Nephrotic syndrome
Reading File
Finding Sources
Searching PubMed
"nephrotic syndrome" management
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have comprehensive information. Let me compile the full, detailed response.
Nephrotic Syndrome
Definition
Nephrotic syndrome is defined as proteinuria >3.5 g/24 hours in adults, with serum albumin <3.5 g/dL, accompanied by hyperlipidemia and clinically apparent edema. A spot urine protein:creatinine ratio correlates with the 24-hour collection and can substitute for it in practice.
The unifying pathological mechanism is impairment of glomerular charge and size selectivity - normally maintained by the glomerular basement membrane (GBM), endothelial cells, and podocytes - resulting in massive protein loss into the urine.
- National Kidneys Foundation Primer on Kidney Diseases, 8e, p. 189
Etiology and Classification

Fig. 16.1 - Most common etiologies of nephrotic syndrome (NKF Primer on Kidney Diseases, 8e)
Primary (Glomerular) Causes
| Disease | Epidemiology | Key Features |
|---|---|---|
| Minimal Change Disease (MCD) | ~15% of adult NS; 70-90% of pediatric NS | Normal light microscopy; diffuse foot process effacement on EM |
| Focal Segmental Glomerulosclerosis (FSGS) | ~25% of adult NS; most common in African descent | Focal/segmental scarring; podocyte injury |
| Membranous Nephropathy (MN) | Most common cause of adult NS in whites; 4th-5th decade; M:F = 2:1 | Subepithelial immune deposits; anti-PLA2R antibodies in ~70% primary MN |
Secondary Causes
- Metabolic: Diabetic kidney disease (most common secondary cause globally), amyloidosis
- Autoimmune: Lupus nephritis (SLE), Henoch-Schonlein purpura
- Infections: Hepatitis B/C (associated with MN), HIV (collapsing FSGS), parvovirus B19
- Drugs: NSAIDs, heroin, pamidronate, interferon, gold salts
- Malignancy: Solid tumors (associated with MN), Hodgkin lymphoma (associated with MCD)
- Genetic: Mutations in podocyte genes - NPHS1 (nephrin), NPHS2 (podocin), ACTN4, APOL1
NKF Primer, pp. 189-192; Tietz Textbook of Laboratory Medicine, 7th Ed.
Pathophysiology
The glomerular filtration barrier has three components: the fenestrated endothelium, the GBM, and podocyte foot processes connected by slit diaphragms. In nephrotic syndrome, damage primarily targets the podocytes, leading to:
- Loss of charge selectivity - the GBM normally carries a net negative charge repelling albumin (also negatively charged). This is disrupted in NS.
- Foot process effacement - the hallmark on electron microscopy across all causes of primary NS.
- Massive proteinuria leading to all downstream consequences.
Edema mechanisms - two models:
- Underfill: Protein loss → hypoalbuminemia → reduced plasma oncotic pressure → fluid shifts to interstitium → low effective circulating volume → RAAS activation → sodium retention. Seen classically in MCD.
- Overfill: Primary renal sodium and water retention (independent of oncotic pressure) with expanded plasma volume and suppressed RAAS. Seen in most other causes.
Brenner and Rector's The Kidney, 2-Vol Set, p. 2277
Clinical Features
Symptoms: Peripheral edema (often anasarca), foamy urine, fatigue, dyspnea
Signs: Hypertension, generalized dependent pitting edema, ascites, pleural effusions. Less common: Muehrcke's lines (white transverse bands on nails due to hypoalbuminemia), eruptive xanthomata, xanthelasma.
Laboratory:
- Proteinuria >3.5 g/24 hr (or spot protein:creatinine ratio >3.5)
- Serum albumin <2.5-3.5 g/dL
- Hyperlipidemia (total cholesterol usually >180 mg/dL; elevated LDL, triglycerides)
- Lipiduria (oval fat bodies, "Maltese cross" under polarized light)
- Bland urinary sediment (minimal hematuria, unlike nephritic syndrome)
Frameworks for Internal Medicine; Tietz Laboratory Medicine, 7th Ed.
