🏥 BMC M1 — R&I Block High-Yield Study Guide
Batterjee Medical College, Jeddah | First Year | Examinations Preparation
TOPIC 1: GLOMERULAR FILTRATION — Physiology
📌 Overview of Renal Processes
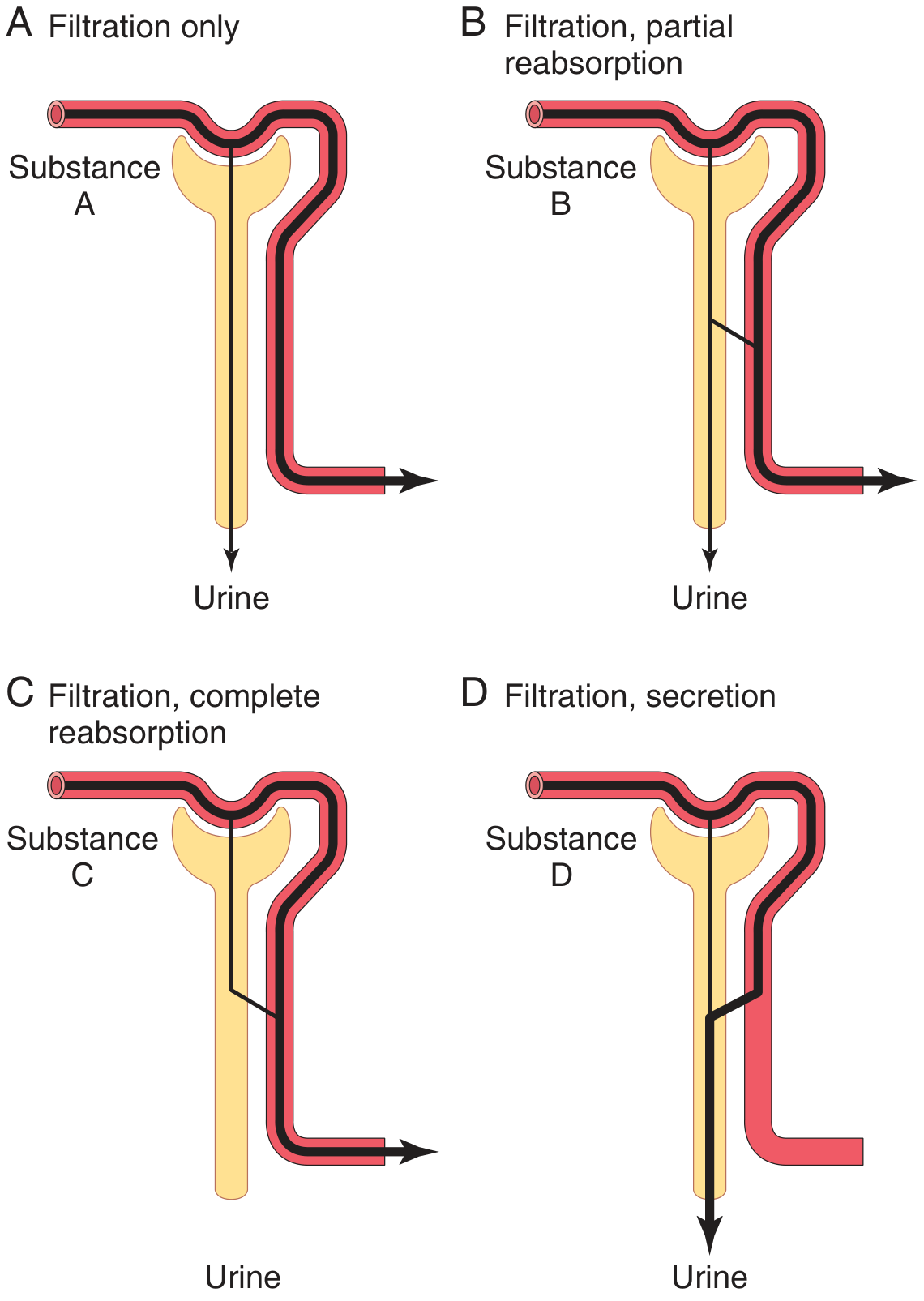
Urine formation results from three sequential processes:
Urinary Excretion = Filtration − Reabsorption + Secretion
| Process | Location | Key Feature |
|---|
| Glomerular filtration | Glomerulus → Bowman's capsule | Bulk, non-selective (except proteins) |
| Tubular reabsorption | All tubule segments | Selective, high-volume |
| Tubular secretion | Tubules → lumen | Organic acids/bases, K⁺, H⁺ |
Figure: Four patterns of renal handling — filtration only (A), partial reabsorption (B), complete reabsorption (C), filtration + secretion (D)
📌 Glomerular Filtration Rate (GFR)
| Parameter | Normal Value |
|---|
| GFR (both kidneys) | 125 mL/min = 180 L/day |
| Renal blood flow | ~20–25% of cardiac output |
| Filtration fraction | ~20% (GFR/RPF) |
| Plasma protein concentration in filtrate | ~0 (proteins NOT filtered) |
Why is a high GFR critical?
- Exposes the entire ECF to tubular scrutiny >10 times/day
- Allows rapid elimination of toxins
- In ESRD (GFR reduced to 10% of normal), BUN rises ~10× to maintain excretion balance
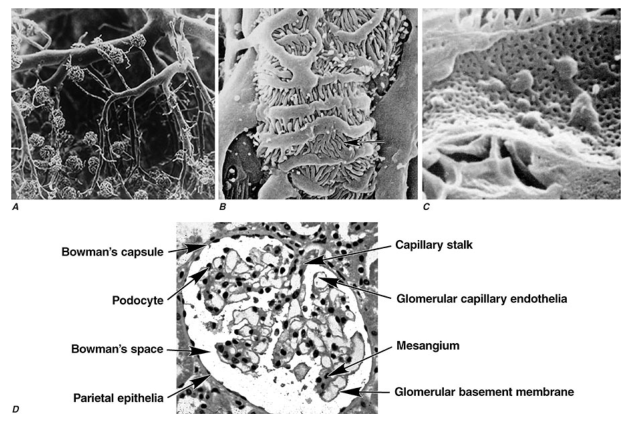
📌 Glomerular Filtration Barrier (3 Layers)
| Layer | Feature | Function |
|---|
| Fenestrated endothelium | 70–100 nm pores | Blocks blood cells, allows water + solutes |
| Glomerular basement membrane (GBM) | Negatively charged collagen IV | Charge barrier (repels albumin) |
| Podocytes (visceral epithelium) | Foot processes + filtration slits | Size + charge selectivity |
Figure: Scanning EM of glomerulus showing capillary loops, podocytes, foot processes, Bowman's capsule, and filtration slits
📌 Starling Forces Governing Filtration
Net Filtration Pressure = (P_GC − P_BS) − (π_GC − π_BS)
| Force | Direction | Approx. Value |
