Synovial sarcoma of Rt proximal arm Pathophysiology Clinical features Investigation Managment Radiation therapy to be given Prognosis Complication Follt standard guidlines
Reading File
Finding Sources
Searching PubMed
"synovial sarcoma"[MeSH Terms] AND "treatment" AND "guidelines"
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Searching PubMed
"synovial sarcoma"[MeSH Terms] AND "radiotherapy" AND "chemotherapy"
Reading File
Searching PubMed
"synovial sarcoma" AND "ifosfamide" AND "treatment outcome"
Searching the Web
synovial sarcoma NCCN ESMO guidelines 2024 2025 treatment radiation dose proximal extremity
Reading File
Reading Web Page
https://www.dmcg.dk/siteassets/kliniske-retningslinjer/opdel…
Reading File
Reading File
Loading Image
Loading Image
Synovial Sarcoma - Right Proximal Arm
A Comprehensive Clinical Review (NCCN/ESMO 2025 Guidelines)
1. Overview & Nomenclature
Synovial sarcoma (SS) accounts for approximately 6-10% of all soft tissue sarcomas (STS). Despite the name, it does NOT arise from synovium - fewer than 10% are intra-articular. The name reflects the histologic resemblance to developing synovial joints, with cleft-like spaces simulating a microscopic "joint space." The proximal arm (humerus region) is an upper extremity location; approximately 60-70% of SS arise in the extremities. (Firestein & Kelley's Textbook of Rheumatology)
2. Pathophysiology
Cell of Origin
The cell of origin is an immature mesenchymal progenitor cell or myoblast - not from synovial lining cells (which do not express keratin, unlike SS cells). (Firestein & Kelley's)
Molecular Hallmark - t(X;18)(p11.2;q11.2)
This is the defining cytogenetic event - present in virtually 100% of cases:
| Translocation | Result | Frequency |
|---|---|---|
| t(X;18)(p11.2;q11.2) | SS18::SSX1 fusion | ~65% (biphasic type) |
| t(X;18)(p11.2;q11.2) | SS18::SSX2 fusion | ~35% (monophasic type) |
| t(X;18)(p11.2;q11.2) | SS18::SSX4 fusion | Rare |
Mechanism: SS18 is a subunit of the SWI/SNF chromatin remodeling complex. Fusion with SSX (which carries C-terminal repression domains) disrupts:
- Epigenetic control via SWI/SNF and histone deacetylase (HDAC)-associated mechanisms
- Normal transcription regulation → aberrant gene expression → oncogenesis
- The chimeric proteins also interfere with normal chromatin remodeling and dysregulate gene expression globally (Robbins & Kumar Basic Pathology)
This genetic event is the only consistent cytogenetic abnormality in SS; the genome is otherwise relatively stable with few additional mutations. (Firestein & Kelley's)
3. Clinical Features
Demographics