Complications
1. Hypercoagulability (10-40% develop thromboembolic events)
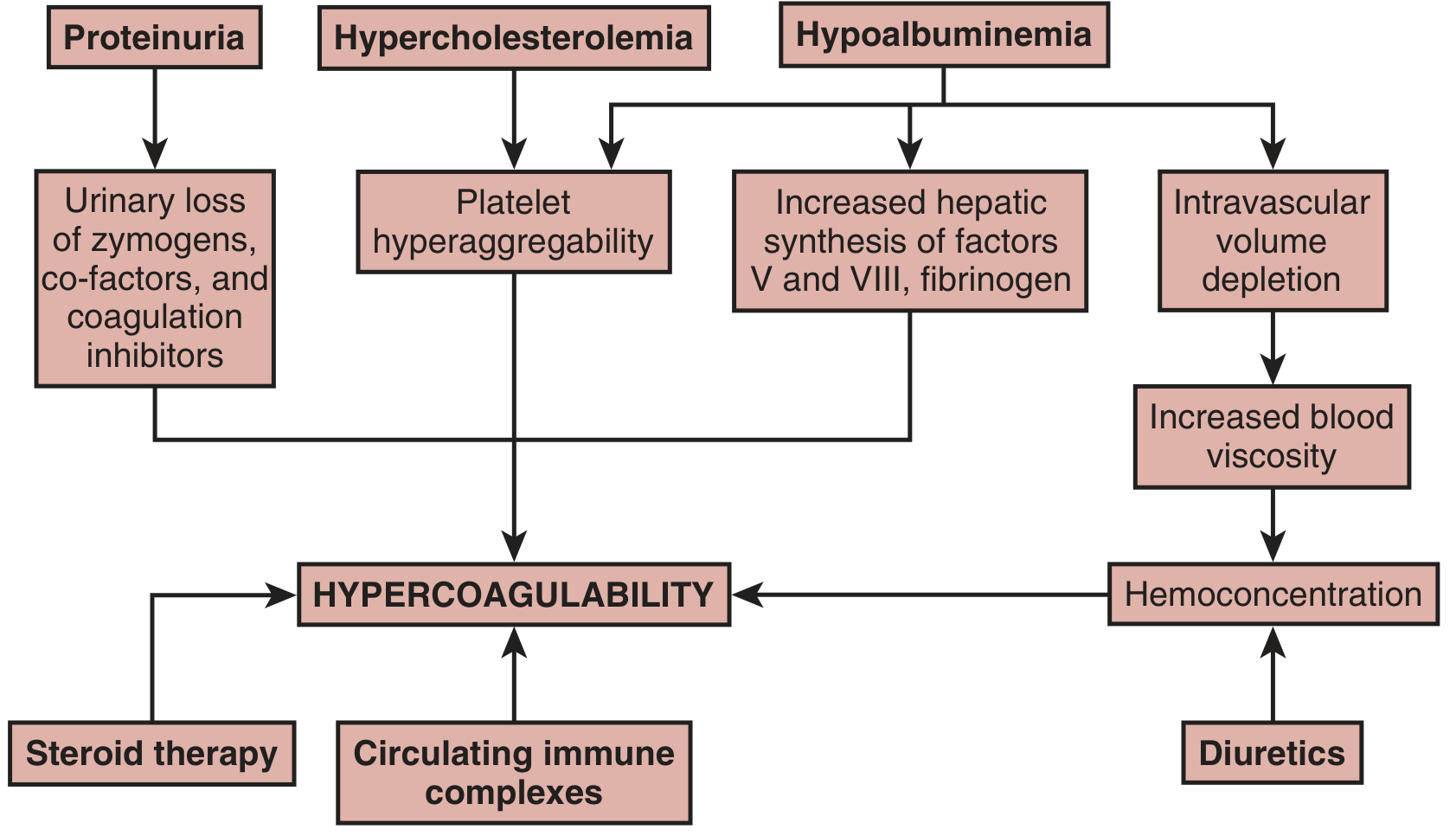
Mechanisms of hypercoagulability in nephrotic syndrome (Brenner & Rector's The Kidney)
- Urinary loss of anticoagulant proteins: antithrombin III, protein C, protein S, plasminogen
- Increased hepatic synthesis of procoagulant proteins: fibrinogen, factors V and VIII
- Platelet hyperaggregability from hypercholesterolemia
- Hemoconcentration from intravascular volume depletion
- Steroid therapy and circulating immune complexes compound the risk
Renal vein thrombosis is the most classic complication, especially with severe proteinuria (>10 g/24 hr) and severe hypoalbuminemia (<2 g/dL). Risk is highest in membranous nephropathy and amyloidosis. DVT and pulmonary embolism also occur.
2. Infection
- Loss of IgG (small molecule), reduced complement activity, and diminished T-cell function → susceptibility to encapsulated organisms (Streptococcus pneumoniae), cellulitis, and spontaneous bacterial peritonitis.
3. Acute Kidney Injury
- Low effective circulating volume
- Acute tubular necrosis (especially MCD in patients >50 years)
- NSAIDs causing acute interstitial nephritis in MCD
- Renal vein thrombosis
- Crescentic GN superimposed on existing disease
4. Nutritional/Metabolic Deficiencies from protein loss
| Protein Lost | Consequence |
|---|---|
| Transferrin | Iron deficiency anemia |
| Vitamin D-binding protein | Vitamin D deficiency, hypocalcemia |
| IgG, complement | Immunodeficiency |
| Thyroxine-binding globulin | Low total T4 (free T4 normal) |
| Albumin-bound drugs | Altered drug pharmacokinetics |
Diagnosis
Approach in adults: Kidney biopsy is almost always indicated in adults, as the underlying cause determines management. Exceptions: known diabetic nephropathy with classic clinical picture, or typical MCD presentation (bland sediment, rapid response to steroids in a young patient).
