plummer Vinson syndrome in detail for 20 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
"Plummer-Vinson syndrome" OR "Paterson-Kelly syndrome"
PMID: 40802140
PMID: 38345572
PMID: 34651287
PMID: 38678196
Plummer Vinson syndrome RGUHS ENT 20 marks pathogenesis treatment recent advances 2024
https://www.ncbi.nlm.nih.gov/books/NBK538306
Medical diagram showing Plummer-Vinson syndrome pathophysiology flowchart. Include: Iron deficiency anemia at top leading down through arrows to: iron-dependent enzyme dysfunction, oxidative stress, mucosal atrophy, esophageal web formation, postcricoid dysphagia. Also show associated features branching out: koilonychia (spoon nails), glossitis, angular cheilitis, atrophic gastritis. Bottom box shows risk of squamous cell carcinoma (3-15%). Use clean medical illustration style with blue and red color scheme, labeled boxes and connecting arrows.
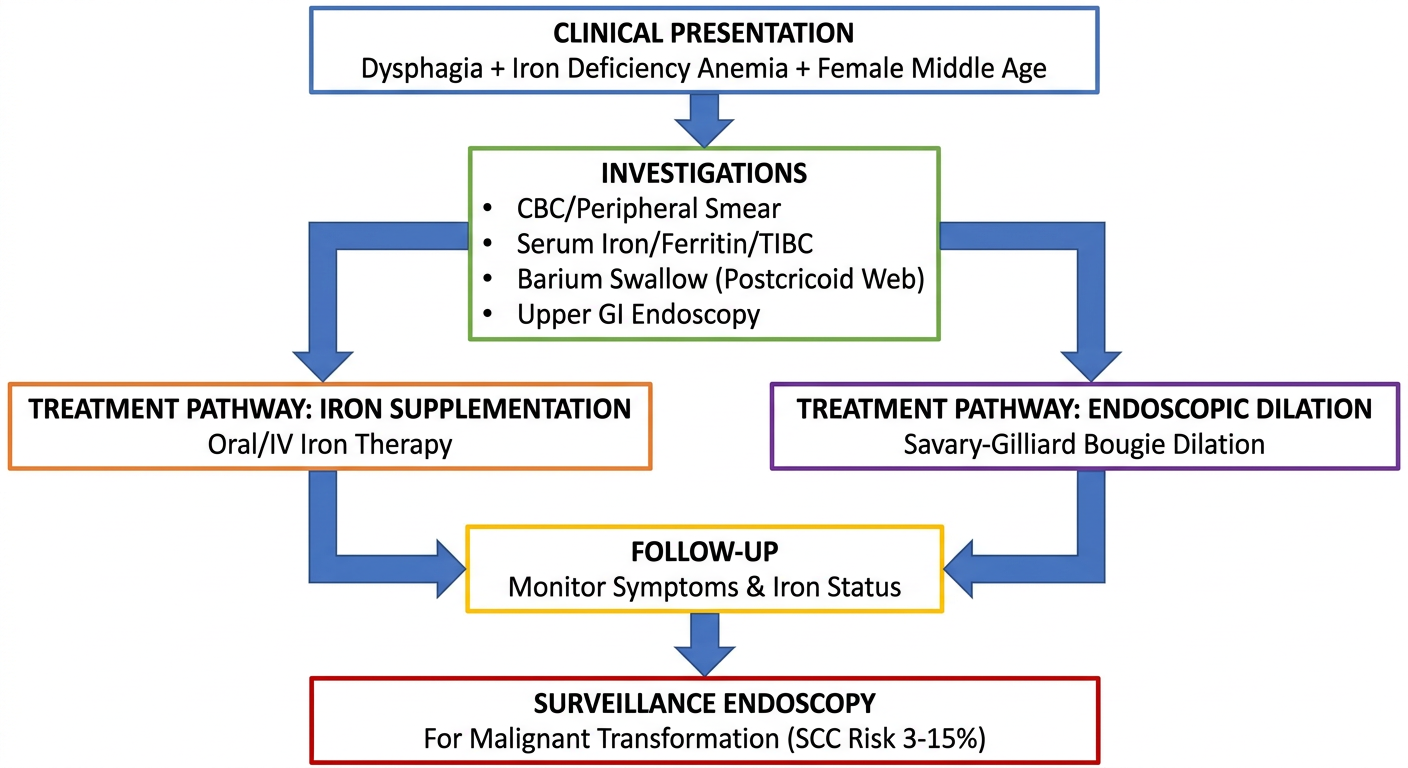
Medical flowchart for management of Plummer-Vinson syndrome. Start with clinical presentation box (dysphagia + iron deficiency anemia + female middle age). Flow down to investigations: CBC/peripheral smear, serum iron/ferritin/TIBC, barium swallow showing postcricoid web, upper GI endoscopy. Then treatment pathway: iron supplementation (oral/IV) on left branch, endoscopic dilation with Savary-Gilliard bougie on right branch. Both merge to follow-up box. At bottom: surveillance endoscopy for malignant transformation (SCC risk 3-15%). Clean medical diagram, white background, professional style with labeled boxes.