- Age: Most common in adolescents and young adults (median age ~34 years; range 9-74 years); occurs with significant frequency in children
- Sex: Slight male predominance
- Site: Right proximal arm - typically in deep soft tissues near the shoulder joint, in the vicinity of tendon sheaths, joint capsules, or along neurovascular bundles
Presentation
- Slowly enlarging, deep-seated, palpable mass - often present for months to years before diagnosis (this frequently leads to misdiagnosis as benign)
- Pain or tenderness in approximately 50-60% of patients (often mild initially)
- Restricted range of motion at the shoulder if large
- Rarely: a rapidly enlarging mass in younger patients (<30 years)
- The mass may wrap around the neurovascular bundle of the proximal arm (brachial vessels, median/ulnar/radial nerve)
Key Point
"No clinical features specific to synovial sarcoma distinguish it from other sarcomas." - the presentation is non-specific. Long duration of symptoms (sometimes years) before diagnosis is characteristic. (Firestein & Kelley's)
4. Histopathology
Gross
- Well-demarcated, pink-tan, fleshy mass
- The tumor "shells out" easily from its bed (pseudocapsule - do NOT mistake this for a benign lesion)
- Cut surface: gray-yellow, rubbery; calcified areas are gritty
- Larger tumors: areas of hemorrhage, necrosis, cystification
Microscopic Subtypes
1. Biphasic (Classic)
- Two distinct components:
- Epithelial cells forming glands, nests, or lining cyst-like spaces (cuboidal to columnar)
- Spindle cells in short, tightly packed fascicles with scant cytoplasm and dense chromatin
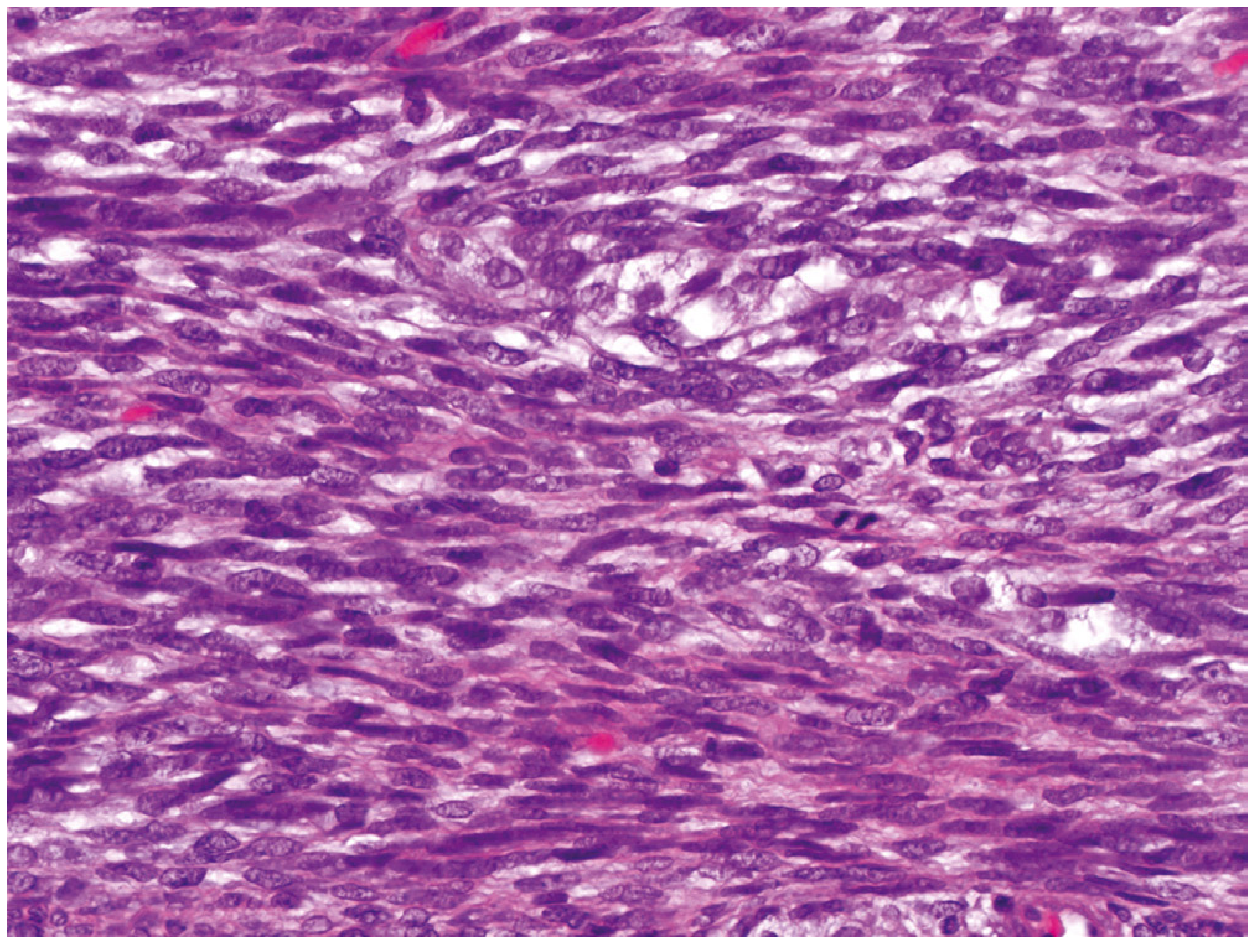
2. Monophasic (Spindle cell) - most common
- Only spindle cell component
- Cells in a herringbone pattern (see histology image below)
3. Monophasic Epithelial - exceptionally rare
4. Poorly Differentiated
- Small round/oval cells that may have rhabdoid morphology
- Most aggressive subtype; worst prognosis
Immunohistochemistry (IHC)
| Marker | Result | Significance |
|---|---|---|
| Keratin (AE1/AE3, CAM5.2) | Positive | Distinguishes from other spindle cell sarcomas |
| EMA (Epithelial Membrane Antigen) | Positive | Especially in biphasic type |
| TLE-1 | Diffusely strongly positive | Highly sensitive (but not specific) for SS |
| SS18::SSX fusion antibody | Positive | Can replace molecular testing |
| S-100 | Negative | Helps exclude MPNST |
| Desmin | Negative | Helps exclude rhabdomyosarcoma |
(Miller's Review of Orthopaedics 9th Edition; Firestein & Kelley's)
All synovial sarcomas are considered high-grade tumors. (Fischer's Mastery of Surgery)
5. Investigations
A. Imaging
Plain Radiograph (X-ray)
