Control zones of a chemical event
Reading File
Searching the Web
chemical incident control zones hot warm cold zone emergency response
Finding Sources
Finding Sources
Reading File
Loading Image
Reading File
Here is a detailed breakdown of the control zones of a chemical event, sourced directly from Tintinalli's Emergency Medicine (Figure 8-1):
Control Zones of a Chemical Event
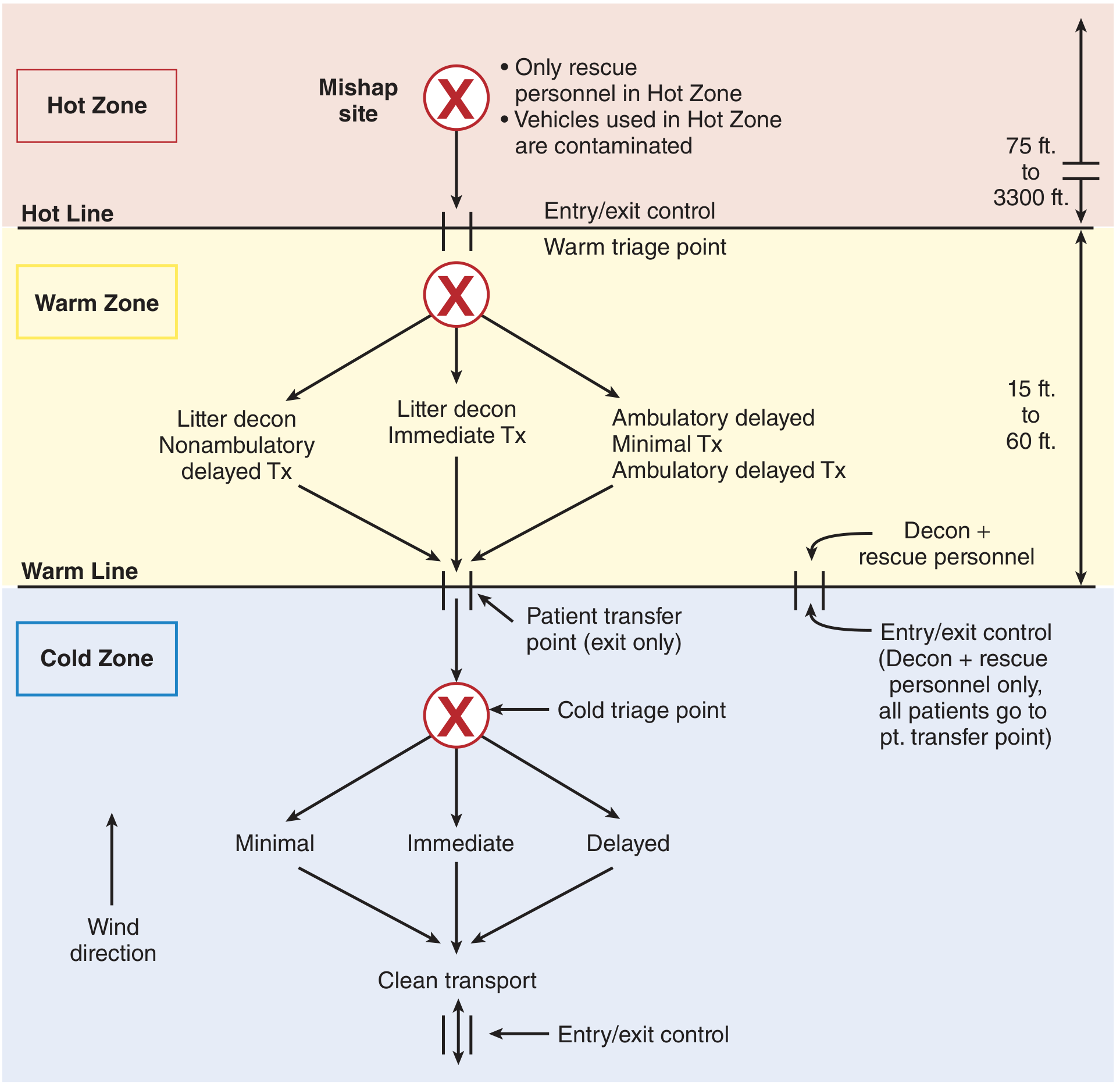
Figure 8-1 from Tintinalli's Emergency Medicine - Control zones of a chemical event
When a chemical release occurs, the EMS incident command system divides the scene into three concentric zones. Each zone has defined boundaries (the hot line and warm line), strict access rules, and specific operational roles.