Evaluation:
- 24-hour urine protein OR spot urine protein:creatinine ratio
- Serum albumin, lipid panel, renal function (BUN, creatinine, eGFR)
- Urinalysis with microscopy
- Serology: ANA, anti-dsDNA (SLE), ANCA, complement C3/C4, anti-PLA2R (membranous nephropathy), hepatitis B/C serology, HIV, serum/urine protein electrophoresis
- Kidney biopsy with light microscopy (LM), immunofluorescence (IF), and electron microscopy (EM)
Specific Diseases
Minimal Change Disease (MCD)
- LM: Normal
- IF: Negative
- EM: Diffuse foot process effacement (>90%)
- Treatment: Corticosteroids (high response rate in children; variable in adults). Anti-CD20 agents (rituximab) show promise in steroid-resistant or frequently relapsing disease.
- In children: Often treated empirically without biopsy.
FSGS
- LM: Focal (some glomeruli) and segmental (part of glomerulus) sclerosis
- EM: Foot process effacement - >80% effacement favors primary FSGS; <80% favors secondary
- Primary FSGS: Corticosteroids, calcineurin inhibitors (tacrolimus/cyclosporine), mycophenolate mofetil. High risk of recurrence post-transplant.
- Secondary FSGS: Treat underlying cause; antiproteinuric therapy; avoid immunosuppression.
- Collapsing FSGS: Strongly associated with HIV and COVID-19; aggressive course.
- APOL1 risk alleles: Associated with high-risk FSGS in African ancestry patients.
Membranous Nephropathy (MN)
- LM: Thickened GBM with "spike and dome" pattern on silver stain
- IF: Granular IgG and C3 along GBM
- EM: Subepithelial electron-dense deposits
- Natural history: "Rule of thirds" - 1/3 spontaneous complete remission, 1/3 partial remission, 1/3 progress to ESKD
- Markers: Anti-PLA2R antibody (~70% primary MN) - useful for diagnosis and monitoring
- Treatment: Reserved for persistent NS or declining GFR. Options include calcineurin inhibitors, cyclophosphamide + corticosteroids (Ponticelli regimen), rituximab (increasingly preferred).
Management
Non-Specific (All Causes)
| Strategy | Details |
|---|---|
| Diet | Low-salt diet; protein restriction 0.8-1 g/kg/day |
| RAAS blockade | ACE inhibitor or ARB - reduces proteinuria, edema, dyslipidemia, and progression |
| Diuretics | Loop diuretics for edema. Note: hypoalbuminemia reduces furosemide protein binding, enlarging its volume of distribution and requiring higher doses |
| Statins | For hyperlipidemia-associated cardiovascular risk |
| Anticoagulation | For those at high thromboembolic risk (especially MN with albumin <2.5 g/dL) |
| Vaccinations | Pneumococcal and other vaccines due to infection risk |
Diuretic Resistance
A more logical approach is to reduce proteinuria first (with ACE inhibitor/ARB), then add loop diuretics. Volume-expanded (overfill) vs. volume-contracted (underfill) states should be distinguished, as diuretics alone are safe for overfill but can worsen underfill edema.
Brenner and Rector's The Kidney, p. 2277; NKF Primer, p. 190
Nephrotic vs. Nephritic - Quick Comparison
| Feature | Nephrotic | Nephritic |
|---|---|---|
| Proteinuria | >3.5 g/day | Sub-nephrotic (<3.5 g/day) |
| Hematuria | Minimal/absent | Prominent (RBC casts) |
| Edema | Marked (oncotic) | Mild-moderate (volume) |
| BP | Variable | Hypertension |
| Mechanism | Permeability defect (podocytes) | Inflammatory (GN) |
| GFR | Usually preserved initially | Often reduced |
Recent Evidence (2024-2026)
- A 2025 Cochrane systematic review examined interventions for idiopathic steroid-resistant nephrotic syndrome in children (PMID: 40337980), reflecting ongoing challenges in this population.
- A 2026 meta-analysis examined rituximab-induced hypogammaglobulinemia in childhood NS (PMID: 41843217) - a clinically important adverse effect to monitor when using anti-CD20 therapy.
- A 2024 systematic review documented NS associated with solid malignancies (PMID: 38965515), reinforcing the need to screen adult-onset NS for occult malignancy, especially in MN.
This is a shared conversation. Sign in to Orris to start your own chat.