Mayocardial infraction bsc nursing
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Loading Image
Loading Image
I now have all the material needed for a comprehensive BSc Nursing-level answer. Let me compose the full response.
Myocardial Infarction (MI) - BSc Nursing
Definition
Myocardial infarction (MI), commonly called a "heart attack," is necrosis (death) of heart muscle resulting from ischemia (inadequate blood supply). The 2018 joint U.S./European Cardiology task force defines it as "the presence of acute myocardial injury detected by abnormal cardiac biomarkers in the setting of evidence of acute myocardial ischemia."
- Robbins & Kumar Basic Pathology, p. 353
Etiology and Risk Factors
The major underlying cause is atherosclerosis of the coronary arteries. Risk factors include:
| Modifiable | Non-modifiable |
|---|---|
| Hypertension | Age (risk rises progressively) |
| Diabetes mellitus | Male sex (women protected pre-menopause) |
| Smoking | Family history |
| Dyslipidemia | Post-menopause (estrogen loss) |
| Obesity / Physical inactivity | |
| Cocaine use |
About 10% of MIs occur before age 40; 45% before age 65. Men are at greater risk, but the gap narrows with age.
- Robbins & Kumar Basic Pathology, p. 353
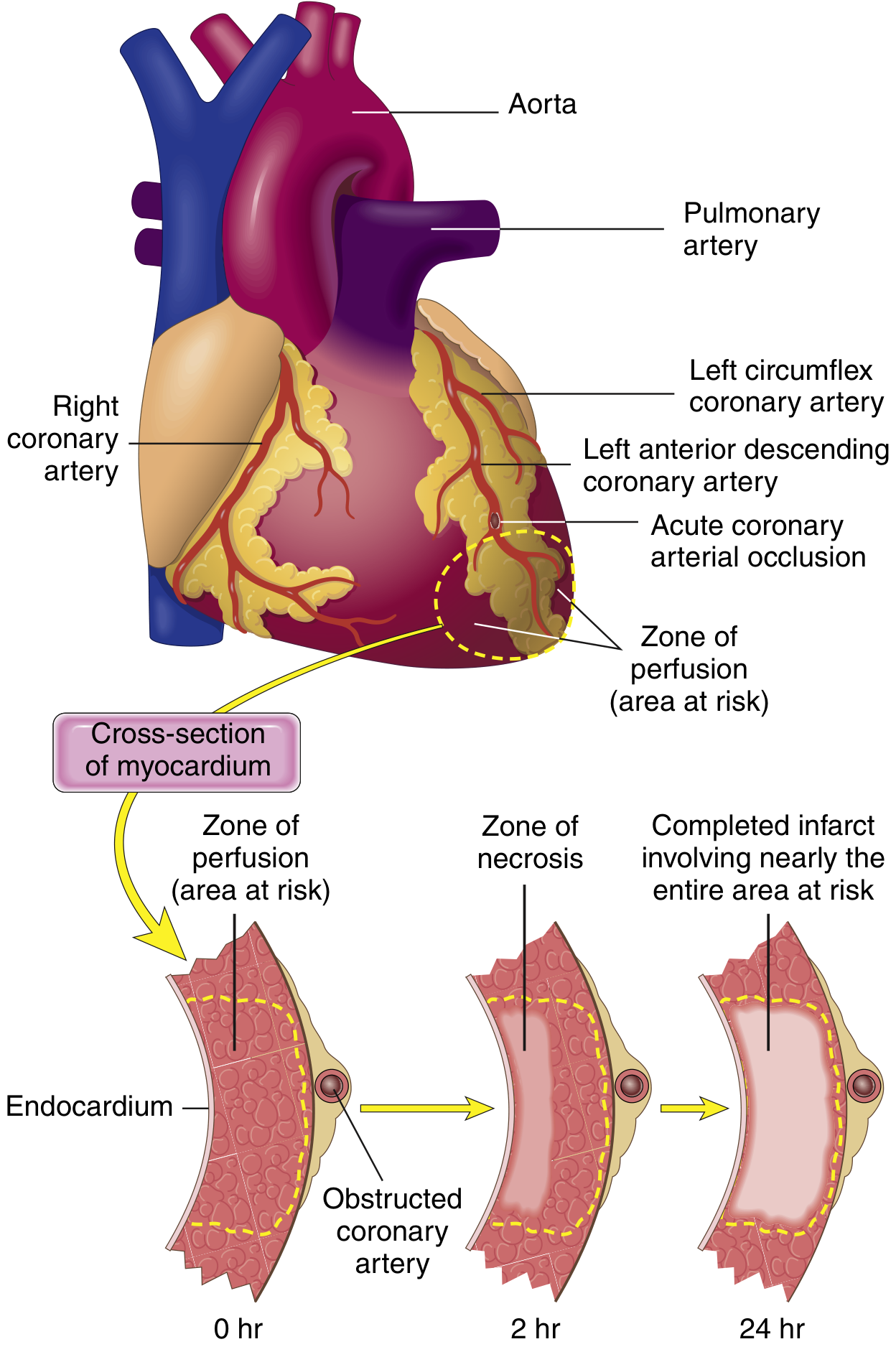
Pathophysiology
Step-by-step Mechanism
- An atheromatous plaque is disrupted by endothelial injury, intraplaque hemorrhage, or mechanical forces, exposing subendothelial collagen and necrotic contents to blood.
