic Pathology, p. 368; Goldman-Cecil Medicine, p. 700
3. EPIDEMIOLOGY
-
Incidence in the United States: approximately 10,000 to 20,000 new cases per year, accounting for about 1 case per 1,000 hospital admissions.
-
In developing countries (where rheumatic fever is still endemic): younger adults with rheumatic heart disease; subacute course; caused by viridans group streptococci (VGS).
-
In developed countries: older patients with health care exposure; acute illness caused primarily by S. aureus; worse outcomes.
-
Injection drug use (IDU): a significant contributing factor due to the opioid epidemic, predominantly causing right-sided (tricuspid) endocarditis with S. aureus.
-
Braunwald's Heart Disease, p. 3533; Goldman-Cecil Medicine, p. 700-701
4. PREDISPOSING CONDITIONS (RISK FACTORS)
More Common
- Mitral valve prolapse (especially with regurgitation) - the leading pre-existing risk factor in developed countries
- Degenerative valvular disease (especially in elderly)
- Injection drug use
- Congenital heart disease (uncorrected ventricular septal defect)
- Previous endocarditis
- Prosthetic heart valves (account for 10-20% of all IE cases)
Less Common
- Rheumatic heart disease (historically dominant; now less common)
- Idiopathic hypertrophic subaortic stenosis
- Coarctation of the aorta
- Complex congenital heart disease
Host Factors
-
Neutropenia, immunodeficiency, malignancy
-
Diabetes mellitus
-
Alcohol or intravenous drug use
-
HIV infection (independent risk factor in IDUs, risk increasing as CD4 count decreases)
-
End-stage renal disease on hemodialysis
-
Goldman-Cecil Medicine, Table 61-1, p. 700; Robbins & Kumar, p. 368
5. ETIOLOGY (MICROBIOLOGY)
The three most common causes worldwide are staphylococci, streptococci, and enterococci:
| Organism | Setting | Type of IE |
|---|---|---|
| Streptococcus viridans | Community-acquired; damaged/deformed valves; oral flora | Subacute |
| Staphylococcus aureus | Healthcare settings; IV drug users; healthy valves | Acute |
| Enterococci | GI/GU sources; elderly | Variable |
| HACEK group* | Normal oral flora; fastidious organisms | Subacute |
| Coagulase-negative staphylococci | Prosthetic valves; healthcare-associated | Subacute |
| Fungi (Candida, Aspergillus) | Immunocompromised; IV drug users; prosthetic valves | Acute/subacute |
| Gram-negative bacilli | Rare; IV drug users | Variable |
*HACEK = Haemophilus, Aggregatibacter (formerly Actinobacillus), Cardiobacterium, Eikenella, Kingella
-
Culture-negative endocarditis: ~10% of all cases - due to prior antibiotic therapy or fastidious organisms (Bartonella, Coxiella, Brucella, Tropheryma whipplei).
-
Robbins & Kumar, p. 368; Goldman-Cecil Medicine, p. 701
6. PATHOGENESIS
Infective endocarditis follows a predictable sequence of events:
- Endothelial damage - Turbulent blood flow, mechanical trauma, or foreign bodies cause disruption of the smooth endothelial surface.
- Sterile vegetation (NBTE) - Aggregation of platelets, fibrin, and coagulation molecules forms a "sterile vegetation" (nonbacterial thrombotic endocarditis).
- Bacteremia - Transient bacteremia (from dental procedures, surgery, IV drug use, GI/GU sources, or occult sources) seeds the sterile vegetation.
- Microbial adhesion and proliferation - Certain organisms (especially staphylococci and streptococci) express specific adhesins to attach to damaged surfaces. Bacteria proliferate within the vegetation, achieving loads of 10⁹ to 10¹¹ colony-forming units per gram of tissue.
- Metastatic infection - Emboli shed from friable vegetations seed organs with high blood flow (kidneys, spleen, brain), causing septic infarcts and mycotic aneurysms.
Key point: Valve surfaces and vegetations are avascular, making antibiotic penetration and healing difficult.
