Explain spinal chord
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Finding Sources
Loading Image
Reading File
I now have comprehensive, well-sourced information to provide a thorough answer. Let me compose the full response.
The Spinal Cord
Overview
The spinal cord is the most caudal (tail-end) portion of the central nervous system (CNS). It acts as the main communication highway between the brain and the rest of the body - carrying sensory signals up to the brain and motor commands down to the muscles and organs.
- Costanzo Physiology, p. 76
Location and Extent
The spinal cord extends from the foramen magnum (base of skull) down to approximately the L1-L2 intervertebral disc in adults (though it can end as high as T12 or as low as the L2-L3 disc). In neonates, it extends to around L3-L4.
The tapered distal tip is called the conus medullaris. Below it, a fine strand of connective tissue called the filum terminale (the pial part) continues inferiorly, anchoring the cord.
- Gray's Anatomy for Students, p. 119
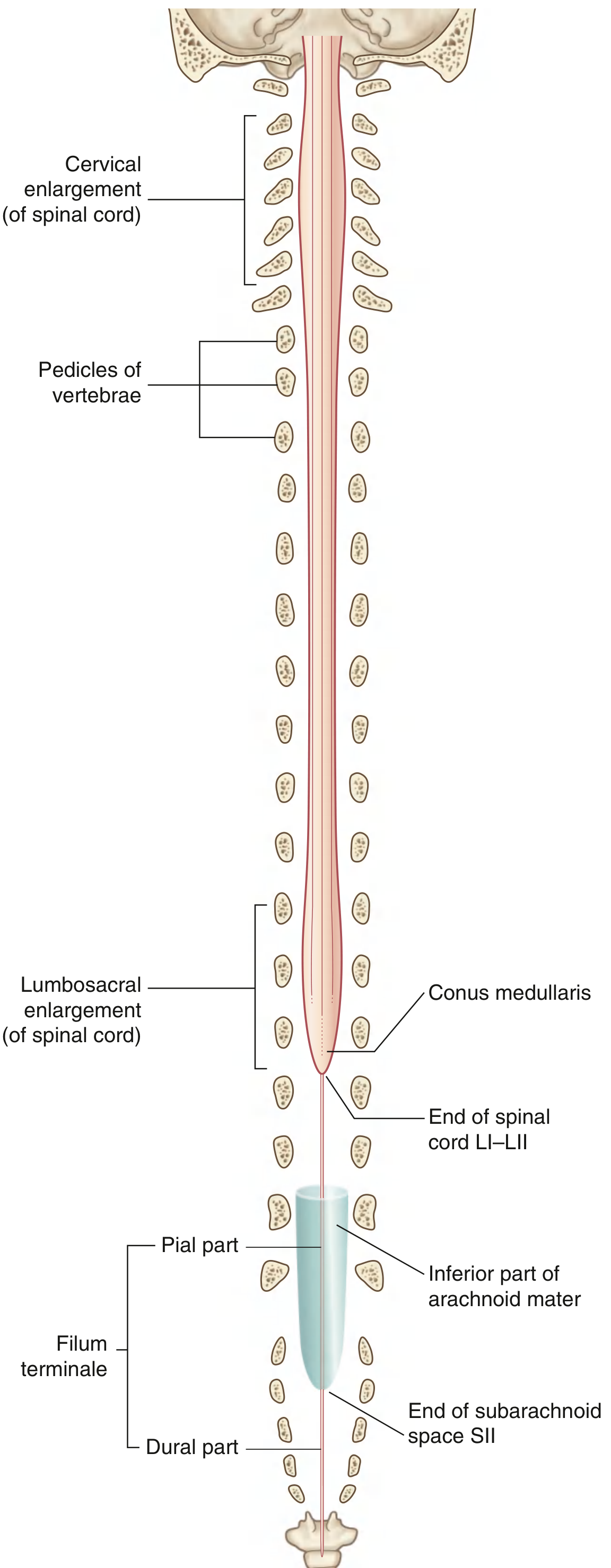
Fig. 2.53 - Spinal Cord (Gray's Anatomy for Students)
Enlargements
The cord is not uniform in diameter. It has two notable swellings:
| Enlargement | Region | Spinal Levels | Function |
|---|---|---|---|
| Cervical enlargement | Upper limb innervation | C5 - T1 | Motor + sensory for arms/hands |
