Study of pericardial fluid after oericardiocentesis
Reading File
Finding Sources
Finding Sources
Searching PubMed
pericardial fluid analysis pericardiocentesis
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive information from multiple authoritative sources. Let me compile the full answer.
Pericardial Fluid Analysis After Pericardiocentesis
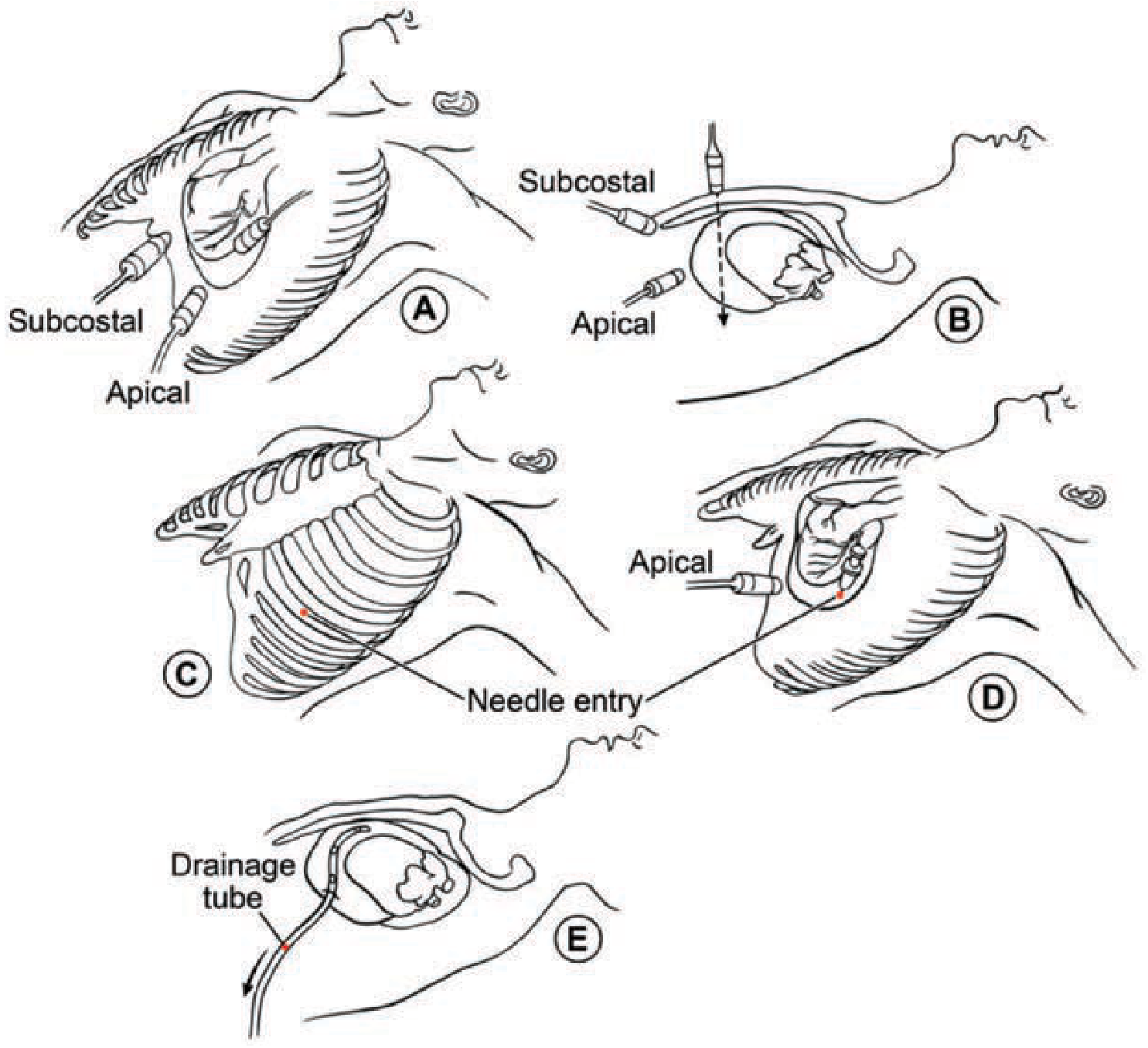
Echocardiographically guided pericardiocentesis showing needle entry sites (subcostal and apical), needle positioning, and drainage tube placement (E). - Fuster and Hurst's The Heart, 15th Ed.