- Goldman-Cecil Medicine, p. 1681; Robbins & Kumar, p. 368
7. MORPHOLOGY (GROSS AND MICROSCOPIC PATHOLOGY)
Gross Appearance
- Friable, bulky, potentially destructive vegetations on heart valves containing fibrin, inflammatory cells, and microorganisms (Fig. 9.20, 9.21 - Robbins).
- Aortic and mitral valves are the most common sites of infection (left-sided).
- Tricuspid valve is a frequent target in IV drug users (right-sided).
- Vegetations may be single or multiple and can involve more than one valve.
- Vegetations can erode into underlying myocardium to produce an abscess cavity (ring abscess).
- Shedding of emboli is common due to friable nature.
Comparison of Vegetations in Valvular Diseases
The diagram below from Robbins Pathology compares vegetation locations across four conditions:
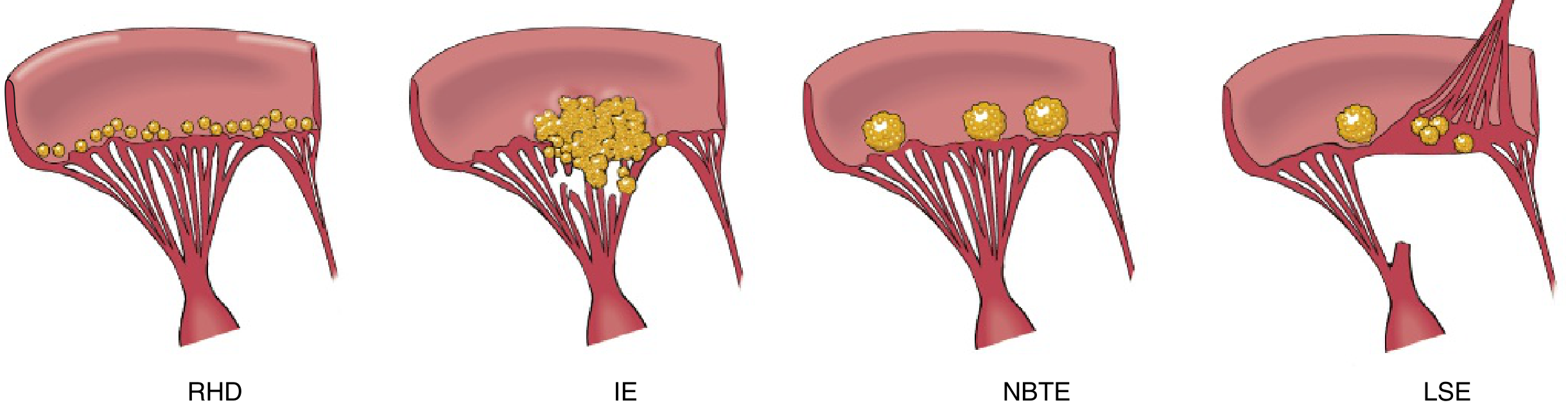
Fig: Diagrammatic comparison of vegetations in Rheumatic Heart Disease (RHD), Infective Endocarditis (IE), Nonbacterial Thrombotic Endocarditis (NBTE), and Libman-Sacks Endocarditis (LSE). IE shows large, irregular, destructive vegetations on the valve leaflet and chordae tendineae - distinct from the smaller, non-destructive vegetations of NBTE and the line of closure deposits in RHD.