| Lumbosacral enlargement | Lower limb innervation | L1 - S3 | Motor + sensory for legs/feet |
- Gray's Anatomy for Students, p. 119
Spinal Segments and Nerves
The spinal cord is segmented, giving rise to 31 pairs of spinal nerves:
- 8 Cervical (C1-C8)
- 12 Thoracic (T1-T12)
- 5 Lumbar (L1-L5)
- 5 Sacral (S1-S5)
- 1 Coccygeal
Each spinal nerve contains both:
-
Sensory (afferent) fibers - entering via the dorsal root from skin, joints, muscles, and viscera
-
Motor (efferent) fibers - exiting via the ventral root to skeletal muscle (somatic) or smooth muscle/glands (autonomic)
-
Costanzo Physiology, p. 76; Miller's Review of Orthopaedics, p. 242
External Surface Features
The outer surface of the spinal cord has several important landmarks:
| Structure | Location | Significance |
|---|---|---|
| Anterior median fissure | Front midline | Deep groove along full length |
| Posterior median sulcus | Back midline | Shallow groove |
| Posterolateral sulcus | Posterior lateral surface | Where dorsal nerve rootlets enter |
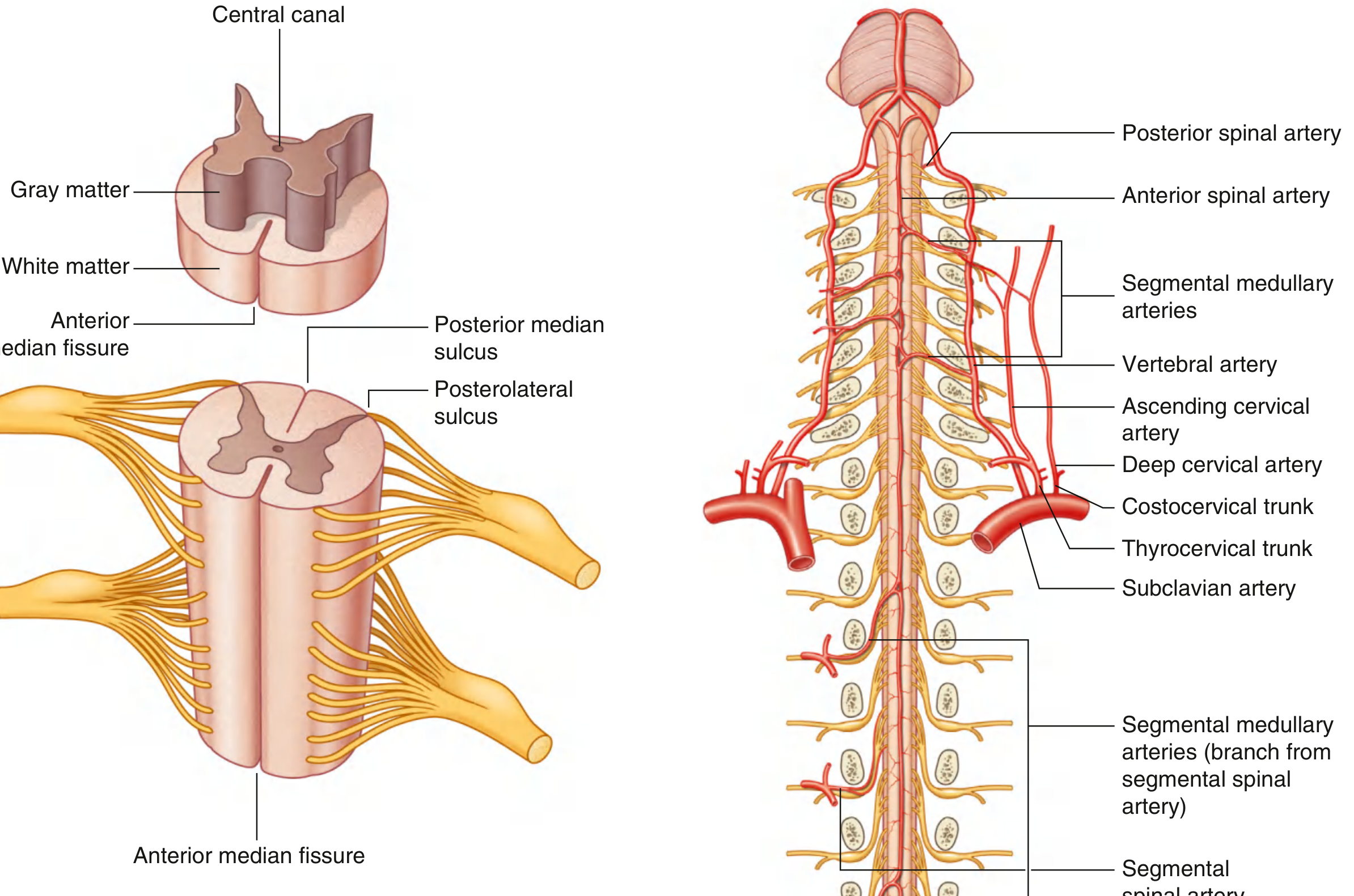
Fig. 2.54 - Features and Blood Supply of the Spinal Cord (Gray's Anatomy for Students)
Internal Structure
Internally, the cord has a central canal surrounded by two tissue types arranged concentrically:
Gray Matter (Butterfly/H-shape)
- Located centrally; rich in nerve cell bodies
- Forms longitudinal columns that appear H-shaped in cross-section
