myocarditis
Reading File
Finding Sources
Searching PubMed
myocarditis
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive, well-sourced content from multiple authoritative textbooks. Here is a complete overview of myocarditis.
Myocarditis
Definition
Myocarditis is an inflammatory process involving the myocardium, defined histologically by mononuclear cell infiltrates within the myocardial tissue. It encompasses a diverse group of clinical entities caused by infectious agents, immune-mediated damage, or toxins.
- Goldman-Cecil Medicine, Ch. 47
- Robbins & Kumar Basic Pathology
Epidemiology
- Incidence is difficult to estimate because presentation ranges from asymptomatic ECG changes to hemodynamic collapse and sudden death.
- Population prevalence estimates: 1 in 100,000 to 1 in 10,000.
- Postmortem studies identify myocarditis in up to 12% of young victims of sudden cardiac death.
- Some degree of subclinical myocarditis is detected in nearly 10% of routine autopsies.
- Up to 5% of patients with viral illness may exhibit some form of myocarditis.
Etiology
Viral (most common in Western world)
- Enteroviruses (Coxsackievirus A and B) historically predominated
- Parvovirus B19 and human herpesvirus 6 (HHV-6) are now increasingly detected
- Others: adenovirus, H1N1 influenza, SARS-CoV-2, CMV, HIV, Epstein-Barr, hepatitis C, rubella, varicella-zoster, RSV, rabies
Protozoal
- Trypanosoma cruzi (Chagas disease) - the most common infective myocarditis worldwide, endemic in Central/South America; about 300,000 infected individuals live in the US. Cardiac involvement occurs in the vast majority; 10% die in the acute phase, with others developing progressive CHF and arrhythmia 10-20 years later.
- Toxoplasma gondii - especially in immunocompromised hosts
Bacterial
- Corynebacterium diphtheriae, Mycoplasma pneumoniae, Salmonella, Staphylococcus, Mycobacterium, meningococcus, Borrelia burgdorferi (Lyme disease - occurs in ~5% of Lyme patients, usually self-limited conduction system disease)
Spirochetal
- Treponema pallidum, Borrelia, Leptospira
Fungal
- Aspergillus, Candida, Cryptococcus, Histoplasma
Parasitic
- Trichinella spiralis (most common helminthic cause), Echinococcus, Taenia solium
Immune-mediated / Non-infectious
- Systemic autoimmune diseases: SLE, systemic sclerosis, polymyositis/dermatomyositis, sarcoidosis, eosinophilic granulomatosis with polyangiitis (EGPA)
- Giant cell myocarditis (rare, often fulminant)
- Drug hypersensitivity (hypersensitivity myocarditis): penicillin, sulfonamides, tetracycline, methyldopa - characterized by eosinophilic infiltrates
- mRNA COVID-19 vaccination: rare, especially in male adolescents and young adults, more often after the second dose, typically within one week; most cases recover uneventfully
- Heart transplant rejection
Pathogenesis
Three stages are proposed:
- Acute stage: direct cytotoxicity, focal myocyte necrosis
- Subacute stage: rise in humoral factors, autoimmune injury
- Chronic stage: diffuse myocardial fibrosis, potential progression to dilated cardiomyopathy (DCM)
In viral myocarditis, direct cell death by some viruses occurs, but in most cases the injury results from the immune response against virally infected cells - analogous to T-cell-mediated hepatocyte damage in viral hepatitis. Some viruses trigger immune reactions that cross-react with myocardial proteins (e.g., myosin heavy chain - molecular mimicry).
Anti-beta-myosin antibodies are elevated in patients with myocarditis and DCM. Myocarditis is linked to the development of DCM in up to 16% of adults and 46% of children; idiopathic DCM after myocarditis may be predominantly autoimmune. Efficient viral clearance usually leads to full recovery; breakdown of T-cell tolerance can cause chronic inflammation.
- ROSEN's Emergency Medicine, Ch. 68
Morphology / Histopathology
Gross: The heart may be normal or dilated in acute disease. In advanced stages, the myocardium is flabby, often mottled with pale and hemorrhagic areas. Mural thrombi may be present.