Anatomical diagram showing location of esophageal web in Plummer-Vinson syndrome. Show sagittal cross-section of head and neck with pharynx, larynx, cricopharyngeal muscle, upper esophagus clearly labeled. Highlight the postcricoid/anterior upper esophageal web as a thin mucosal shelf protruding from the anterior wall, just below the cricopharyngeal muscle. Arrows indicating the narrowed lumen. Also show barium swallow appearance with web visible as thin horizontal shelf. Medical textbook illustration style, clean anatomical labels.
PLUMMER-VINSON SYNDROME (20 Marks)
1. INTRODUCTION AND HISTORICAL BACKGROUND
- Henry Stanley Plummer (1874-1936) and Porter Paisley Vinson (1890-1959) at the Mayo Clinic (USA)
- Donald Ross Paterson (1863-1939) and Adam Brown-Kelly (1865-1941) in the UK - who published their findings in 1919
- Post-cricoid dysphagia
- Iron deficiency anemia
- Esophageal (pharyngeal/postcricoid) webs
"Patterson-Brown-Kelly syndrome is the association of dysphagia with atrophic gastritis and iron-deficiency anaemia." - Scott-Brown's Otorhinolaryngology Head & Neck Surgery
2. EPIDEMIOLOGY
| Parameter | Details |
|---|---|
| Sex | Predominantly females (F:M = 10:1); 80-85% female (Cummings) |
| Age | 4th-7th decade (40-70 years), middle-aged women |
| Geography | Higher prevalence in Scandinavian countries, USA, Wales |
| Racial predilection | Predominantly Caucasian (Scandinavian descent) |
| Trend | Declining incidence due to improved nutrition and prenatal care |
"Improved nutrition and better prenatal care have resulted in a decline in the incidence of postcricoid carcinomas in Sweden." - Cummings Otolaryngology
3. PATHOGENESIS / ETIOLOGY
Pathophysiology Flowchart:
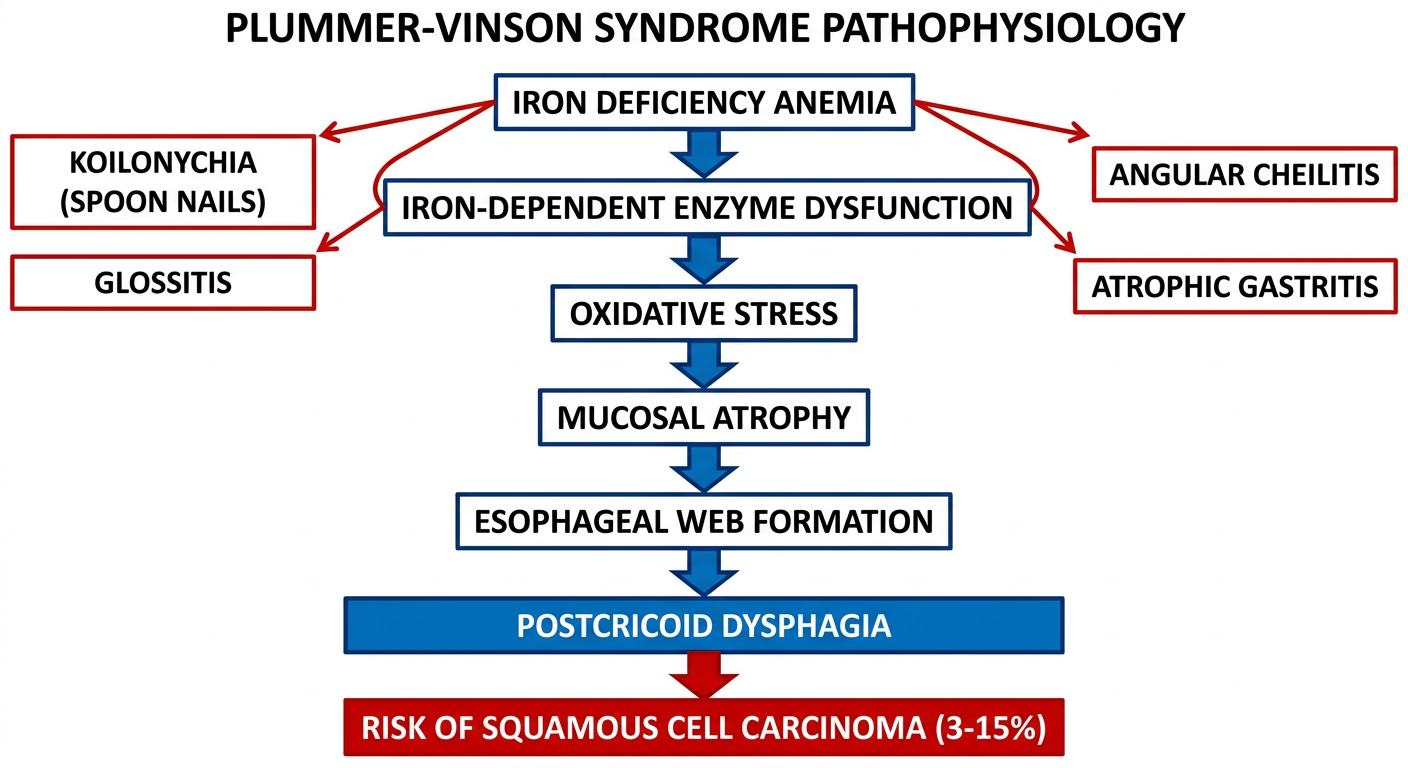
- Iron deficiency → dysfunction of iron-dependent oxidative enzymes (cytochrome oxidase)
- Enzyme dysfunction → oxidative stress and DNA damage
- Malfunctioning iron-dependent enzymes → myasthenic changes in swallowing muscles
- Atrophy of esophageal mucosa → epithelial complications
- Repeated epithelial injury → web formation in the postcricoid / upper esophageal region
- Web acts as a mechanical barrier → progressive dysphagia
- Genetic predisposition
- Autoimmune mechanisms (association with Sjogren syndrome, rheumatoid arthritis, thyroid disease, celiac disease)
- Nutritional deficiencies (riboflavin, iron)
- Possible relationship with GERD (KJ Lee)
- Chronic mucosal irritation