- Organized into horns:
- Dorsal horn - receives sensory input
- Ventral horn - contains lower motor neurons (LMNs) that directly drive muscles
- Lateral horn (only T1-L2/S2-S4) - contains preganglionic autonomic neurons
White Matter (Peripheral)
- Surrounds the gray matter; rich in myelinated axon tracts
- Organized into three pairs of funiculi (columns):
- Posterior (dorsal) funiculi
- Lateral funiculi
- Anterior (ventral) funiculi
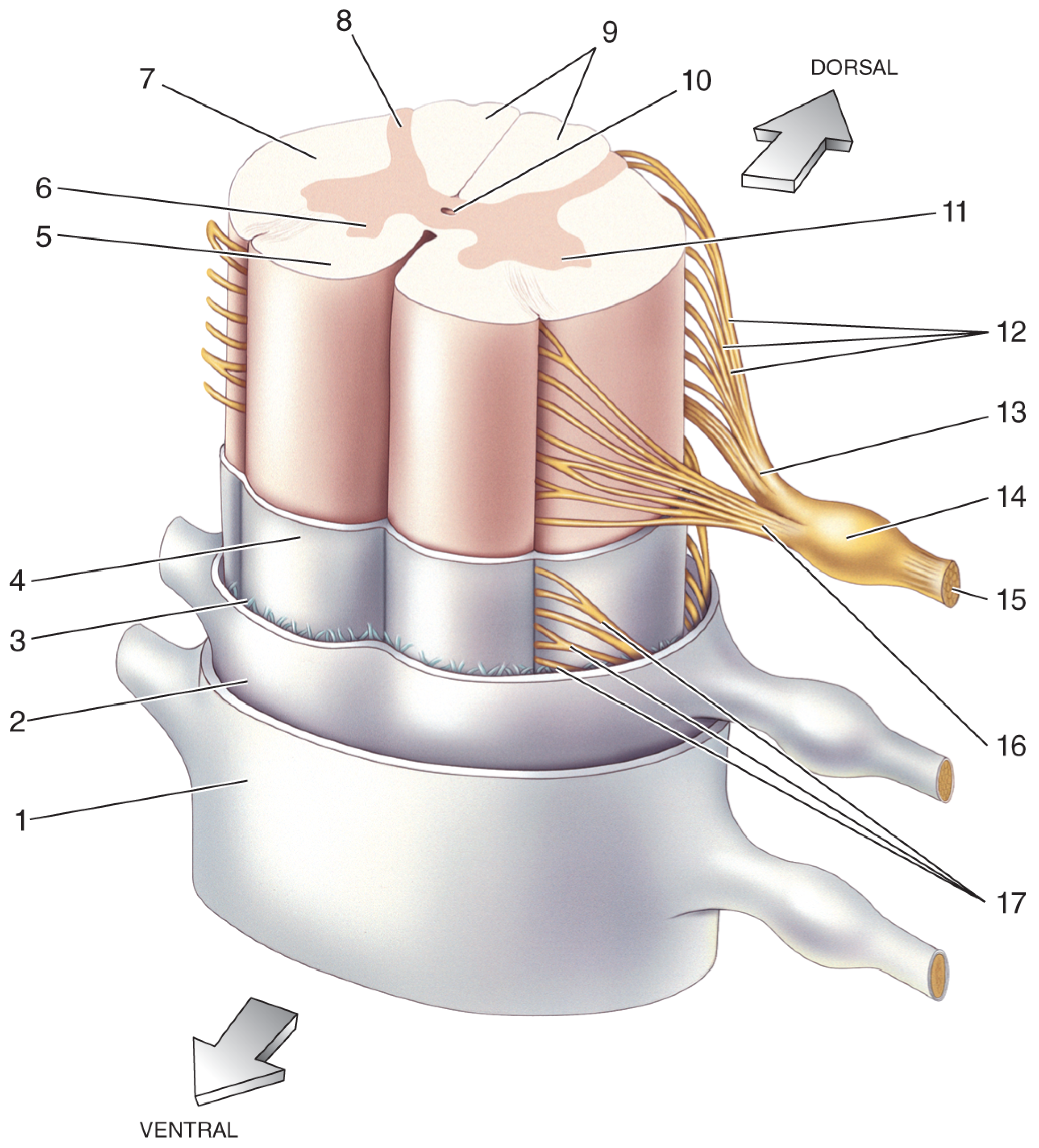
Spinal Cord Cross-Sectional Anatomy (Neuroscience: Exploring the Brain)
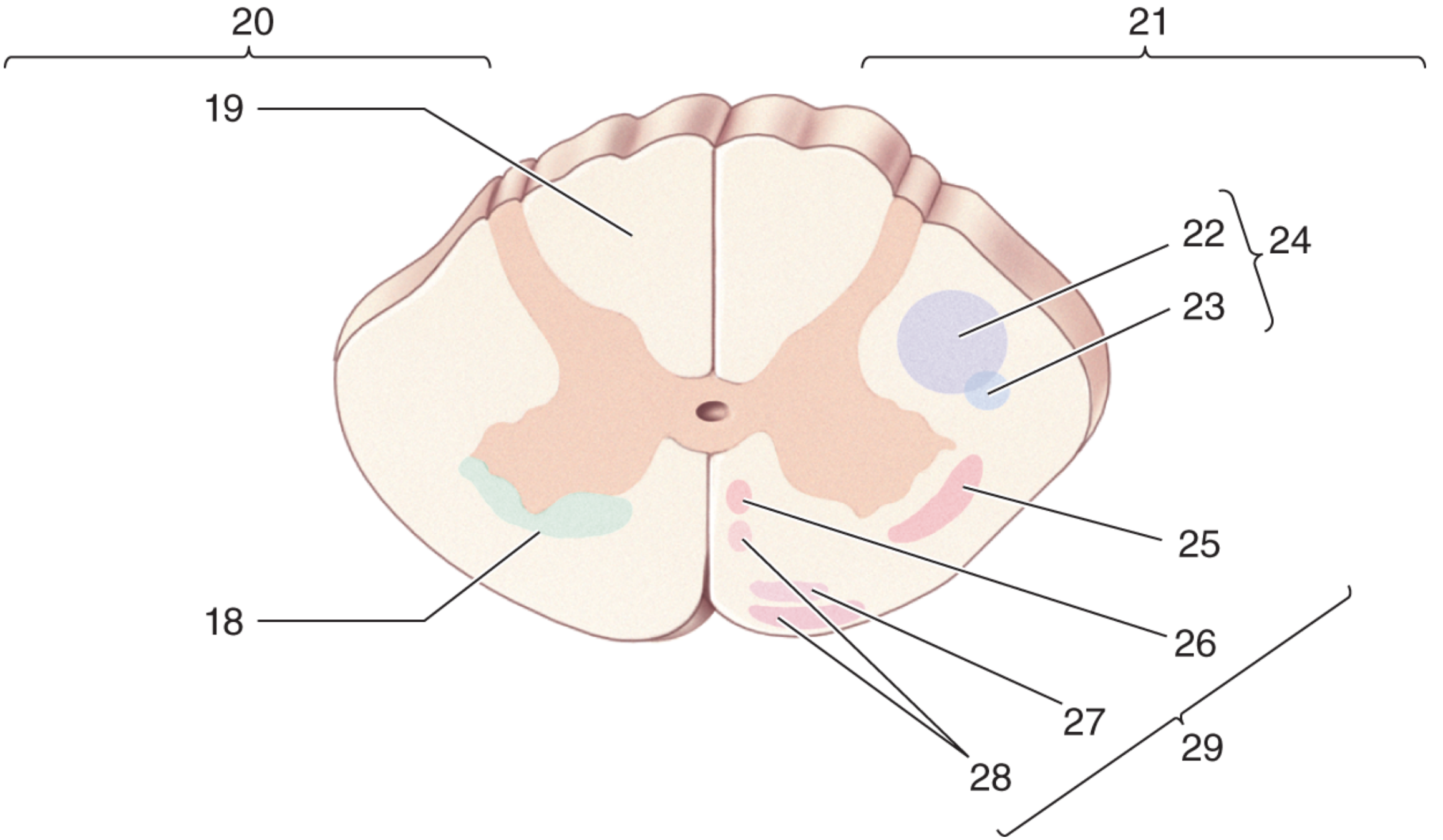
Spinal Cord Tract Regions (Neuroscience: Exploring the Brain)
Major White Matter Tracts
Ascending (Sensory) Tracts
| Tract | Location | Sensation Carried |
|---|---|---|
| Posterior columns (dorsal funiculi) | Posterior | Fine touch, vibration, proprioception |
| Lateral spinothalamic tract | Lateral funiculus | Pain and temperature |
| Anterior spinothalamic tract | Anterior funiculus | Crude/light touch |
| Spinocerebellar tracts | Lateral funiculus | Unconscious proprioception to cerebellum |
Descending (Motor) Tracts
| Tract | Location | Function |
|---|---|---|
| Lateral corticospinal tract | Lateral funiculus | Voluntary movement (contralateral, ~90% of fibers) |
| Anterior corticospinal tract | Anterior funiculus | Voluntary movement (ipsilateral/bilateral) |