| Feature | IE | NBTE | RHD |
|---|---|---|---|
| Location | Any surface; irregular; destructive | Line of closure; small | Line of closure; small, bead-like |
| Composition | Organisms + fibrin + PMNs | Sterile fibrin/platelets | Sterile; fibrin |
| Destruction | Yes (ulceration, perforation) | No | Mild sclerosis |
- Robbins & Kumar Basic Pathology, p. 368-369
8. CLINICAL FEATURES
Symptoms
- Fever (most consistent sign; present in up to 96%) - may be absent in elderly or those with renal/cardiac failure
- Constitutional symptoms: fatigue, malaise, weight loss
- Musculoskeletal symptoms: arthralgia, myalgia (~50%)
- Low back pain (~5-10%), even without osteomyelitis
- Right-sided IE (IV drug users, device-related): pleuritic chest pain, multilobar pneumonia
Cardinal Physical Signs (Stigmata of Endocarditis)
| Sign | Description | Mechanism | Frequency |
|---|---|---|---|
| Fever | Persistent, spiking | Bacteremia | 96% |
| New or changing murmur | Regurgitant murmur | Valve destruction | 48% (new), 20% (worsening) |
| Petechiae | Conjunctiva, palate, extremities | Microemboli | Common |
| Splinter hemorrhages | Linear, subungual | Microemboli in nail beds | 8% |
| Osler nodes | Painful, red nodules on finger/toe pads | Immune complex + microemboli | 3% |
| Janeway lesions | Painless, erythematous macules on palms/soles | Septic microemboli | 5% |
| Roth spots | Retinal hemorrhages with pale centre | Microemboli / immune complex | 2% |
| Splenomegaly | Enlarged spleen | Chronic infection (subacute) | 11% |
| Clubbing | Finger clubbing | Chronic hypoxia/infection | Late feature |
| Embolic events | Stroke, infarcts | Vegetation fragmentation | 17% |
Memory aid: "From Jane's Roth Spots, Osler Hoped to Prove Clubbing" - Janeway lesions, Roth Spots, Osler nodes, Heart murmur, Petechiae, Clubbing
- Goldman-Cecil Medicine, Table 61-2, p. 1694-1700; Robbins & Kumar, p. 368-369
9. LABORATORY INVESTIGATIONS
| Investigation | Finding/Purpose |
|---|---|
| Blood cultures (most important) | 3 sets from different sites before antibiotics; identifies causative organism |
| CBC | Leukocytosis (acute); normochromic normocytic anemia (subacute) |
| ESR / CRP | Elevated (ESR elevated in ~61% of cases) |
| Urine analysis | Hematuria in ~26%; proteinuria (glomerulonephritis) |
| Rheumatoid factor | Positive in ~5% |
| Procalcitonin | Guides therapy duration |
| Echocardiography | Primary imaging modality |
| Chest X-ray | Abnormal in 67-85% in right-sided IE (effusion, septic emboli) |
| ECG | New conduction delay suggests myocardial abscess |
Echocardiography
-
TTE (Transthoracic Echocardiography): First-line; may miss small vegetations
-
TEE (Transesophageal Echocardiography): More sensitive; used when:
- TTE negative but high clinical suspicion
- Prosthetic valve involvement
- Suspected perivalvular extension
- Staphylococcal bacteremia
-
CT angiography / PET-CT: Useful for prosthetic valve IE or perivalvular complications
-
Braunwald's Heart Disease, p. 1235-1240; Goldman-Cecil Medicine, p. 1881
10. DIAGNOSIS: MODIFIED DUKE CRITERIA
The Modified Duke Criteria (Li et al., 2000) is the standard diagnostic framework, validated across diverse patient populations.
MAJOR CRITERIA
1. Blood Culture Positive for IE
- Typical microorganisms from 2 separate blood cultures: viridans streptococci, S. bovis, HACEK group, S. aureus, or community-acquired enterococci in the absence of a primary focus; OR
- Microorganisms consistent with IE from persistently positive blood cultures (≥2 positive cultures drawn >12 hours apart; or all 3, or majority of ≥4 separate cultures)
- Single positive blood culture for Coxiella burnetii or anti-phase 1 IgG antibody titer ≥1:800
2. Evidence of Endocardial Involvement
- Echocardiogram positive for IE: oscillating intracardiac mass on valve or supporting structure, in the path of regurgitant jets, or on implanted material, without alternative explanation; or abscess; or new partial dehiscence of prosthetic valve; OR
- New valvular regurgitation (worsening or changing of preexisting murmur is not sufficient)