|---|
| Glomerular capillary hydrostatic pressure (P_GC) | ↑ Filtration | ~60 mmHg |
| Bowman's space hydrostatic pressure (P_BS) | ↓ Filtration | ~18 mmHg |
| Glomerular oncotic pressure (π_GC) | ↓ Filtration | ~32 mmHg |
| Bowman's space oncotic pressure (π_BS) | ↑ Filtration | ~0 mmHg |
| Net filtration pressure | | ~10 mmHg |
📌 Factors That Change GFR
| Factor | Effect on GFR | Mechanism |
|---|
| ↑ Afferent arteriole constriction | ↓ GFR | ↓ P_GC |
| ↑ Efferent arteriole constriction | ↑ then ↓ GFR | ↑ P_GC initially, then ↑ oncotic pressure |
| Angiotensin II | ↑ Efferent tone → maintains GFR in low flow | Efferent constriction |
| NSAIDs | ↓ GFR | Block prostaglandins → afferent constriction |
| ↑ Plasma protein | ↓ GFR | ↑ oncotic pressure |
| Urinary obstruction | ↓ GFR | ↑ P_BS |
📌 GFR Measurement — Renal Clearance
Clearance = (U_x × V̇) / P_x
Gold standard marker = INULIN (exogenous)
- Freely filtered, NOT reabsorbed, NOT secreted, NOT synthesized or broken down
- Inulin clearance = GFR exactly
Clinical estimate = Creatinine clearance
- Creatinine is freely filtered + small amount secreted → slightly overestimates GFR (~140 mL/min vs 125 mL/min)
| Substance | Clearance (mL/min) | Interpretation |
|---|
| Glucose | 0 | Completely reabsorbed |
| Sodium | 0.9 | Mostly reabsorbed |
| Inulin | 125 | GFR marker |
| Creatinine | ~140 | Filtered + secreted |
| PAH | ~625 | Filtered + secreted → measures RPF |
Key rule:
- Clearance < inulin → net reabsorption
- Clearance > inulin → net secretion
- Clearance = inulin → only filtered
📌 Autoregulation of GFR
GFR is maintained constant over MAP 80–180 mmHg via:
- Myogenic mechanism — afferent arteriole constricts when stretched
- Tubuloglomerular feedback (TGF) — macula densa senses ↑ NaCl → releases adenosine → afferent constriction
🧠 High-Yield MCQs — Glomerular Filtration
Q1. Normal GFR in an adult is:
- A) 60 mL/min