Microscopy:
- Viral myocarditis: edema, interstitial inflammatory infiltrates (predominantly lymphocytic, often patchy), and myocyte injury
- Hypersensitivity myocarditis: interstitial and perivascular infiltrates with lymphocytes, macrophages, and a high proportion of eosinophils
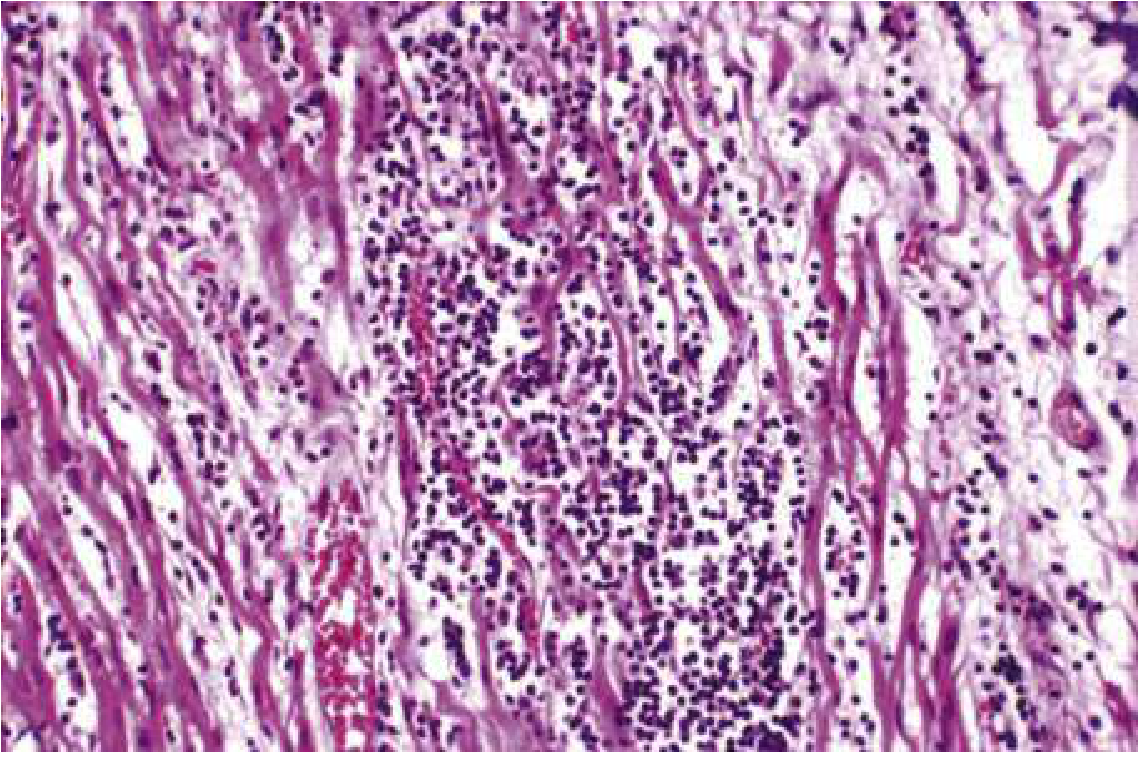
The histological Dallas criteria (leukocyte infiltration + necrosis) remain the gold standard but are debated given sampling error issues on biopsy.
- Robbins & Kumar Basic Pathology, p. 375
Clinical Presentation
The presentation is highly variable:
| Pattern | Features |
|---|---|
| Flu-like prodrome | Fever, fatigue, myalgias, vomiting, diarrhea (1-2 weeks before cardiac symptoms) |
| Chest pain | Can mimic acute coronary syndrome |
| Heart failure | Dyspnea (most common in adults), reduced LVEF, global hypokinesis |
| Dysrhythmias | Palpitations, syncope, ventricular tachycardia, AV block |
| Fulminant | Hemodynamic collapse, cardiogenic shock (especially in infants) |
| Asymptomatic | Detected incidentally |
In adults, the most common presenting symptoms are dyspnea, chest pain, and dysrhythmias. In children, dyspnea predominates; infants may present with cyanosis, respiratory distress, fever, and cardiac failure. Toxic appearance or tachycardia disproportionate to fever may be the only finding.
Differential Diagnosis
- Acute myocardial infarction (most important)
- Other infectious processes with cardiac involvement
- Takotsubo cardiomyopathy
- Dilated cardiomyopathy
- Arrhythmogenic cardiomyopathy
Patients with myocarditis are typically young with few coronary risk factors. Chest pain in myocarditis does not evolve with ischemic ECG changes following a coronary territory distribution.