- Platelets adhere, aggregate, and release thromboxane A2, ADP, and serotonin - triggering further aggregation and vasospasm.
- Coagulation is activated by tissue factor exposure, building a growing thrombus.
- Within minutes, the enlarging thrombus completely occludes the coronary artery lumen.
- Angiography within 4 hours of MI shows coronary thrombosis in ~90% of cases.
In ~10% of MIs, transmural infarction occurs without occlusive atherosclerosis - attributed to coronary artery vasospasm or embolization (e.g., from atrial fibrillation or valve vegetations).
- Robbins & Kumar Basic Pathology, p. 353-354
Cellular Response to Ischemia
- Within seconds: aerobic metabolism stops; ATP falls; lactic acid accumulates.
- Within minutes: contractility is lost (but still reversible).
- After 20-40 minutes: irreversible damage and coagulative necrosis of myocytes begins.
- The subendocardial zone is most vulnerable - it is farthest from epicardial blood supply and exposed to high intramural pressures.
- In 80-90% of deaths from ischemia, the cause is ventricular fibrillation from myocardial irritability, not mechanical failure.
Types / Patterns of MI
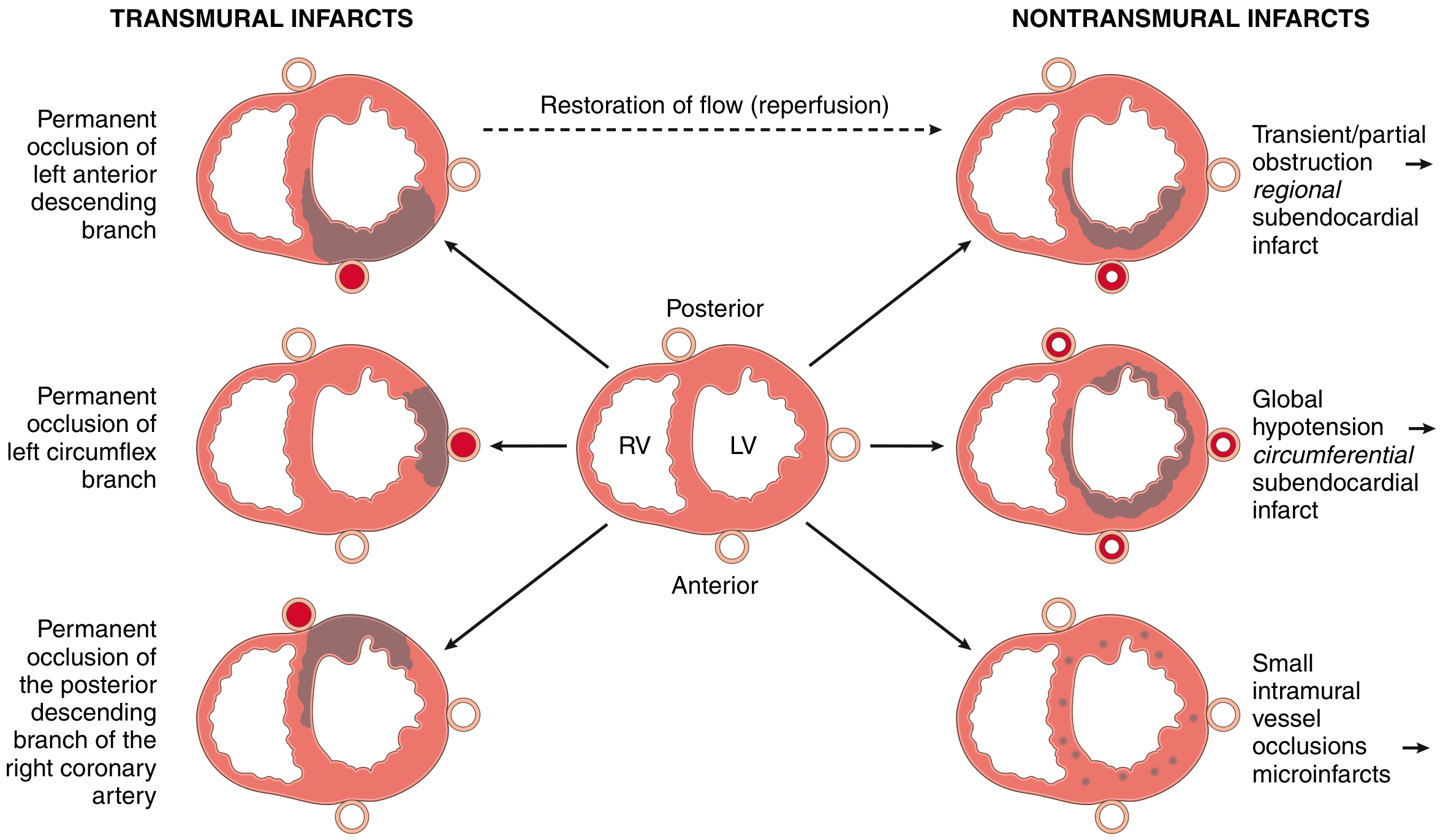
By Location of Vessel
| Occluded Artery | % of MIs | Area Affected |
|---|---|---|
| Left Anterior Descending (LAD) | 40-50% | Anterior LV wall, anterior 2/3 of septum, apex |
| Right Coronary Artery (RCA) | 30-40% | Right ventricle, posterior LV, posterior septum |
| Left Circumflex (LCX) | 15-20% | Lateral LV wall |
By Depth (Transmural vs. Subendocardial)
- Transmural infarction: Full thickness of the ventricular wall; caused by complete epicardial vessel occlusion with atherosclerosis + acute thrombus. Associated with ST-elevation MI (STEMI).
- Subendocardial infarction: Limited to the inner 1/3 of myocardium; thrombus is lysed before necrosis becomes transmural. Associated with NSTEMI.
- Microscopic infarcts: Small vessel occlusions (vasculitis, emboli, vasospasm); no diagnostic ECG changes.