"Iron deficiency anemia is the most accepted causal association. The pathogenesis of this syndrome is poorly understood." - Yamada's Textbook of Gastroenterology
4. ANATOMY OF THE WEB
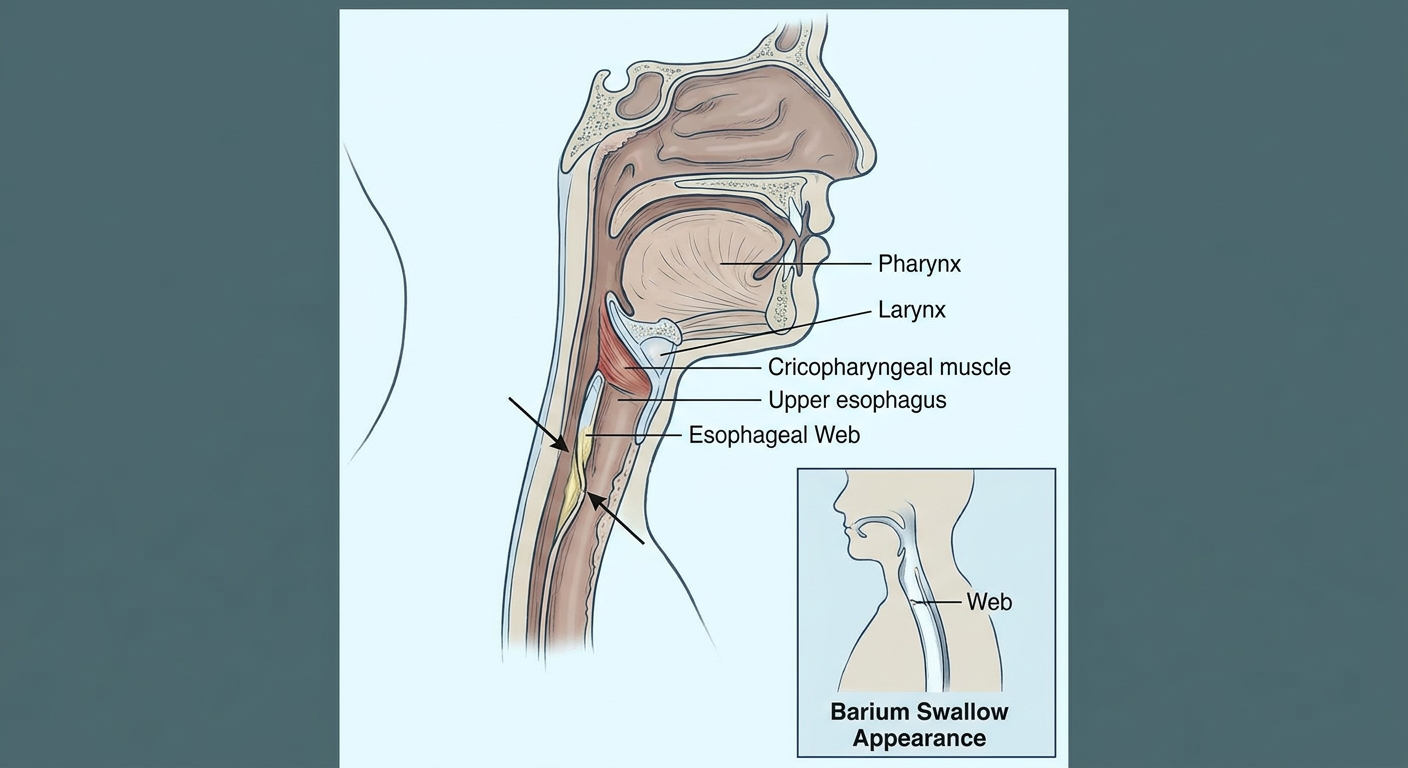
- The web is a thin mucosal shelf composed of mucosa and submucosa
- Located in the postcricoid region / anterior wall of the upper esophagus, just below the cricopharyngeal muscle
- Most commonly attached asymmetrically to the anterior wall
- The web forms an eccentric or central lumen
- Dysphagia typically occurs when luminal diameter becomes less than 12 mm (Yamada)
- Appears as smooth, thin, gray lesions on endoscopy
5. CLINICAL FEATURES
5.1 Classic Triad (Diagnostic Triad)
- Dysphagia - progressive, initially for solids, high (postcricoid level), may be intermittent; develops slowly
- Iron deficiency anemia - microcytic hypochromic anemia; mean Hb ~8.2 g/dL
- Postcricoid / upper esophageal webs - on anterior wall, best seen on videofluoroscopy
5.2 Associated Features (From Multiple Sources)
| System | Features |
|---|---|
| Oral | Angular cheilitis (cheilosis), angular stomatitis |
| Tongue | Glossitis - erythematous plaques, loss of fungiform papillae, smooth/atrophic tongue |
| Nails | Koilonychia - spoon-shaped, brittle fingernails |
| Gastric | Atrophic gastritis, achlorhydria |
| Constitutional | Lassitude, poor exercise tolerance |
| Skin | Dryness, pallor |
| Hormonal | Hypothyroidism (associated) |
| ENT | Hoarseness, pharyngitis, esophagitis |
"Other features of iron deficiency anaemia - smooth tongue, angular stomatitis and koilonychias - may be seen." - Scott-Brown's
"Koilonychia describes a nail abnormality whereby fingernails or toenails are spoon-shaped and brittle. Glossitis presents as erythematous plaques of the tongue, sometimes with loss of fungiform papillae. Angular stomatitis (perleche) describes scale, erythema, and fissuring at the oral commissures." - Yamada's Gastroenterology
6. DIAGNOSIS
Investigative Flow:
6.1 Hematological Investigations
- Complete Blood Count (CBC): Microcytic hypochromic anemia
- Peripheral smear: Hypochromic, microcytic RBCs, pencil cells
- Serum iron: Reduced
- Serum ferritin: Reduced (mean ~10 ng/mL in multicenter study)
- Total Iron Binding Capacity (TIBC): Elevated
- Transferrin saturation: Reduced
"Diagnosis: barium esophagram; check CBC, serum iron, ferritin levels." - KJ Lee's Essential Otolaryngology
6.2 Radiological
- Barium swallow / Videofluoroscopy (Gold Standard for web):