- Well-circumscribed deep soft tissue mass adjacent to proximal humerus
- Calcification in 30-50% - may be fine, stippled, focal, or dense (SS is one of few STS that frequently calcify)
- Periosteal reaction of adjacent humerus in ~20% of cases
- Frank bone invasion is rare
CT Scan
- More sensitive than X-ray for detecting calcification and periosteal reaction
- Shows intratumoral calcification clearly
- Used for chest CT - to stage pulmonary metastases (most common metastatic site)
MRI (Modality of Choice)
- Essential for delineating anatomic extent and surgical planning
- Shows a large, inhomogeneous mass with areas of hemorrhage
- "Triple signal" on T2 (seen in ~35%): areas of high, iso, and low intensity relative to fat - indicating cystic/hemorrhagic elements, fibrous tissue/calcification, and solid non-necrotic tumor
- Fluid-fluid levels (~18%)
- Evidence of hemorrhage (~44%)
- Bone erosion or invasion (~21%)
- Important: SS may appear small, homogeneous, and slow-growing on MRI - leading to frequent misdiagnosis as benign tumor

(Grainger & Allison's Diagnostic Radiology; Firestein & Kelley's)
PET-CT
- Useful for staging (detect distant metastases and lymph node involvement)
- Guides biopsy site (metabolically active area)
Ultrasound
- Can guide biopsy; may show internal vascularity
B. Biopsy
Core Needle Biopsy - preferred initial tissue diagnosis
- Must be performed along a planned surgical excision tract (the biopsy tract must be excised en bloc at definitive surgery)
- Incisional biopsy if core biopsy non-diagnostic
- Excisional biopsy should NOT be performed for masses >3 cm (risk of contamination)
C. Pathology Work-up
- H&E morphology
- Full IHC panel (keratin, EMA, TLE-1, S100, desmin, CD34)
- FISH or RT-PCR for SS18::SSX translocation (confirmatory)
- Next-generation sequencing (NGS) panel in selected cases
D. Staging Work-up
- Chest CT - pulmonary metastases
- MRI of primary site (if not already done)
- Bone scan if bone involvement suspected
- Regional lymph node assessment (SS has higher lymph node metastasis rate than most STS ~4-10%)
- Baseline labs: CBC, CMP, LFTs (pre-chemotherapy)
E. Staging System
AJCC 8th Edition (for soft tissue sarcomas):
- Stage IA: T1 (≤5 cm), G1/GX, N0, M0
- Stage IB: T2-T4 (>5 cm), G1/GX, N0, M0
- Stage II: T1, G2/G3, N0, M0
- Stage IIIA: T2, G2/G3, N0, M0
- Stage IIIB: T3-T4, G2/G3, N0, M0
- Stage IV: Any T, any G, N1 or M1
6. Management
Multidisciplinary Team (MDT) Approach - MANDATORY per NCCN/ESMO 2025
All patients should be discussed at a sarcoma MDT including surgical oncology, medical oncology, radiation oncology, pathology, and radiology at a sarcoma referral center.