MINOR CRITERIA
- Predisposing condition: IV drug use or predisposing cardiac condition
- Fever ≥38°C
- Vascular phenomena: arterial embolism, septic pulmonary emboli, mycotic aneurysm, intracranial hemorrhage, conjunctival hemorrhages, Janeway lesions
- Immunologic phenomena: glomerulonephritis, Osler nodes, Roth spots, rheumatoid factor
- Echocardiogram findings consistent with endocarditis but not meeting major criteria
- Microbiologic evidence: positive blood cultures not meeting major criteria or serologic evidence of active infection
Classification
| Category | Criteria |
|---|---|
| Definite IE | 2 major criteria OR 1 major + 3 minor OR 5 minor criteria (or pathological proof) |
| Possible IE | 1 major + 1 minor OR 3 minor criteria |
| Rejected IE | Firm alternative diagnosis; resolution with ≤4 days antibiotics; no pathological evidence |
- Goldman-Cecil Medicine, p. 1757-1796; Fuster and Hurst's The Heart 15e, p. 1203-1207
11. COMPLICATIONS
Cardiac Complications
- Valvular regurgitation / heart failure - most common cause of death; from leaflet destruction or perforation
- Perivalvular abscess (ring abscess) - most common with aortic valve IE; presents with new AV conduction block on ECG
- Pericarditis / myocarditis
- Fistula formation between cardiac chambers
Embolic Complications (Most common non-cardiac complications)
- Systemic emboli (in left-sided IE): stroke, renal infarction, splenic infarction, mesenteric ischemia, peripheral arterial occlusion
- Pulmonary emboli (in right-sided IE): septic pulmonary emboli, pneumonia, pleural effusion
- Mycotic aneurysms: from bacterial infection of arterial walls at embolic sites; can rupture
Neurological Complications (~15-30%)
- Embolic stroke (ischemic most common)
- Intracranial hemorrhage (from mycotic aneurysm rupture or hemorrhagic transformation)
- Brain abscess
- Meningitis
Renal Complications
- Immune complex glomerulonephritis (hematuria, proteinuria, renal failure) - from glomerular trapping of antigen-antibody complexes
- Renal infarction from emboli
- Antibiotic-related nephrotoxicity (aminoglycosides, vancomycin)
Other Complications
-
Musculoskeletal: osteomyelitis, septic arthritis, vertebral osteomyelitis (causing back pain)
-
Splenic abscess
-
Robbins & Kumar, p. 368-369; Goldman-Cecil Medicine, p. 1973-1974
12. TREATMENT
General Principles
- All patients with IE should be managed inpatient in a medical center with an experienced multidisciplinary "Endocarditis Team" (infectious disease + cardiology + cardiac surgery).
- Treatment involves prolonged IV antibiotic therapy (usually 4-6 weeks) guided by blood cultures and sensitivity testing.
- Empiric therapy is initiated in acutely ill patients, high-risk patients (prosthetic valves), or those with complications.
- Stable patients with subacute presentation without complications can be observed and blood cultures obtained before starting antibiotics.
Empirical Antibiotic Therapy
| Patient Type | Empirical Regimen |
|---|---|
| Native valve, community-acquired, MRSA unlikely | Nafcillin 2g IV q4h + Penicillin 4 million units IV q4h + Gentamicin 1 mg/kg IV q8h |
| Healthcare-associated / suspected MRSA / penicillin allergy | Vancomycin 15-20 mg/kg IV q8-12h (trough 15-20 mg/L) + Gentamicin 1 mg/kg IV q8h |
| Prosthetic valve | Vancomycin + Gentamicin + Rifampin 300 mg PO/IV q8h |
Organism-Specific Therapy (Selected)
| Organism | Drug of Choice |
|---|---|
| Viridans streptococci (penicillin-sensitive) | Penicillin G IV or Ceftriaxone for 4 weeks |
| S. aureus (MSSA), native valve | Nafcillin or Oxacillin for 6 weeks |
| S. aureus (MRSA) | Vancomycin for 6 weeks |
| Enterococci | Ampicillin + Gentamicin (4-6 weeks) |
| HACEK organisms | Ceftriaxone for 4 weeks |
| Candida endocarditis | Amphotericin B ± azoles + valve surgery |
| Bartonella | Doxycycline 6 weeks + Gentamicin 2 weeks |
| Coxiella (Q fever) | Doxycycline + Hydroxychloroquine (≥18 months) |
Note: Rifampin is never used as monotherapy due to rapid resistance development.