Diagnostic Workup
ECG
- Sinus tachycardia (most common)
- Widened QRS, low voltages
- Prolonged QT interval
- AV block
- ST/T-wave changes that may simulate an AMI pattern but extend beyond the distribution of a single coronary artery
Biomarkers
- Troponin may be elevated (timing is variable; a negative troponin does not exclude the diagnosis)
- WBC, CRP, ESR: not diagnostically useful
- Serologic studies: rising antibody titers to specific pathogens; PCR on tissue
Echocardiography
- Reduced LVEF, global hypokinesis, regional wall motion abnormalities not following coronary anatomy
- May be normal or show modest changes
- Pericardial effusion may coexist
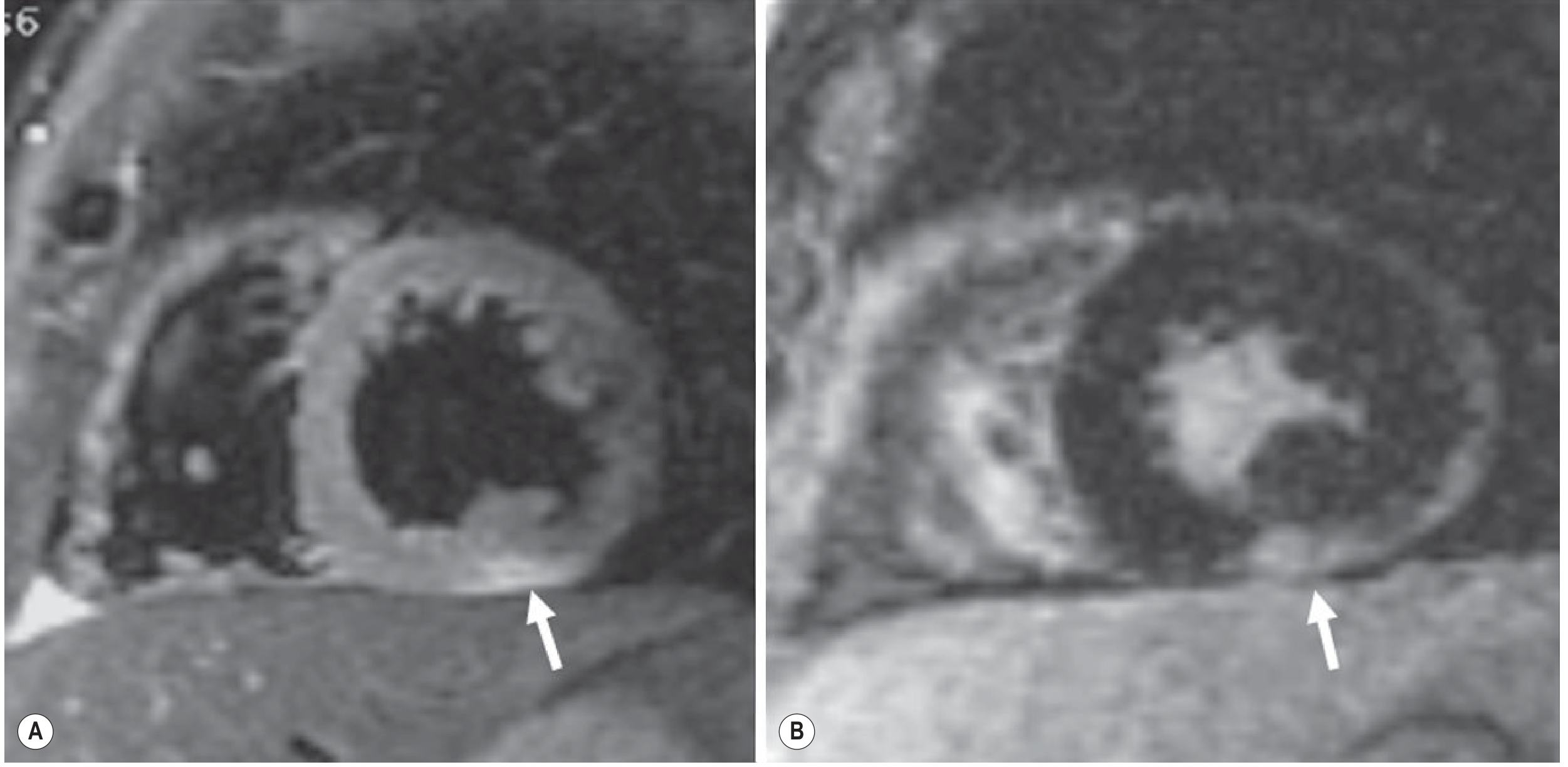
Cardiac MRI (CMR) - key non-invasive modality
The Lake Louise Criteria use three findings:
- T2-weighted imaging: subepicardial or myocardial edema
- Early gadolinium enhancement: inflammatory hyperemia
- Late gadolinium enhancement (LGE): non-ischemic pattern - typically subepicardial, most often in the lateral and/or inferior wall
This pattern distinguishes myocarditis from AMI (where LGE is subendocardial or transmural) and from Takotsubo (where LGE is absent). Septal, mid-wall, and patchy LGE distributions correlate with increased risk of sudden death.