- Demonstrates thin horizontal shelf on anterior wall
- Eccentric/asymmetric filling defect in upper esophagus
- Best diagnostic test (KJ Lee)
- May appear as a subtle indentation on lateral view
6.3 Endoscopy (Upper GI Endoscopy/Esophagoscopy)
- Webs appear as smooth, thin, gray lesions with eccentric/central lumen
- Located most commonly on anterior wall
- Caution: Webs may be accidentally ruptured during passage of endoscope (Yamada)
- Endoscope must be introduced under direct visualization
- Mandatory to rule out postcricoid carcinoma
6.4 Additional Tests
- Thyroid function tests (TFT) - associated hypothyroidism
- Anti-tissue transglutaminase antibody (rule out celiac disease)
- Autoimmune workup (ANA, anti-Ro/SS-A for Sjogren syndrome association)
7. DIFFERENTIAL DIAGNOSIS
| Condition | Differentiating Features |
|---|---|
| Zenker's Diverticulum | Regurgitation of undigested food, bad breath, posterior wall |
| Carcinoma of Esophagus | Progressive, alarming features; biopsy distinguishes |
| Achalasia | Both solids and liquids affected, bird-beak sign on barium |
| Pernicious Anemia | Megaloblastic (not microcytic), neurological symptoms, intrinsic factor absent |
| Folic Acid Deficiency | Megaloblastic anemia, no neurological symptoms, no webs |
| Eosinophilic Esophagitis | Younger males, food bolus obstruction, >15 eosinophils/HPF |
| Pharyngeal pouch | Posterior, Killian's dehiscence, regurgitation |
"This disease is to be contrasted with pernicious anemia, which is a megaloblastic anemia with diarrhea, nausea and vomiting, neurologic symptoms, enlarged spleen, and achlorhydria." - KJ Lee's
8. TREATMENT
8.1 Iron Supplementation (First-line)
- Oral iron (ferrous sulphate 200 mg TDS) - treatment of choice in mild-moderate cases
- Parenteral iron (IV iron sucrose) - for non-responders or severe anemia
- Iron supplementation alone can resolve dysphagia in many patients (Yamada)
- Resolves mucosal atrophy, cheilitis, glossitis, and koilonychia
- A rapid improvement in dysphagia and web after 2 weeks of iron therapy has been reported
8.2 Esophageal Dilation
- Indicated when: Dysphagia persists after iron correction, or web diameter < 12 mm
- Savary-Gilliard bougie dilators - used in 89% of cases (Alzamzamy et al., Dig Dis Sci 2025)
- Single dilation session is sufficient in 76.8% of patients (multicenter study, 2025)
- Rigid esophagoscopy: May accidentally rupture the web (therapeutic effect)