Surgical Treatment
Indications for urgent/early valve surgery:
| Indication | Timing |
|---|---|
| Heart failure due to severe valvular regurgitation/obstruction | Emergency/urgent |
| Perivalvular extension (abscess, fistula, new conduction block) | Urgent |
| Uncontrolled infection (persistent bacteremia >5-7 days, fungal IE) | Urgent |
| Prevention of embolism (large mobile vegetation >10mm with prior embolism) | Early elective |
| Prosthetic valve dehiscence | Urgent |
- Goldman-Cecil Medicine, p. 1886-2000; Braunwald's Heart Disease, p. 1230
13. ANTIBIOTIC PROPHYLAXIS
The AHA 2021 Scientific Statement updated prophylaxis guidelines:
Conditions Warranting Antibiotic Prophylaxis Before Invasive Dental Procedures:
- Prosthetic cardiac valve or prosthetic material used for valve repair
- History of previous IE
- Congenital heart disease (unrepaired cyanotic CHD; repaired CHD with residual defects; repaired CHD within 6 months of procedure)
- Cardiac transplant recipients with valvulopathy
- Ventricular assist devices and implantable hearts (newly added in 2021)
Prophylaxis Regimen (Dental Procedures):
- Amoxicillin 2g PO 30-60 min before procedure (preferred)
- If unable to take oral: Ampicillin 2g IM/IV
- Penicillin allergy: Doxycycline 100mg PO (new addition in 2021; clindamycin eliminated due to C. difficile risk)
- Azithromycin/clarithromycin 500mg PO as alternative
Routine antibiotic prophylaxis is no longer recommended for GI endoscopy or urologic procedures.
- Braunwald's Heart Disease, p. 1230-1233
14. PROGNOSIS
-
Left untreated, IE is generally fatal.
-
With appropriate antibiotic therapy and/or valve replacement, mortality is significantly reduced.
-
Adverse prognostic factors:
- Heart failure (most common cause of death)
- S. aureus etiology
- Prosthetic valve infection
- Older age, comorbidities
- Perivalvular extension/abscess
- Renal failure
- Neurological complications
-
In-hospital mortality ranges from 15-30% in developed countries.
-
Robbins & Kumar, p. 369; Goldman-Cecil Medicine, p. 1970
15. SPECIAL SITUATIONS
IV Drug Users (Right-Sided IE)
- Tricuspid valve most commonly affected
- S. aureus predominates
- Presents with fever, septic pulmonary emboli, and multilobar pneumonia
- Better prognosis than left-sided IE; more responsive to medical therapy
- High risk of recurrence
Prosthetic Valve Endocarditis (PVE)
- Early PVE (<12 months post-surgery): Coagulase-negative staphylococci, S. aureus, gram-negative bacilli; carries worse prognosis
- Late PVE (>12 months): Similar to native valve endocarditis
- TEE preferred for diagnosis; surgery often required
Healthcare-Associated IE
- More than one-third of cases in non-drug-using patients
- Caused primarily by S. aureus; MRSA must be considered
- Sources: IV catheters, hemodialysis access, pacemakers/ICD leads
SUMMARY TABLE
| Feature | Details |
|---|---|
| Definition | Microbial infection of endocardial surface/valves with vegetation formation |
| Most common organisms | S. aureus (acute), Viridans streptococci (subacute) |
| Most common risk factor (modern) | Mitral valve prolapse (developed countries) |
| Most common valve involved | Mitral > Aortic (left-sided); Tricuspid (IV drug users) |
| Hallmark lesion | Friable vegetations on valve leaflets |
| Diagnostic tool | Modified Duke Criteria + Blood cultures + Echocardiography |
| Most common complication | Heart failure (from valvular destruction) |
| Most common cause of death | Heart failure |
| Treatment | Prolonged IV antibiotics (4-6 weeks) ± valve surgery |
Sources:
- Robbins & Kumar Basic Pathology, pp. 368-369
- Goldman-Cecil Medicine International Edition, 2 Vol Set, pp. 700-705, 1678-2000
- Braunwald's Heart Disease: A Textbook of Cardiovascular Medicine, pp. 1221-1340
- Fuster and Hurst's The Heart, 15th Edition, pp. 999-1022
This is a shared conversation. Sign in to Orris to start your own chat.