A. Surgery - Cornerstone of Treatment
Goal: Wide surgical resection (R0 margins)
- Limb-sparing surgery (LSS) is the standard for proximal arm SS
- Wide local excision with negative margins (≥1 cm or an intact fascial plane)
- En bloc removal of biopsy tract
- Amputation is reserved for cases where LSS would result in a non-functional extremity or cannot achieve negative margins
For Right Proximal Arm:
- Resection of the tumor with surrounding soft tissue (deltoid, biceps, triceps heads as needed)
- Brachial neurovascular bundle: attempted preservation if tumor not adherent
- Proximal humerus resection with endoprosthetic reconstruction if bone involved
- Functional reconstruction planning (rotator cuff, shoulder mechanics)
Re-excision: If initial excision was intralesional (shelled out without adequate margins - a common scenario given the pseudocapsule), re-excision is strongly recommended before adjuvant therapy
B. Chemotherapy
SS is uniquely chemosensitive among soft tissue sarcomas - chemotherapy has demonstrated clinical benefit, unlike most other STS histotypes. (Miller's Review of Orthopaedics; Fischer's Mastery of Surgery)
First-Line (Neoadjuvant/Adjuvant):
| Regimen | Agents | Indication |
|---|---|---|
| AI regimen | Doxorubicin + Ifosfamide + Mesna | High-risk (>5 cm, deep, high-grade) - preferred |
| AD regimen | Doxorubicin alone | Alternative if ifosfamide contraindicated |
| Ifosfamide + Etoposide | Second-line or alternative |
Neoadjuvant chemotherapy rationale for proximal arm:
- Assess tumor response
- Attempt tumor downsizing to facilitate LSS
- Early treatment of micrometastases
- Particularly valuable for large tumors (>5 cm)
Adjuvant chemotherapy: Recommended for high-risk patients (tumors >5 cm). (Firestein & Kelley's)
For Advanced/Metastatic Disease (NCCN 2025 Update):
- Afami-cel (Afamitresgene autoleucel) - a T-cell receptor (TCR) therapy targeting MAGE-A4 antigen
- Approved for HLA-A*02-positive patients with SS expressing MAGE-A4, following progression on anthracycline/ifosfamide-based therapy
- Phase II trial showed durable responses - added to NCCN 2025 STS Guidelines
- Pazopanib, trabectedin (second-line options)
C. Radiation Therapy (RT)
Radiation is a key component of limb-sparing treatment. Per the DSG/ESMO radiotherapy guidelines:
Equipment
- Megavoltage equipment (4-20 MV linear accelerator)
- For extremity tumors (including proximal arm): photons of 4-6 MV are recommended
- IMRT (Intensity-Modulated Radiation Therapy) or 3D-conformal RT
Timing: Pre-operative vs Post-operative
| Feature | Pre-operative RT | Post-operative RT |
|---|---|---|
| Dose | 50 Gy | 60-66 Gy |
| Field size | Smaller (treats less tissue) | Larger (treats surgical bed) |
| Wound healing | Increased complication risk | Less wound risk |
| Local control | Equivalent | Equivalent |
| Late toxicity | LESS (lower dose, smaller field) | MORE |
Pre-operative RT is generally preferred for large, high-grade proximal extremity sarcomas per ESMO/NCCN because it results in smaller radiation fields, lower doses, and equivalent tumor control.
Dose Fractionation for Synovial Sarcoma (Adults)
Conventional fractionation: 1.8 Gy/day, 5 days/week
| Setting | Total Dose | Notes |
|---|---|---|
| Post-op R0 (clear margins) | 50-54 Gy | Standard post-op dose |
| Post-op R1 (microscopically +) | 54-60 Gy | Boost to margin area |
| Post-op R2 (grossly +) | 66 Gy | Boost required |
| Pre-operative | 50 Gy (1.8 Gy/fractions) | Then surgery |
| Unresectable / definitive | 59.4-66 Gy |
For the proximal arm specifically:
- Fractionation: 1.8 Gy/day, 5 days/week
- Total dose: 50.4-60 Gy depending on margin status (post-op) or 50 Gy pre-op
- Boost on smaller volume to residual/at-risk areas: typically 10-16 Gy additional
- A longitudinal strip of uninvolved skin/subcutaneous tissue should be spared to prevent lymphedema
- Humeral head and shoulder joint: attempt to keep mean dose <45 Gy if possible
Brachytherapy (low-dose-rate, LDR): can be used as monotherapy or to boost the surgical bed. The total dose calculation must account for radiation tolerance of adjacent tissue.