- Balloon dilation: alternative endoscopic approach
- In pediatric cases: Sequential dilation starting with smaller probes (5 mm, 7 mm, then 9 mm)
8.3 Dietary Advice
- Iron-rich diet
- Treat underlying malabsorption if present
8.4 Surveillance / Follow-up Endoscopy
- Mandatory due to risk of malignant transformation
- Regular surveillance endoscopy every 1-3 years
9. COMPLICATIONS AND PROGNOSIS
Malignant Transformation - KEY POINT FOR EXAMS
| Source | Risk Stated |
|---|---|
| Yamada's Gastroenterology | 3-15% develop squamous cell carcinoma |
| Cummings Otolaryngology | Associated with postcricoid and upper esophageal carcinoma |
| Scott-Brown's | "Small percentage develop postcricoid carcinoma" |
| Bailey & Love | Higher incidence of postcricoid malignancy |
- Type: Squamous cell carcinoma of hypopharynx (postcricoid region) / upper esophagus
- Mechanism: Chronic iron deficiency causes irreversible mucosal changes leading to malignant degeneration
- Monitoring: Close surveillance endoscopy is essential (PMID 40802140, 2025)
- Excellent with treatment - most patients need only one EGD session + iron therapy
- Koilonychia, glossitis, cheilitis resolve with iron supplementation
- No significant post-dilation complications reported in recent studies
10. RECENT ADVANCES (2021-2026)
10.1 Multicenter Study (Alzamzamy et al., Dig Dis Sci, 2025) [PMID: 40802140]
- 56 patients across 7 centers in Egypt, India, and Iraq (2021-2024)
- Mean age 41 years; 80.5% female
- Mean Hb 8.2 g/dL; mean ferritin 10.34 ng/mL
- Celiac disease most common associated condition (10.7%)
- Savary-Gilliard bougie dilators used in 89%
- Single dilation session sufficient in 76.8%
- 7.1% developed SCC/dysplasia on follow-up
10.2 Autoimmune Associations (de Carvalho & Lerner, Immunol Res, 2022) [PMID: 34651287]
- Sjogren syndrome association established - in Sjogren's, triad of iron-deficiency anemia + dysphagia + weight loss should trigger PVS evaluation
- Autoantibodies: ANA, anti-Ro/SS-A
- Parenteral iron in Sjogren's-PVS avoided need for dilation in 2/3 cases
- Suggests immune dysregulation as a contributing pathogenic mechanism
10.3 Pediatric PVS (Vohra et al., BMC Pediatrics, 2024) [PMID: 38678196]
- Rare occurrence in children - case in 1-year-old male
- Iron supplements increase Hb but may not resolve dysphagia - dilation still required
- Sequential Savary-Gilliard dilation effective and safe in pediatrics