1. Normal Pericardial Fluid
- Volume: 10-50 mL (Tietz: 25-35 mL) of clear, pale-yellow fluid
- Composition: a plasma ultrafiltrate - lymphocytes are the predominant cell type
- Functions as a lubricant protecting the heart from physical forces
2. Indications for Fluid Analysis
Per European Society of Cardiology (ESC) guidelines, pericardial fluid analysis is recommended in:
- Therapeutic pericardiocentesis for cardiac tamponade
- Suspected infectious or neoplastic pericarditis
- Moderate-to-large effusions (100 to >500 mL) of unknown cause not responding to therapy
Tietz Textbook of Laboratory Medicine, 7th Ed.
3. Specimen Collection
Fluid is obtained by either:
- Pericardiocentesis (sterile needle aspiration, image-guided)
- Pericardiotomy (following limited thoracotomy)
Procedure steps (echocardiographic guidance):
- Locate the area with the largest effusion volume and mark it
- Determine effusion depth and optimal angulation
- Perform pericardiocentesis after sterile prep and local anesthesia
- Confirm needle position by injecting agitated saline (bubbles visible on echo)
- Monitor fluid withdrawal with repeat echocardiography
- Place a 6F or 7F pigtail catheter to minimize reaccumulation
- Drain residual fluid every 4-6 hours; remove catheter after 2-3 days if no reaccumulation
Fuster and Hurst's The Heart, 15th Ed.
4. Gross (Macroscopic) Examination
| Appearance | Interpretation |
|---|---|
| Pale yellow, clear | Normal |
| Turbid | Infection or malignancy |
| Clear, straw-coloured | Uremia |
| Hemorrhagic / blood-like | Hemorrhagic effusion, malignancy, trauma, anticoagulant therapy |
| Milky / cloudy | Chylous or pseudochylous effusion |
| "Gold paint" (cholesterol-rich) | Hypothyroidism |
Important distinction - blood vs. hemorrhagic effusion:
| Feature | Hemorrhagic Effusion | Accidental Cardiac Puncture |
|---|---|---|
| Hematocrit | Lower than peripheral blood | Same as peripheral blood |
| Clotting | Usually does NOT clot | Clots |
| Blood gas | Different from arterial/venous | Similar to venous/arterial blood |
Henry's Clinical Diagnosis and Management by Laboratory Methods
5. Routine Laboratory Tests
The recommended routine panel includes:
| Test | Purpose |
|---|---|
| Cell count (WBC + differential) | Infection, inflammation, malignancy |
| Hematocrit / RBC count | Hemorrhagic effusion |
| Glucose | Infection screening |
| Total protein | Exudate vs. transudate |
| Lactate dehydrogenase (LD) | Exudate vs. transudate |
| Gram stain | Bacterial identification |
| Aerobic/anaerobic bacterial culture | Bacterial infection |
| Fungal and mycobacterial culture | TB, fungal pericarditis |
| Cytology | Malignant cells |
Henry's Clinical Diagnosis and Management; Fuster and Hurst's The Heart, 15th Ed.
6. Exudate vs. Transudate (Light's Criteria)
Light's criteria - originally validated for pleural fluid - are the most reliable tool for pericardial exudates/transudates. An exudate meets one or more of:
- Fluid/serum protein ratio > 0.5
- Fluid/serum LD ratio > 0.6
- Fluid LD > 200 U/L
- Specific gravity > 1.015
- Protein > 3.0 g/dL (fluid-to-serum ratio > 0.5)
Note: Most pericardial effusions are exudates. Detecting a transudate narrows the differential significantly (heart failure, hypoalbuminemia, hypothyroidism).
Henry's Clinical Diagnosis; Tietz Textbook of Laboratory Medicine, 7th Ed.