Start Time
- Post-operative RT should begin within 21 days of surgery (unless postoperative complications)
- Treatment planning: 3D-conformal RT planning recommended when critical structures lie in the target volume (brachial plexus, humeral head)
7. Prognosis
Survival Data
| Time Point | Disease-Free Survival (Localized) |
|---|---|
| 5-year | 59% |
| 10-year | 52% |
| 15-year | 52% |
- Localized disease: 5-year overall survival 40-90.7% (wide range based on risk factors)
- Metastatic disease: 5-year overall survival ~10%
(Firestein & Kelley's Textbook of Rheumatology - citing series of 150 patients and systematic review)
Prognostic Factors
| Factor | Better Prognosis | Worse Prognosis |
|---|---|---|
| Tumor size | < 5 cm | ≥ 5 cm |
| Patient age | < 25 years (esp. <16 yrs) | ≥ 25 years |
| Histology | Biphasic or monophasic | Poorly differentiated component |
| Calcification | Heavily mineralized/ossified | No calcification |
| Margins | R0 (negative) | R1/R2 |
| Stage | Localized | Metastatic |
| Fusion type | SS18::SSX2 (better) | SS18::SSX1 (slightly worse) |
Note: Pediatric patients (<16 years) have improved prognosis despite similar tumor size, site, grade, and location compared to adults.
8. Natural History & Complications
Pattern of Recurrence
- Local recurrence: May be repetitive
- Most recurrences manifest within 2 years of initial treatment (but intervals >10 years are documented)
- Metastases occur in 50-70% of patients ultimately
Sites of Metastasis
| Site | Frequency |
|---|---|
| Lung | 80% (most common) |
| Bone | 10% |
| Liver | 5% |
| Regional lymph nodes | ~4-10% (higher than other STS - important to evaluate) |
- ~10% of patients die within 1 year of metastatic diagnosis (usually from massive pulmonary metastases)
Treatment-Related Complications
| Complication | Cause | Management |
|---|---|---|
| Wound healing delay | Pre-op RT (major concern) | Close monitoring, wound care |
| Lymphedema of arm | RT/surgery to axillary region | Sparing of skin strip; compression |
| Radiation fibrosis | High-dose RT to soft tissue | PT/OT, pentoxifylline |
| Brachial plexopathy | RT dose to brachial plexus | Limit plexus dose <60 Gy |
| Radiation-induced fracture (proximal humerus) | Bone irradiation | Bisphosphonates, orthopaedic f/u |
| Shoulder dysfunction/stiffness | Surgery + RT to rotator cuff | Early physiotherapy |
| Post-operative hematoma/seroma | Surgery | Drain management |
| Local recurrence | Inadequate margins | Re-resection ± re-irradiation |
| Chemotherapy toxicity | Doxorubicin: cardiotoxicity; Ifosfamide: hemorrhagic cystitis, encephalopathy | Echocardiography monitoring; Mesna co-administration; hydration |
| Distant metastases (lung) | Hematogenous spread | Metastasectomy if resectable; chemotherapy |
| Secondary lymph node metastasis | Lymphatic spread | Nodal evaluation; regional RT if involved |
9. Follow-up Protocol (NCCN/ESMO Standard)
Years 1-2 (High-risk period):
- Clinical examination + chest imaging every 3-6 months
- MRI of primary site every 3-6 months
Years 3-5:
- Clinical examination + chest imaging every 6 months
- MRI of primary site every 6 months
Beyond 5 years:
- Annual chest X-ray/CT and clinical exam
- (Note: late recurrences >10 years are documented in SS - hence long-term follow-up)
Sources
- Firestein & Kelley's Textbook of Rheumatology (2-Volume Set), Chapter 129 - Synovial Sarcoma
- Robbins & Kumar Basic Pathology, Chapter 19 - Soft Tissue Tumors
- Miller's Review of Orthopaedics, 9th Edition, Chapter 5 - Musculoskeletal Tumors
- Fischer's Mastery of Surgery, 8th Edition - Retroperitoneal/Soft Tissue Sarcoma
- Grainger & Allison's Diagnostic Radiology - Soft Tissue Masses
- NCCN Clinical Guidelines - Soft Tissue Sarcoma, Version 1.2025 (includes afami-cel update for synovial sarcoma)
- DSG/ESMO Radiotherapy Guidelines for Localized Soft Tissue Sarcoma (v1.3, 2025) - conventional fractionation and dose recommendations
- ESMO-EURACAN-GENTURIS Clinical Practice Guidelines, Annals of Oncology 2021;32(11):1348-1365
This is a shared conversation. Sign in to Orris to start your own chat.