- B) 100 mL/min
- C) 125 mL/min ✓
- D) 180 mL/min
GFR = 125 mL/min (180 L/day). This is a consistently tested value at BMC.
Q2. Which substance is used as the gold standard to measure GFR?
- A) Creatinine
- B) PAH
- C) Inulin ✓
- D) Urea
Inulin is freely filtered, neither reabsorbed nor secreted, not metabolized, physiologically inert.
Q3. A substance has a clearance of 70 mL/min. Inulin clearance is 125 mL/min. This substance is:
- A) Only filtered
- B) Filtered and partially reabsorbed ✓
- C) Filtered and secreted
- D) Not filtered at all
Clearance < inulin → net reabsorption occurs.
Q4. Which of the following DECREASES GFR?
- A) Dilation of afferent arteriole
- B) ↑ Glomerular capillary pressure
- C) NSAIDs ✓
- D) ↑ Renal blood flow
NSAIDs block prostaglandins → afferent arteriole constricts → ↓ P_GC → ↓ GFR. Critical for pharmacology integration.
Q5. The filtration barrier between glomerular blood and Bowman's space includes all EXCEPT:
- A) Fenestrated endothelium
- B) Glomerular basement membrane
- C) Podocyte filtration slits
- D) Macula densa cells ✓
Macula densa is part of tubuloglomerular feedback, not the filtration barrier.
Q6. Oncotic pressure in Bowman's capsule is normally:
- A) 32 mmHg
- B) 18 mmHg
- C) 0 mmHg ✓
- D) 10 mmHg
Virtually no protein enters the filtrate, so oncotic pressure in Bowman's space ≈ 0.
Q7. Creatinine clearance slightly overestimates GFR because creatinine is:
- A) Reabsorbed by tubules
- B) Secreted by tubules ✓
- C) Synthesized in tubules
- D) Bound to plasma proteins
Q8. What is the filtration fraction?
- A) GFR/Renal Blood Flow
- B) GFR/Renal Plasma Flow ✓
- C) Urine output/Plasma volume
- D) Filtered load/Excreted amount
FF = GFR/RPF = 125/625 ≈ 20%
TOPIC 2: HISTOLOGY OF THE KIDNEY
📌 Overview of Renal Histology
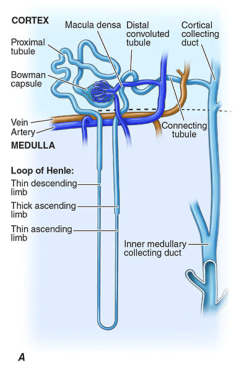
The kidney is composed of cortex and medulla. The functional unit is the nephron (~1 million per kidney).