- Robbins & Kumar Basic Pathology, p. 354-356
Morphological Changes Over Time
Table (from Robbins & Kumar Basic Pathology, Table 9.2):
| Time | Gross Features | Light Microscopic Findings |
|---|---|---|
| 0-30 min | None | None (electron microscopy: mitochondrial swelling, glycogen loss) |
| 30 min - 4 hr | None | Waviness of fibers at border |
| 4-12 hr | Occasional dark mottling | Coagulation necrosis begins; edema; hemorrhage |
| 12-24 hr | Dark mottling | Coagulation necrosis; pyknotic nuclei; hypereosinophilic myocytes; early neutrophil infiltrate |
| 1-3 days | Yellow-tan center with mottling | Loss of nuclei and striations; increased neutrophils |
| 3-7 days | Hyperemic border; central softening | Dead myofiber disintegration; macrophage phagocytosis begins |
| 7-10 days | Yellow-tan, soft with depressed red-tan margins | Early granulation tissue formation |
| 10-14 days | Red-gray depressed borders | Well-established granulation tissue |
| 2-8 weeks | Gray-white | Progressive collagen deposition (fibrosis) |
| >2 months | White, dense scar | Dense collagenous scar |
Key point for exams: MI less than 12 hours old is usually NOT grossly visible. Vital stains (triphenyl tetrazolium chloride) can reveal infarcts >3 hours old - necrotic areas stain pale (enzymes leak out), while healthy tissue stains red.
Clinical Features / Signs and Symptoms
Classic Presentation
- Chest pain: Sudden onset, severe, crushing/squeezing, substernal, radiates to left arm, jaw, neck, back
- Diaphoresis (profuse sweating)
- Dyspnea (shortness of breath)
- Nausea and vomiting
- Sense of impending doom / anxiety
- Pallor, cold clammy skin
- Tachycardia or bradycardia
- Hypotension (in severe cases)
Atypical Presentation (common in women, elderly, diabetics)
- Epigastric pain / indigestion-like symptoms
- Fatigue, weakness
- Silent MI (no pain - especially in diabetics due to neuropathy)
Diagnosis
1. ECG (Electrocardiogram)
The hallmark of acute MI is ST-segment elevation in leads overlying the area of infarction.