| Rubrospinal, reticulospinal, vestibulospinal | Lateral/anterior | Posture, balance, muscle tone |
A key clinical note: in the lateral corticospinal tract, sacral fibers lie most peripherally and cervical fibers more medially. This somatotopic arrangement explains why a central cord injury preferentially affects the arms (cervical) more than the legs (sacral).
- Miller's Review of Orthopaedics, p. 242
Blood Supply
The spinal cord is supplied by three longitudinal arteries running along its length:
- Anterior spinal artery (1) - midline, formed from both vertebral arteries; supplies the anterior 2/3 of the cord including motor tracts
- Posterior spinal arteries (2) - one on each side; supply the posterior columns
These are reinforced at intervals by segmental medullary arteries branching from vertebral, deep cervical, subclavian, intercostal, and lumbar arteries. The most important is the artery of Adamkiewicz (great radicular artery), usually entering at T9-T12 on the left, supplying the lumbosacral enlargement.
Protective Coverings (Meninges)
The spinal cord is wrapped in three meningeal layers:
- Dura mater - tough outermost layer
- Arachnoid mater - middle layer; the subarachnoid space (between arachnoid and pia) contains cerebrospinal fluid (CSF)
- Pia mater - innermost layer, tightly adherent to the cord surface
The subarachnoid space ends at S2, which is why lumbar punctures are performed below L2 (within the lumbar cistern, below the cord), safely drawing CSF from around the cauda equina roots.
Key Clinical Points
| Concept | Explanation |
|---|---|
| Cauda equina | Bundle of nerve roots (L2 and below) that travel through the lumbar canal below the conus medullaris |
| Brown-Sequard syndrome | Hemisection of the cord: ipsilateral motor loss + proprioception loss; contralateral pain/temp loss (due to crossing of spinothalamic tract) |
| Central cord syndrome | Cervical injury preferentially affects arms > legs (sacral fibers peripheral in lateral CST) |
| Anterior cord syndrome | Bilateral motor loss + pain/temp loss with preserved posterior column (vibration/proprioception) |
| Conus medullaris syndrome | Lower motor neuron signs + autonomic dysfunction (bowel/bladder) |
Sources:
- Gray's Anatomy for Students (9780323934237) - Spinal Cord section
- Costanzo Physiology 7th Edition (9780323793339) - CNS organization
- Neuroscience: Exploring the Brain 5th Ed (9781284286878) - Cross-sectional anatomy
- Miller's Review of Orthopaedics 9th Ed (9780443112140) - Tracts and nerve roots
Infinites potential
Asking for Preferences
Many people complaint about disc pain
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Loading Image
Reading File
Reading File
I now have comprehensive content from multiple authoritative sources. Let me compose the full answer.