Figure: Labeled nephron showing Bowman's capsule, glomerulus, proximal tubule, Loop of Henle, distal tubule, collecting duct in cortex and medulla (Harrison's)
📌 Nephron Components — Histological Features
1. Renal Corpuscle (Glomerulus + Bowman's Capsule)
| Component | Histology | Notes |
|---|
| Glomerulus | Tuft of fenestrated capillaries | Supported by mesangial cells |
| Parietal layer of Bowman's capsule | Simple squamous epithelium | Lines outer capsule |
| Visceral layer | Podocytes (modified epithelium) | Foot processes wrap capillaries |
| Mesangial cells | Between capillary loops | Phagocytic, contractile, matrix production |
| Juxtaglomerular (JG) cells | Modified smooth muscle of afferent arteriole | Secrete renin |
| Macula densa | Columnar cells of distal tubule | Senses NaCl; controls renin release |
2. Proximal Convoluted Tubule (PCT)
| Feature | Detail |
|---|
| Epithelium | Simple cuboidal with prominent brush border (microvilli) |
| Cytoplasm | Highly eosinophilic (acidophilic) — many mitochondria |
| Lumen | Relatively narrow, indistinct (due to brush border) |
| Location | Cortex |
| Function | Reabsorbs ~65–70% of filtered Na, water, glucose, amino acids, HCO₃⁻ |
BMC HY: PCT is distinguished from DCT by: larger cells, more eosinophilic cytoplasm, brush border, narrower lumen.
3. Loop of Henle
| Segment | Epithelium | Permeability |
|---|
| Descending thin limb | Simple squamous | Permeable to water; impermeable to solutes |
| Ascending thin limb | Simple squamous | Impermeable to water |
| Thick ascending limb | Simple cuboidal/columnar; NO brush border | Actively transports Na, K, Cl (NKCC2) |
4. Distal Convoluted Tubule (DCT)
| Feature | Detail |
|---|
| Epithelium | Simple cuboidal, NO brush border |
| Cytoplasm | Less eosinophilic than PCT |
| Lumen | Relatively wider, more distinct than PCT |
| Location | Cortex — returns near glomerulus of origin |
| Function | Reabsorbs Na (aldosterone-sensitive); Ca²⁺ reabsorption (PTH) |
5. Collecting Duct
| Feature | Detail |
|---|
| Principal cells | Pale cytoplasm, respond to ADH (AQP2 insertion) and aldosterone |
| Intercalated cells (Type A) | Dark cytoplasm, secrete H⁺; reabsorb K⁺ |
| Intercalated cells (Type B) | Secrete HCO₃⁻ |
| Epithelium | Simple cuboidal → columnar in papillary duct |
📌 PCT vs DCT Comparison Table (High-Yield)
| Feature | PCT | DCT |
|---|
| Brush border | Yes (prominent) | No |
| Cell size | Larger | Smaller |
| Cytoplasm | Strongly eosinophilic | Pale/less eosinophilic |
| Lumen | Narrow, irregular | Wider, distinct |
| Mitochondria | Abundant (basal striations) | Moderate |
| % of cortex area | More numerous | Fewer |
📌 Juxtaglomerular Apparatus (JGA)
Components:
- JG cells — modified smooth muscle of afferent arteriole → secrete renin
- Macula densa — modified DCT cells sensing NaCl delivery
- Extraglomerular mesangial cells (lacis cells) — between JG cells and macula densa
Function: Regulates GFR (tubuloglomerular feedback) and systemic blood pressure (RAAS).