1. Hot Zone (Red Zone / Exclusion Zone)
- Location: The immediate area surrounding the mishap site where primary contamination occurs
- Distance: Extends 75 ft to 3,300 ft from the release source depending on the agent and conditions
- Access: Only trained rescue personnel in fully encapsulated protective gear (Level A PPE)
- Key rule: Vehicles used in the hot zone are considered contaminated
- Activities:
- Victim rescue and removal from the contaminated environment
- Site characterization and hazard monitoring
- Controlling and confining the release
- What is NOT done here: Decontamination or definitive patient care
- The hot line marks the boundary between the hot and warm zones, with a formal entry/exit control point
2. Warm Zone (Yellow Zone / Contamination Reduction Zone)
- Location: A surrounding corridor just outside the hot zone
- Distance: 15 ft to 60 ft wide
- Access: Decontamination and rescue personnel only; patients exit through the patient transfer point
- Activities:
- Decontamination - the primary function: remove clothing, brush off solids, wash with warm water for at least 5 minutes
- Warm triage point at the hot line entry to sort incoming casualties
- Three decontamination lanes based on patient status:
- Litter decon + immediate treatment (most critical)
- Litter decon + nonambulatory delayed treatment
- Ambulatory delayed / minimal treatment
- Basic airway management may occur simultaneously with decon
- Decon agent: Water is the universal agent; plain warm water is adequate for most agents
- The warm line marks the boundary between the warm and cold zones
3. Cold Zone (Blue Zone / Support Zone / Green Zone)
- Location: Beyond the warm line, upwind and uphill from the hot zone
- Access: Open to unprotected medical personnel once patients are fully decontaminated
- Activities:
- Cold triage point: Secondary triage into Minimal, Immediate, and Delayed categories
- Full stabilization and advanced medical care
- Antidote administration (e.g., atropine/pralidoxime for organophosphates)
- Airway management, oxygen, bronchodilators, IV access
- Clean transport to hospital
- Incident command center is based here
- Key rule: The cold zone must be positioned upwind (and uphill if applicable) from the hot zone to prevent vapor drift contamination
Key Operational Principles
| Feature | Hot Zone | Warm Zone | Cold Zone |
|---|---|---|---|
| Color code | Red | Yellow | Blue/Green |
| Contamination risk | High | Intermediate | None |
| PPE required | Level A (full encapsulation) | Level B/C | Minimal or none |
| Primary function | Rescue | Decontamination | Treatment & triage |
| Patient care | Evacuation only | Basic airway/decon | Full stabilization |
| Personnel | HazMat/rescue teams | Decon teams | Medical personnel |
Secondary Contamination - Key Concern
Rescuers who enter the hot zone without proper gear risk secondary contamination - absorbing the chemical through contact with victims or the environment. Organophosphates in particular can be excreted in sweat and adhere to leather items (shoes, belts, holsters), which must be discarded and cannot be effectively decontaminated.
Source: Tintinalli's Emergency Medicine: A Comprehensive Study Guide, Chapter 8 - Isolation and Scene Control (pp. 78-79)
Explain me the warm zone
Reading File
Here is a full explanation of the warm zone from Tintinalli's Emergency Medicine, Chapter 8:
The Warm Zone - Detailed Explanation
The warm zone is the contamination reduction corridor - a buffer strip that physically and operationally separates the hot (contaminated) zone from the cold (clean) zone. Its entire purpose is to reduce contamination to a safe level before any patient or personnel crosses into the cold zone.
Physical Layout
- Sits between the hot line (inner boundary) and the warm line (outer boundary)
- Width: 15 to 60 feet
- Entry and exit for personnel is controlled at the warm line on the side
- Patients exit only through the patient transfer point at the warm line - they do not share the same entry/exit as personnel
Who Enters the Warm Zone
Only decontamination and rescue personnel wearing appropriate PPE (Level B or C protection) may enter. All patients pass through this zone after being brought out of the hot zone but before receiving full medical care. No unprotected bystanders or general medical staff are permitted.
What Happens Here
1. Warm Triage Point
At the hot line entry, incoming casualties are rapidly sorted into three lanes based on their condition:
| Lane | Patient Type | Action |
|---|---|---|
| Left | Litter (nonambulatory) - delayed treatment | Decontamination, then delayed Tx |
| Centre | Litter (nonambulatory) - immediate treatment | Decontamination + immediate Tx simultaneously |
| Right | Ambulatory - delayed or minimal treatment | Walk-through decontamination |
2. Decontamination - The Core Function
Decontamination is the most critical management step in the warm zone. Steps in order:
- Remove clothing - this alone eliminates up to 80% of contamination
- Brush off solid particles from skin and hair
- Wash the face and towel dry
- Hose down with warm water for a minimum of 5 minutes (warm water is specifically used to prevent shivering, which would otherwise keep victims outdoors longer and worsen hypothermia)
Decontamination agent: Plain water is the universal agent. Some guidelines recommend dilute household bleach for nerve agents and vesicants, but there is little evidence it outperforms water, and bleach is rarely available in sufficient quantity at the scene.
Special attention areas where fluids hide:
- Hair
- Skin folds
- Axillae
- Groin
- Between toes
- Eyes
3. Simultaneous Basic Treatment (when needed)
For patients with severe symptoms, full decontamination and basic treatment run at the same time - decon is not delayed waiting for treatment. Basic interventions that may begin in the warm zone include:
- Opening an obstructed airway
- Positioning
Definitive treatment, IV lines, antidotes, and advanced care are held for the cold zone.
Contamination Types Managed Here
| Type | Description |
|---|---|
| Primary contamination | Direct contact with the released substance - what patients arrive with |
| Secondary contamination | Transfer of the agent from a contaminated patient to a rescuer or piece of equipment |
Secondary contamination is the key hazard in the warm zone. It can affect:
- Rescuers who touch wet contaminated skin without PPE
- Equipment as small as a stethoscope or as large as a fire truck (taken out of service until decontaminated)
- Organophosphates specifically - they are excreted in sweat and adhere to leather; shoes, belts, and holsters of first responders must be discarded, not just washed
Why the Warm Zone Matters
Without an effective warm zone:
- Contaminated patients would carry the agent directly into the cold zone
- Medical staff treating patients would suffer secondary contamination
- The chemical hazard would spread beyond the incident perimeter
- Vehicles and equipment would become contamination vectors
The warm zone is the only point at which the chain of contamination can be broken before the patient reaches definitive care.
Source: Tintinalli's Emergency Medicine: A Comprehensive Study Guide, "Decontamination in the Warm Zone," p. 78-79
This is a shared conversation. Sign in to Orris to start your own chat.