Three electrical abnormalities cause ECG changes:
| Defect in Infarcted Cells | Current Flow | ECG Change |
|---|---|---|
| Rapid repolarization | Out of infarct | ST segment elevation |
| Decreased resting membrane potential | Into infarct | TQ depression (seen as ST elevation) |
| Delayed depolarization | Out of infarct | ST segment elevation |
After days to weeks, the infarcted zone becomes electrically silent, and pathological Q waves appear - the permanent marker of a completed MI.
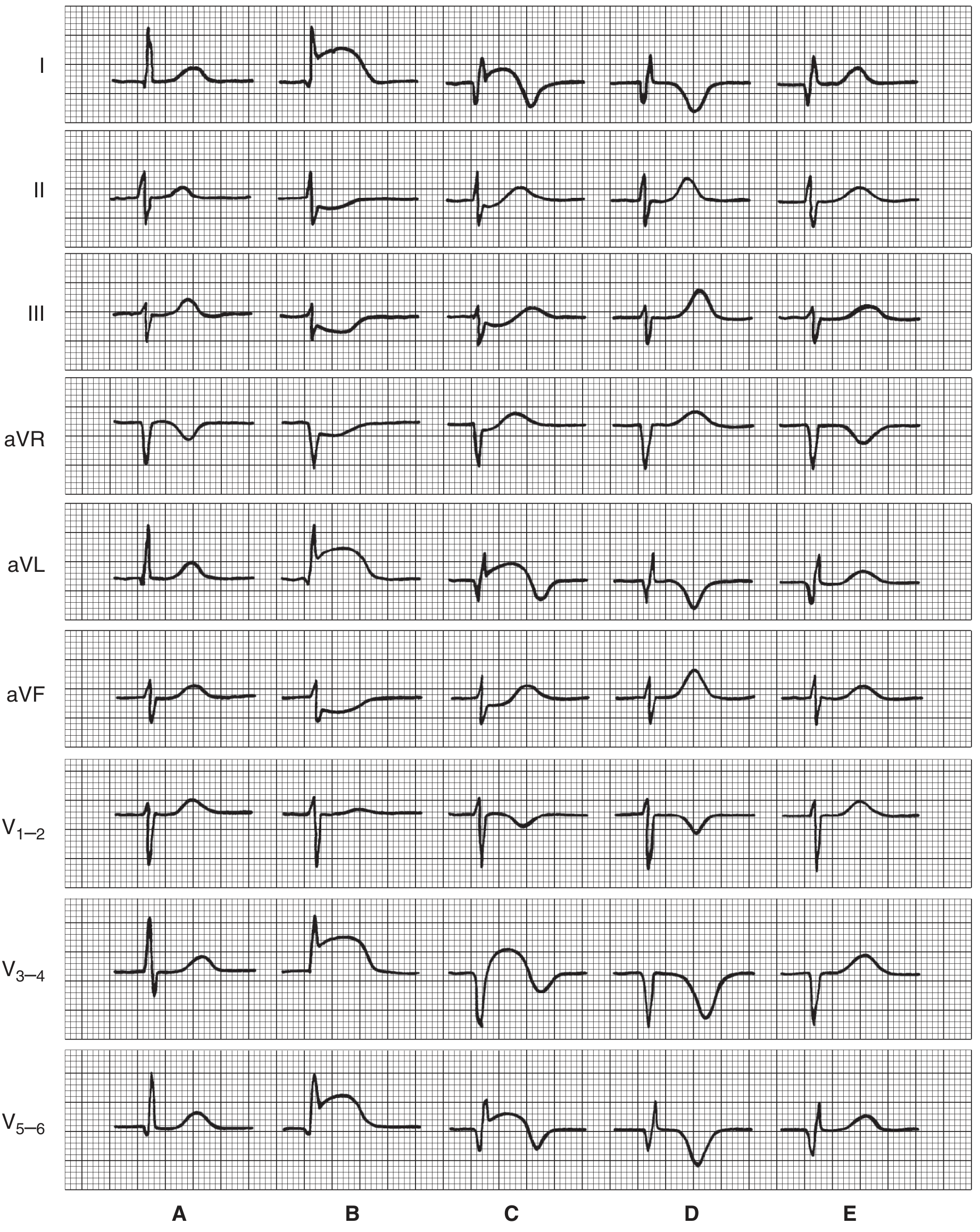
- STEMI: ST elevation + Q waves (transmural)
- NSTEMI: No ST elevation; ST depression or T-wave inversion (subendocardial)
2. Cardiac Biomarkers
| Biomarker | Rises | Peaks | Returns to Normal | Notes |
|---|---|---|---|---|
| Troponin I / T | 3-6 hr | 24-48 hr | 7-10 days | Most specific and sensitive; gold standard |
| CK-MB | 3-6 hr | 12-24 hr | 48-72 hr | Useful for reinfarction detection |
| Myoglobin | 1-2 hr | 4-8 hr | 24 hr | First to rise; less specific |
| LDH | 24-48 hr | 3-6 days | 8-14 days | Older marker |
Troponin I and T are the gold standard markers - they are highly specific for myocardial injury.