📌 Renal Interstitium
- Cortical interstitium: sparse, few fibroblasts
- Medullary interstitium: prominent fibroblasts that synthesize prostaglandins and erythropoietin
🧠 High-Yield MCQs — Histology of Kidney
Q1. The proximal convoluted tubule is distinguished histologically by:
- A) Wide clear lumen and pale cells
- B) Brush border and eosinophilic cytoplasm ✓
- C) Simple squamous epithelium
- D) Absence of mitochondria
Q2. Which cells of the kidney produce renin?
- A) Podocytes
- B) Juxtaglomerular (JG) cells ✓
- C) Macula densa cells
- D) Principal cells of collecting duct
JG cells are modified smooth muscle cells of the afferent arteriole.
Q3. The macula densa is located in which part of the nephron?
- A) Proximal convoluted tubule
- B) Ascending thick limb of Henle
- C) Distal convoluted tubule ✓
- D) Collecting duct
Q4. In a kidney cross section, tubules with NO brush border, pale cytoplasm, and wider lumens are most likely:
- A) Proximal convoluted tubules
- B) Distal convoluted tubules ✓
- C) Thick ascending loop of Henle
- D) Collecting ducts
Q5. Which cells in the collecting duct are responsible for water reabsorption in response to ADH?
- A) Principal cells ✓
- B) Type A intercalated cells
- C) Type B intercalated cells
- D) JG cells
Q6. The visceral layer of Bowman's capsule is composed of:
- A) Simple squamous epithelium
- B) Podocytes ✓
- C) Columnar epithelium
- D) Transitional epithelium
Q7. Which segment of the nephron is impermeable to water but actively transports NaCl?
- A) Descending thin limb of Henle
- B) Thick ascending limb of Henle ✓
- C) Collecting duct (without ADH)
- D) Proximal tubule
This is the "diluting segment" — impermeable to water, active NKCC2 transport builds medullary gradient.
Q8. Mesangial cells in the glomerulus are important because they:
- A) Filter blood
- B) Produce renin
- C) Are phagocytic and provide structural support ✓
- D) Reabsorb glucose
TOPIC 3: TUBULAR PROCESSING OF GLOMERULAR FILTRATE
📌 Key Concept
The kidney filters 180 L/day but excretes only ~1.5 L — reabsorbs 99% of the filtrate.
Tubular reabsorption is quantitatively large and highly selective — glucose and amino acids are 100% reabsorbed; waste products (urea, creatinine) are poorly reabsorbed.
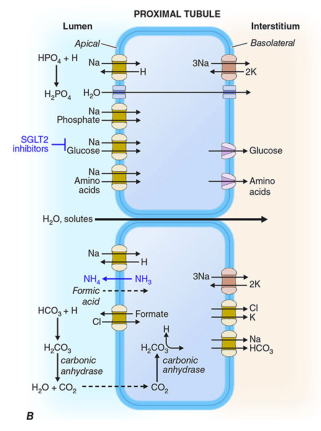
📌 Proximal Tubule — Bulk Reabsorption (~65–70%)
| Substance | % Reabsorbed | Mechanism |
|---|
| Na⁺ | ~65% | Na⁺/K⁺-ATPase (basolateral); passive via tight junctions |
| Water | ~65% (iso-osmotic) | Osmosis through AQP1 |
| Glucose | 100% (at normal plasma levels) | SGLT2 (apical), GLUT2 (basolateral) |
| Amino acids | ~100% | Na⁺-coupled cotransporters |
| HCO₃⁻ | ~80% | Na⁺/H⁺ exchange + carbonic anhydrase |
| Phosphate | ~80% | Na⁺-phosphate cotransporter (inhibited by PTH) |
| Urea | ~50% passive | Passive (follows water) |
| K⁺ | ~65% | Passive, paracellular |
Glucose Transport Maximum (Tm):
- Transport maximum for glucose = 375 mg/min
- Threshold plasma glucose = ~180 mg/dL → above this, glucose spills into urine (glucosuria)