Coronary Angiography
- Usually shows normal arteries; performed to exclude obstructive CAD when ACS cannot be ruled out by history/ECG alone
Endomyocardial Biopsy
- Still the gold standard for formal diagnosis
- Limited by variable sensitivity and specificity due to patchy inflammation and sampling error
- MRI guidance can improve yield by targeting abnormal regions
- Biopsy may identify alternative causes (e.g., giant cell myocarditis, amyloid) or confirm inflammatory etiology
- Not routinely performed; reserved for cases where the result will change management
Management
Treatment is primarily supportive:
Heart Failure
- Diuretics: furosemide (10 mg IV initially in diuretic-naive patients)
- Vasodilators: nitroglycerine for CHF symptom relief
- Inotropes: dobutamine (2 mcg/kg/min) for severe hemodynamic compromise
- ACE inhibitors (e.g., lisinopril): long-term benefit, especially in Chagas-related heart failure
- Mechanical circulatory support: VADs (temporary/percutaneous) as a bridge to recovery or transplant; ECMO for refractory cases
- Cardiac transplantation: for non-recovery, though outcomes are worse than transplant for other indications (lower 1-year survival, higher rejection rates)
Rhythm Management
- Rate and rhythm control as needed
- Amiodarone (600 mg/day) for ventricular dysrhythmias
- ICD consideration in patients with persistent ventricular arrhythmias
Activity Restriction
- Athletes with myocarditis should not compete until signs of inflammation have resolved and LV function has normalized - exercise worsens myocarditis in animal models
Immunosuppression
- No proven benefit in viral myocarditis in clinical trials
- May be appropriate for autoimmune causes (SLE, giant cell myocarditis, sarcoidosis)
- Corticosteroids, azathioprine, cyclosporine have been studied without consistent benefit in viral disease
Specific Causes
- Chagas disease: benzmidazole (ages 2-12 yr: 5-8 mg/kg/day x 60 days), nifurtimox (8-15 mg/kg/day depending on age)
- Drug hypersensitivity: withdraw the offending agent
- Autoimmune disease: optimize immunosuppressive therapy
Prognosis and Complications
- 10-20% rate of major adverse cardiac events overall
- Complications: ventricular dysrhythmias, LV aneurysm, CHF, progression to dilated cardiomyopathy (DCM)
- Myocarditis accounts for up to 16% of adult DCM cases and up to 46% in children
- Fulminant presentation in children has a higher rate of in-hospital death, transplantation, and persistent LV dysfunction compared with non-fulminant disease
- Patients are at elevated risk for sudden cardiac death (SCD), including those who are asymptomatic
Recent Evidence (PubMed 2024-2026)
- A 2024 systematic review and meta-analysis in JAMA Oncology (PMID 39172480) found that immune checkpoint inhibitor-related cardiotoxicity - including myocarditis - is increasingly recognized in cancer patients and carries a high mortality rate.
- A 2025 systematic review (PMID 38221509) in ESC Heart Failure examined autopsy findings in fatal COVID-19 vaccine-induced myocarditis cases, confirming histopathological evidence of myocarditis in these rare events.
Sources: Robbins & Kumar Basic Pathology; ROSEN's Emergency Medicine (9e), Ch. 68; Goldman-Cecil Medicine (International Ed.), Ch. 47; Braunwald's Heart Disease (11e); Grainger & Allison's Diagnostic Radiology, Ch. 14.
differential diagnosis table
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.