3. Other Diagnostic Tests
- Echocardiography: Wall motion abnormalities, ejection fraction assessment
- Coronary angiography: Definitive identification of the blocked vessel
- Chest X-ray: Pulmonary edema, cardiomegaly
- CBC: Leukocytosis (inflammatory response)
- Serum lipids, blood glucose
Management / Treatment
Immediate (Emergency) Management - "MONA" (or Modified)
| Drug/Action | Purpose |
|---|---|
| Morphine 2-4 mg IV (every 5 min) | Pain relief; reduces anxiety and preload |
| Oxygen (if SpO2 <90%) | Correct hypoxemia; not given if O2 saturation is normal |
| Nitroglycerin 0.4 mg sublingual (up to 3 doses, 5 min apart) | Reduces preload; dilates coronary vessels |
| Aspirin 160-325 mg chewed | Inhibits COX-1; reduces thromboxane A2; prevents further platelet aggregation |
- Harrison's Principles of Internal Medicine 22E, 2025
Reperfusion Therapy (Most Critical)
"Time is muscle" - the goal is restoring blood flow as fast as possible.
-
Primary PCI (Percutaneous Coronary Intervention): Preferred for STEMI if available. Goal: balloon inflation within 90 minutes of first medical contact (or 120 min if transfer required). More effective than thrombolysis.
-
Thrombolysis (fibrinolytic therapy): Used when PCI is not available within the recommended time. Agents: streptokinase, alteplase (tPA), reteplase, tenecteplase. Effective if given within 12 hours of symptom onset.
Antiplatelet and Anticoagulation Therapy
- Clopidogrel / Prasugrel / Ticagrelor (P2Y12 inhibitors): Added to aspirin; reduces reocclusion risk
- Unfractionated Heparin (UFH): IV bolus 60 U/kg then infusion; maintains artery patency after thrombolysis or PCI
- Enoxaparin (LMWH): Subcutaneous alternative; better bioavailability
Beta-Blockers
- Metoprolol 5 mg IV (every 2-5 min, up to 3 doses) if HR >60, SBP >100 mmHg
- Reduce myocardial O2 demand
- Reduce risk of reinfarction and ventricular fibrillation
- Contraindicated in acute decompensated HF, bradycardia, heart block
ACE Inhibitors / ARBs
- Started within 24 hours, especially for anterior MI with reduced EF
- Reduce ventricular remodeling
- Prevent HF progression
Statins
- High-intensity statin (e.g., atorvastatin 80 mg) started early and continued long-term
- Stabilize plaques, reduce inflammation and LDL
Complications
From Robbins & Kumar Basic Pathology:
| Complication | Time of Occurrence | Notes |
|---|---|---|
| Arrhythmias | Immediate/Early | Most common; VF is most lethal; seen in 3 phases (0-30 min, 12 hr, 3 days-weeks) |
| Cardiogenic shock | Early | Pump failure; >40% LV damage |
| Ventricular free wall rupture | 3-7 days | Cardiac tamponade; often fatal |
| Interventricular septal rupture | 3-7 days | New loud systolic murmur; VSD |
| Papillary muscle rupture | 3-7 days | Acute mitral regurgitation |
| Pericarditis (Dressler syndrome) | Days to weeks | Fibrinous inflammation over infarcted area |
| Mural thrombus | Days to weeks | Embolism risk; anticoagulation needed |
| Ventricular aneurysm | Weeks to months | Paradoxical wall motion; late complication |
| Heart failure | Any time | Due to loss of contractile mass |
Nursing Assessment
A nurse should assess for:
- Vital signs: HR, BP, RR, SpO2, temperature
- Pain: Onset, character, location, radiation, severity (0-10 scale), duration
- Skin: Pallor, cyanosis, diaphoresis, coolness, capillary refill
- Level of consciousness: Confusion, restlessness
- Lung sounds: Crackles (pulmonary edema), S3/S4 heart sounds
- Urine output: Oliguria suggests reduced cardiac output
- Peripheral pulses: Strength and regularity
- JVP (jugular venous pressure): Elevated in right heart failure