7. Microscopic Examination
WBC/Differential:
- Total WBC > 10,000/µL suggests bacterial, tuberculous, or malignant pericarditis
- Neutrophil predominance: bacterial pericarditis
- Lymphocyte predominance: viral, tuberculous, or malignant effusion
- Even with low WBC counts, a stained smear should always be examined for atypical or malignant cells
Cytology:
- Sensitivity 95%, specificity 100% for malignant cells
- Most common: metastatic carcinoma of the lung and breast
8. Chemical Analysis
Glucose
- < 60 mg/dL: diagnostic accuracy only 36% for exudate
- < 40 mg/dL: common in bacterial, tuberculous, rheumatic, or malignant effusions
- Fluid-to-serum ratio < 0.3: supportive of bacterial infection
Protein
-
3.0 g/dL: sensitivity 97% for exudate, but specificity only 22% - limited discriminating power
pH
- < 7.10: rheumatic or purulent pericarditis
- 7.20-7.30: malignancy, uremia, TB, or idiopathic
Lipids
- Triglycerides and cholesterol + lipoprotein electrophoresis: differentiates chylous from pseudochylous effusions
Enzymes
- LD > 200 U/L: exudate cutoff
- CK-MB, myoglobin, troponin I (postmortem): elevated in myocardial injury
Henry's Clinical Diagnosis and Management by Laboratory Methods
9. Special/Additional Tests
For Suspected Tuberculosis (TB Pericarditis)
These should be performed whenever TB is clinically suspected, given the long time for bacteriologic diagnosis:
| Test | Sensitivity | Specificity | Notes |
|---|---|---|---|
| Adenosine deaminase (ADA) | 94% (cutoff 30 U/L) / 93% (cutoff 40 U/L) | 68% / 97% | Most useful adjunct; median ADA much higher in TB than other effusions |
| Interferon-gamma (IFN-γ) | High | High | Elevated in TB serous effusions |
| PCR | Variable | High | Rapid, especially valuable when smear negative |
| Lysozyme | Adjunct | Adjunct | Elevated in TB |
| AFB smear and culture | Low-moderate | High | Gold standard but slow |
For Malignant Effusions
- Cytology remains the primary tool (95% sensitivity)
- CEA: does not add sensitivity beyond cytology; use remains limited
- Other tumor markers: preliminary/controversial
Emerging/Newer Approaches
- Cytokine and biomarker panels (in research): may distinguish inflammatory subtypes
- Anti-myolemmal antibodies: predictive of recurrence in chronic effusions
- Proteomics: under investigation
Braunwald's Heart Disease; Henry's Clinical Diagnosis; Fuster and Hurst's The Heart, 15th Ed.
10. Causes of Pericardial Effusion (Differential Diagnosis Guide)
| Cause | Typical Fluid Features |
|---|---|
| Viral / idiopathic | Exudate, lymphocytic, normal glucose |
| Bacterial | Turbid, WBC >10,000, neutrophils, very low glucose, positive culture |
| Tuberculosis | Exudate, lymphocytic, high ADA/IFN-γ, positive PCR/culture |
| Malignancy | Hemorrhagic or exudate, positive cytology, high LDH |
| Uremia | Clear, straw-colored, exudate |
| Hypothyroidism | "Gold paint" - cholesterol crystals |
| Trauma / anticoagulation | Hemorrhagic |
| Rheumatic / autoimmune | Low pH (<7.10), exudate |
| Chylous (thoracic duct injury) | Milky, high triglycerides, chylomicrons |
Summary: Diagnostic Yield
| Test | Highest Yield Condition |
|---|---|
| Culture (bacterial) | Purulent pericarditis |
| Cytology | Malignant pericarditis (95% sensitivity) |
| ADA / IFN-γ / PCR | Tuberculous pericarditis |
| Glucose < 40 | Bacterial, TB, rheumatic, malignancy |
| Exudate markers | Most pathologic effusions |
| Hematocrit comparison | Distinguish hemorrhagic effusion from cardiac puncture |
Sources:
- Henry's Clinical Diagnosis and Management by Laboratory Methods (Box 30.12, pp. 608-611)
- Braunwald's Heart Disease, 2 Vol Set (p. 951)
- Fuster and Hurst's The Heart, 15th Ed. (pp. 1700-1702)
- Tietz Textbook of Laboratory Medicine, 7th Ed. (p. 1646)
This is a shared conversation. Sign in to Orris to start your own chat.