10.4 Celiac Disease Association (Alfaris et al., Int Med Case Rep J, 2023) [PMID: 37501941]
- PVS possibly associated with celiac disease as underlying cause of iron malabsorption
- Screening for celiac disease recommended in PVS patients
10.5 NEJM Case Report (Binet & Delorme, NEJM, 2024) [PMID: 38345572]
- Classic case highlighted in the NEJM - brought renewed attention to this rare condition
10.6 Role of Serum Ferritin
- Serum ferritin emerging as a key diagnostic marker in PVS (JOAS, India)
- Low ferritin levels correlate with severity of web formation
11. SUMMARY TABLE (High-Yield for RGUHS)
| Feature | Details |
|---|---|
| Synonym | Paterson-Brown-Kelly (UK), Sideropenic dysphagia |
| Classic Triad | Dysphagia + Iron deficiency anemia + Esophageal web |
| Sex ratio | F:M = 10:1 |
| Age | 4th-7th decade |
| Web location | Anterior wall, postcricoid / upper esophagus |
| Best investigation for web | Barium swallow / Videofluoroscopy |
| Endoscopy | Smooth, thin, gray lesion; may rupture on scope entry |
| Primary treatment | Iron supplementation (resolves in many) |
| Dilation | Savary-Gilliard bougie; 76.8% respond to single session |
| Malignant risk | SCC of pharynx/esophagus in 3-15% |
| Key associated conditions | Hypothyroidism, celiac disease, Sjogren syndrome, RA |
| Prognosis | Excellent with treatment |
12. SOURCES CITED
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery - Patterson-Brown-Kelly Syndrome section
- Cummings Otolaryngology Head & Neck Surgery - Etiology and Biology, Hypopharyngeal Ca (p. 1906)
- KJ Lee's Essential Otolaryngology (9th/10th ed) - Plummer-Vinson Syndrome; Esophageal Webs
- Bailey & Love's Short Practice of Surgery 28th ed - Sideropenic Dysphagia section
- Yamada's Textbook of Gastroenterology, 7th ed - Plummer-Vinson Syndrome (pp. 2325, 2350)
- StatPearls/NCBI - Plummer-Vinson Syndrome (Verma & Mukherjee, 2026 update)
- Alzamzamy et al., Dig Dis Sci 2025 - Multicenter Study PMID 40802140
- de Carvalho & Lerner, Immunol Res 2022 - Sjogren's Association PMID 34651287
- Vohra et al., BMC Pediatrics 2024 - Pediatric PVS PMID 38678196
- Binet & Delorme, NEJM 2024 - Classic Case PMID 38345572
RGUHS EXAM TIPS (20 Marks Structure)
- Definition + History (1 mark)
- Epidemiology (1 mark)
- Pathogenesis with flowchart (3 marks)
- Clinical features/Triad (3 marks)
- Investigations with diagram (3 marks)
- Differential diagnosis (2 marks)
- Treatment (4 marks)
- Complications + Malignant risk (2 marks)
- Recent advances (1 mark)