📌 Loop of Henle — Countercurrent Mechanism
| Limb | Water | Solute |
|---|
| Descending thin | Permeable | Impermeable → fluid becomes concentrated |
| Ascending thin | Impermeable | Some passive NaCl diffusion |
| Thick ascending | Impermeable | Active NKCC2 transport (blocked by furosemide) |
→ Creates hypertonic medullary interstitium → essential for urine concentration
📌 Distal Tubule & Collecting Duct — Fine-Tuning
| Segment | Key Transporters | Regulated By |
|---|
| DCT | Na⁺-Cl⁻ cotransporter (NCC) | Aldosterone |
| DCT | Ca²⁺ reabsorption (TRPV5) | PTH, Vitamin D |
| Collecting duct principal cells | ENaC (Na), ROMK (K secretion) | Aldosterone |
| Collecting duct principal cells | AQP2 insertion | ADH (vasopressin) |
| Type A intercalated cells | H⁺-ATPase | Acid-base balance |
📌 Hormonal Control of Tubular Processing
| Hormone | Site of Action | Effect |
|---|
| Aldosterone | DCT + collecting duct | ↑ Na⁺ reabsorption, ↑ K⁺ secretion, ↑ H⁺ secretion |
| ADH (vasopressin) | Collecting duct | ↑ Water reabsorption via AQP2 |
| PTH | PCT + DCT | ↓ Phosphate reabsorption, ↑ Ca²⁺ reabsorption |
| Angiotensin II | PCT | ↑ Na⁺/H⁺ exchange → ↑ Na⁺ reabsorption |
| ANP/BNP | Collecting duct | ↓ Na⁺ reabsorption |
📌 Potassium Handling
- PCT: 65% reabsorbed passively
- Thick ascending: 25–30% reabsorbed via NKCC2
- Collecting duct: K⁺ secretion regulated by aldosterone
- Hypokalemia → ↓ K⁺ secretion; Hyperkalemia → ↑ K⁺ secretion via ROMK
📌 Urea Recycling
- ~50% reabsorbed in PCT passively
- Secreted in thin limbs of Henle
- Reabsorbed in collecting duct (facilitated by UT-A1 transporters, stimulated by ADH)
- Urea recycling contributes to medullary hypertonicity
📌 Acidification of Urine (H⁺ Secretion)
| Location | Mechanism | % of H⁺ |
|---|
| PCT | Na⁺/H⁺ exchanger (NHE3) | ~80% |
| Thick ascending | NHE3 | Small |
| Collecting duct Type A | H⁺-ATPase & H⁺/K⁺-ATPase | ~20% |
Buffers in urine: phosphate (titratable acid) and ammonia (NH₃ → NH₄⁺)
Figure: Proximal tubule apical and basolateral transporters — SGLT2, NHE3, Na-phosphate, Na-amino acid cotransporters (Harrison's)
🧠 High-Yield MCQs — Tubular Processing
Q1. At normal plasma glucose levels, glucose is:
- A) Filtered and 50% reabsorbed
- B) Completely reabsorbed in the proximal tubule ✓
- C) Secreted by the distal tubule
- D) Excreted in small amounts
SGLT2 in PCT reabsorbs all filtered glucose at plasma levels <180 mg/dL.
Q2. Furosemide (a loop diuretic) works by blocking:
- A) Na⁺/K⁺-ATPase
- B) NKCC2 in the thick ascending limb ✓
- C) ENaC in the collecting duct
- D) SGLT2 in the proximal tubule
Q3. Aldosterone primarily acts on which cells?
- A) JG cells
- B) Proximal tubule cells
- C) Principal cells of the collecting duct ✓
- D) Podocytes
Aldosterone → ↑ ENaC expression → ↑ Na⁺ reabsorption, ↑ K⁺ secretion.
Q4. ADH (vasopressin) increases water reabsorption by inserting which channel?
- A) AQP1
- B) AQP3
- C) AQP2 ✓
- D) ROMK
ADH → V2 receptor → cAMP → AQP2 insertion into apical membrane of principal cells.