Disc Pain (Intervertebral Disc Disease)
Disc pain is one of the most common musculoskeletal complaints worldwide. It affects otherwise healthy people most often in their 3rd and 4th decades of life, though back pain from discs can begin as early as the second decade.
What is an Intervertebral Disc?
The intervertebral disc sits between each pair of vertebrae and acts as a shock absorber. It has two main parts:
| Part | Structure | Function |
|---|---|---|
| Nucleus pulposus | Gel-like center, high water content | Absorbs compressive load; appears bright on T2 MRI |
| Annulus fibrosus | Tough outer fibrous ring | Holds the nucleus in place and resists tensile forces |
With aging, the nucleus pulposus gradually desiccates (dries out), losing its water content and shock-absorbing ability. This is the starting point of disc degeneration.
- Campbell's Operative Orthopaedics 15th Ed, p. 198
How Does Disc Pain Develop?
1. Degenerative Disc Disease
The normal aging process causes gradual loss of disc height and hydration. Heavy exertion, repetitive bending, twisting, or heavy lifting accelerates this process. Risk factors include:
-
Family history (genetic predisposition)
-
Male gender
-
Age 30-50 years
-
Heavy physical labor or stressful occupation
-
Cigarette smoking
-
Lower socioeconomic status
-
Bailey and Love's Short Practice of Surgery 28th Ed, p. 1020
2. Disc Herniation (Prolapse / "Slipped Disc")
When the annulus fibrosus tears or weakens, the nucleus pulposus can bulge outward. This can be:
| Type | Description |
|---|---|
| Bulge | Disc extends beyond its normal margins symmetrically |
| Protrusion | Focal bulging with the base wider than the extension |
| Extrusion | Nucleus pushes through the annulus |
| Sequestration | A free fragment breaks off entirely into the spinal canal |
Over 90% of lumbar herniations occur at L4/5 or L5/S1 - the most mechanically stressed levels in the spine.
Types of Pain
Disc disease produces two distinct pain patterns:
Axial (Back) Pain
- Felt directly in the lower back
- Often brought on by heavy lifting, bending, or twisting
- Relieved by rest
- Can radiate to the sacroiliac region and buttocks
- May have been intermittent for months or years before becoming severe
Radicular Pain (Sciatica)
- Caused by nerve root compression by the herniated disc
- Radiates below the knee following a specific dermatome
- Usually leg pain equals or exceeds back pain - this is a key diagnostic clue
- Worsens with sitting, driving, sneezing, straining, or coughing
- Relieved by lying in the semi-Fowler (reclined) position
A posterolateral L4/5 disc protrusion typically affects the L5 nerve root. A far-lateral (extraforaminal) L5/S1 protrusion affects the L5 root (the exiting, not traversing, root).
- Campbell's Operative Orthopaedics 15th Ed, p. 2352; Bailey and Love's Surgery, p. 1026
Symptoms at a Glance
| Symptom | What It Means |
|---|---|