Nursing Diagnoses (NANDA)
- Acute pain related to myocardial ischemia
- Decreased cardiac output related to myocardial damage
- Activity intolerance related to reduced cardiac reserve
- Anxiety / Fear related to severity of illness and perceived threat of death
- Ineffective tissue perfusion (cardiopulmonary) related to coronary artery occlusion
- Risk for arrhythmia related to ischemia and electrolyte imbalance
- Deficient knowledge related to disease, treatment, and lifestyle modifications
Nursing Interventions
Immediate (Acute Phase)
- Admit to CCU / ICU; continuous ECG monitoring
- Establish IV access; administer medications as prescribed
- Administer supplemental oxygen (if SpO2 <90%)
- Relieve pain: Administer morphine/nitrates as ordered; reassess pain
- Complete bed rest to minimize myocardial oxygen demand
- Monitor vital signs every 15-30 minutes
- Monitor cardiac biomarkers (Troponin, CK-MB) serially
- Prepare patient for PCI/thrombolysis as indicated
- Keep defibrillator and crash cart at bedside
Ongoing Care
- Monitor for complications: arrhythmias, signs of heart failure, hypotension
- Fluid management: Strict input/output recording
- Psychological support: Calm environment; address patient and family anxiety
- Nutrition: Low-sodium, low-fat diet; restrict caffeine and stimulants
- Bowel care: Prevent straining (Valsalva increases cardiac workload) - stool softeners
- Leg exercises: Prevent DVT; graduated mobility
Rehabilitation / Discharge Teaching
- Medication adherence: Aspirin, beta-blockers, ACE inhibitors, statins (explain purpose and side effects)
- Activity progression: Gradual increase; cardiac rehabilitation referral
- Diet modification: Heart-healthy diet (DASH diet principles)
- Smoking cessation: Complete and permanent
- Risk factor control: BP, diabetes, cholesterol management
- When to seek emergency care: Recurrent chest pain, dyspnea, palpitations
- Psychological support: Depression is common post-MI; screen and refer
Prevention
Primary Prevention (Before MI)
- Control hypertension, diabetes, and dyslipidemia
- Smoking cessation
- Regular physical exercise (150 min/week moderate activity)
- Heart-healthy diet
- Weight management
Secondary Prevention (After MI)
- DAPT (dual antiplatelet therapy) for at least 12 months
- Statin therapy indefinitely
- Beta-blocker (at least 1 year post-MI)
- ACE inhibitor/ARB for reduced EF
- Cardiac rehabilitation
Key Points Summary for Exam
| Topic | Key Fact |
|---|---|
| Most common cause | Atherosclerosis with plaque disruption + thrombosis |
| Most common occluded vessel | LAD artery (40-50% of MIs) |
| Irreversible damage begins | After 20-40 minutes of ischemia |
| Time for full infarct | 3-6 hours without intervention |
| Gold standard biomarker | Cardiac Troponin I/T |
| Earliest biomarker | Myoglobin (rises in 1-2 hr) |
| ECG hallmark of STEMI | ST segment elevation |
| ECG permanent marker | Pathological Q waves |
| Most common cause of death | Ventricular fibrillation (80-90% of cardiac deaths) |
| Most lethal complication | Ventricular rupture (3-7 days) |
| Preferred reperfusion therapy | Primary PCI within 90 min |
| Nursing priority #1 | Pain relief + continuous ECG monitoring |
Sources:
- Robbins & Kumar Basic Pathology - Myocardial Infarction section, pp. 353-358
- Ganong's Review of Medical Physiology, 26th Edition - ECG changes in MI, p. 534
- Harrison's Principles of Internal Medicine, 22nd Edition (2025) - STEMI management
- Guyton and Hall Textbook of Medical Physiology - Myocardial Infarction
This is a shared conversation. Sign in to Orris to start your own chat.