| Lower back + leg pain | Classic disc herniation |
| Pain worse with sitting/coughing | Increased intradiscal pressure compressing nerve |
| Numbness/tingling in leg or foot | Nerve root irritation (paresthesias) |
| Muscle weakness in leg | Motor nerve root compression |
| Loss of reflexes | e.g., knee jerk (L4), ankle jerk (S1) |
| Bilateral leg pain + bladder/bowel issues | Cauda equina syndrome - medical emergency |
MRI: The Gold Standard Investigation
MRI is the procedure of choice for evaluating disc disease. On MRI:
- T2-weighted images: Normal disc = bright (high water content). Degenerated disc = dark (desiccated)
- Herniated/extruded disc appears as a convex or polypoid mass extending posteriorly into the epidural space
- Can directly show nerve root compression and spinal cord changes (myelopathy)
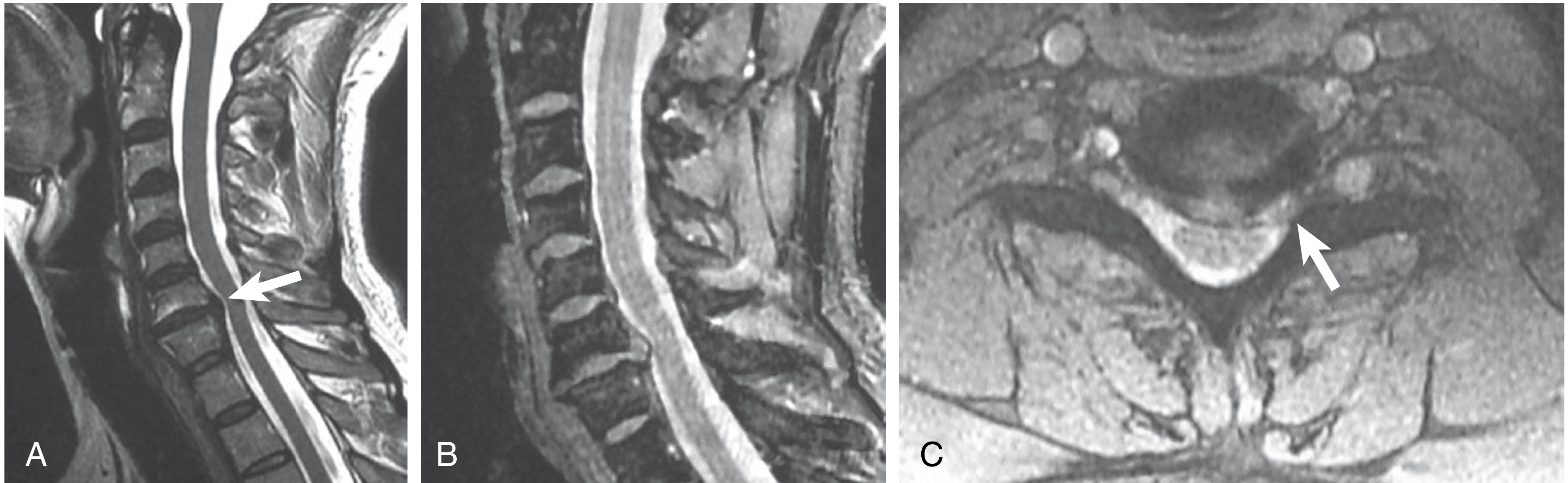
MRI of cervical disc herniation/extrusion: A) T2 sagittal showing extruded C6-C7 disc (arrow), B) Gradient echo sagittal, C) Axial view showing left eccentric extrusion compressing the cord (arrow) - Campbell's Operative Orthopaedics
- Campbell's Operative Orthopaedics 15th Ed, p. 197-198
Treatment
Conservative (First Line) - Effective in ~70% within 6-12 weeks
- Rest (avoid aggravating activities; not strict bed rest)
- NSAIDs / analgesics (e.g., ibuprofen, naproxen)
- Physiotherapy - core strengthening, posture correction
- Pregabalin (GABA analogue) for neuropathic/radicular pain
- Epidural steroid injections (transforaminal) - reduce inflammation around the nerve root
Surgical (When Conservative Fails)
-
Microdiscectomy: Standard procedure for lumbar disc herniation failing 6-12 weeks of conservative treatment
- Prone position with fluoroscopic level confirmation
- Ligamentum flavum removed to enter the spinal canal
- Thecal sac and nerve root retracted medially
- Herniated disc fragment removed via annulotomy
- Patient typically discharged the next morning
-
Bailey and Love's Short Practice of Surgery, p. 1036-1047
Cauda Equina Syndrome = Surgical Emergency
Bilateral leg pain, saddle anesthesia (inner thighs/perianal), bladder/bowel incontinence, and impotence indicate a large central disc herniation compressing the cauda equina. This requires urgent MRI and emergency surgical decompression.
Common Levels Affected
| Region | Most Common Level | Typical Symptoms |
|---|---|---|
| Lumbar | L4/5 and L5/S1 | Sciatica, leg weakness, foot drop (L5), absent ankle jerk (S1) |
| Cervical | C5/6 and C6/7 | Arm/hand pain, neck stiffness, bicep/tricep weakness |
| Thoracic | Rare | Mid-back pain, intercostal neuralgia |
Sources:
- Campbell's Operative Orthopaedics 15th Ed 2026 (9780443117633)
- Bailey and Love's Short Practice of Surgery 28th Ed (9780367548117)
- Miller's Review of Orthopaedics 9th Ed (9780443112140)
- Schwartz's Principles of Surgery 11th Ed (9781259835346)
This is a shared conversation. Sign in to Orris to start your own chat.