Q5. A patient with plasma glucose of 250 mg/dL will have glucosuria because:
- A) Glucose is poorly filtered
- B) GLUT2 is saturated in the DCT
- C) The transport maximum (Tm) for glucose is exceeded ✓
- D) ADH inhibits glucose reabsorption
Q6. PTH acts on the kidney to:
- A) ↑ Phosphate reabsorption
- B) ↓ Phosphate reabsorption + ↑ Ca²⁺ reabsorption ✓
- C) ↑ Na⁺ reabsorption
- D) ↓ Water reabsorption
Q7. The descending thin limb of Henle is:
- A) Impermeable to water, permeable to NaCl
- B) Permeable to water, impermeable to NaCl ✓
- C) Permeable to both water and NaCl
- D) Active transporter of NKCC2
Descending limb: water leaves → fluid becomes concentrated. Ascending limb: NaCl leaves (active) → fluid becomes diluted.
Q8. Which formula is used to determine if net reabsorption or secretion occurred?
- A) GFR = (U_x × V̇)/P_x
- B) Filtered load = GFR × P_x; compare to excreted amount ✓
- C) Osmolality = 2 × [Na] + glucose/18 + BUN/2.8
- D) Clearance = U_x/P_x
If excreted < filtered → reabsorption; if excreted > filtered → secretion.
TOPIC 4: ANATOMY OF THE KIDNEY AND SUPRARENAL GLAND
📌 Position & Relations of the Kidney
| Feature | Right Kidney | Left Kidney |
|---|
| Vertebral level | T12–L3 | T12–L3 (slightly higher) |
| Peritoneal relation | Retroperitoneal | Retroperitoneal |
| Anterior relations | Liver, right flexure of colon, 2nd part of duodenum (no peritoneum) | Stomach, spleen, pancreas, left flexure of colon |
| Superior relation | Right suprarenal gland | Left suprarenal gland |
Key point: Right kidney is lower than the left (liver pushes it down). The right kidney is directly related to the 2nd part of duodenum (retroperitoneal, no peritoneum between them).
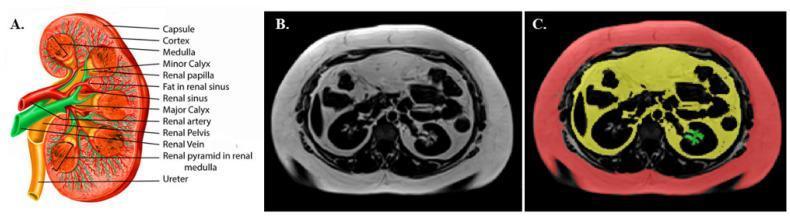
📌 External Anatomy
- Shape: Bean-shaped, ~11 cm × 6 cm × 3 cm
- Weight: 125–170 g (men); 115–155 g (women)
- Hilus: Medial concave border — entry of renal artery + nerves; exit of renal vein, lymphatics, ureter
- Renal sinus: Space inside hilus containing renal pelvis, calyces, vessels, fat
- Renal capsule: Fibrous, non-distensible
Figure: Coronal cross-section of kidney showing cortex, medulla (pyramids), calyces, renal pelvis, and ureter
📌 Internal Structure
| Layer | Contents |
|---|
| Cortex (outer, granular) | Glomeruli, PCT, DCT, cortical collecting ducts |
| Medulla (inner, striated) | Loops of Henle, collecting ducts, vasa recta |
| Renal pyramids (8–18) | Medullary cones, base at corticomedullary junction, apex = renal papilla |
| Renal columns (of Bertin) | Cortical tissue between pyramids |
| Minor calyx → Major calyx → Renal pelvis → Ureter | Urine drainage |
📌 Renal Blood Supply
Pathway:
Aorta → Renal artery → Segmental arteries → Interlobar arteries → Arcuate arteries (at corticomedullary junction) → Interlobular arteries → Afferent arterioles → Glomerular capillaries → Efferent arterioles → Peritubular capillaries / Vasa recta → venous drainage
| Feature | Note |
|---|
| Renal artery origin | Lateral aorta at L1–L2 |
| Right renal artery | Longer; passes posterior to IVC |
| Segmental arteries | End arteries — no anastomoses → infarcts are wedge-shaped |
| Vasa recta | Supply medulla; form countercurrent exchange system |
📌 Two Types of Nephrons
| Type | Location | Loop of Henle | Function |
|---|
| Cortical nephrons (85%) | Outer cortex | Short loop | General filtration |
| Juxtamedullary nephrons (15%) | Inner cortex | Long loop into deep medulla | Urine concentration via countercurrent |
📌 Renal Lymphatics & Nerves
- Lymph: follows renal vessels → paraaortic lymph nodes
- Nerves: Renal plexus (T10–L1) sympathetic fibers; renal pain referred to loin/groin (T10–L1 dermatomes)
📌 Suprarenal (Adrenal) Glands
| Feature | Right | Left |
|---|
| Shape | Pyramidal | Semilunar (crescent) |
| Position | Anteromedial to upper right kidney | Anteromedial to upper left kidney |
| Relation | IVC anteromedially; liver anteriorly | Aorta; left renal vein; splenic vessels |
| Weight | ~4 g | ~4 g |
Blood supply:
- Superior suprarenal artery → inferior phrenic artery
- Middle suprarenal artery → aorta
- Inferior suprarenal artery → renal artery
- Single suprarenal vein: Right → IVC; Left → left renal vein
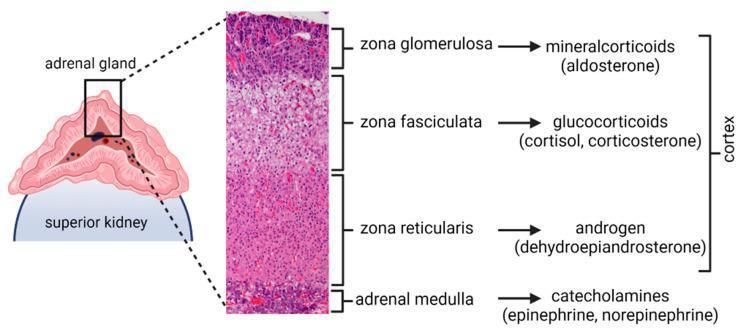
📌 Histology of the Suprarenal Gland
Figure: Adrenal gland zones — glomerulosa (mineralocorticoids), fasciculata (glucocorticoids), reticularis (androgens), medulla (catecholamines)
Mnemonic: GFR + M → "Go Find Receptor Medulla"
| Zone | Cells Arrangement | Hormone |
|---|
| Zona glomerulosa (outer) | Rounded clusters | Aldosterone (mineralocorticoid) |
| Zona fasciculata (middle, thickest) | Parallel cords; lipid-laden "spongiocytes" | Cortisol (glucocorticoid) |
| Zona reticularis (inner) | Anastomosing cords | Androgens (DHEA) |
| Medulla (innermost) | Chromaffin cells | Epinephrine (80%), Norepinephrine (20%) |
BMC HY: Zona fasciculata is the thickest zone. Chromaffin cells of the medulla are modified postganglionic sympathetic neurons. The right suprarenal vein drains directly into the IVC (clinically important in laparoscopic surgery).
🧠 High-Yield MCQs — Anatomy of Kidney and Suprarenal Gland
Q1. The kidneys lie at which vertebral level?
- A) L1–L4
- B) T12–L3 ✓
- C) T10–L1
- D) L2–L5
Q2. The right kidney is lower than the left because:
- A) The liver occupies the right upper quadrant ✓
- B) The right renal artery is longer
- C) The right suprarenal gland is larger
- D) The right ureter is shorter
Q3. The renal artery originates from the aorta at which level?
- A) T12
- B) L1–L2 ✓
- C) L3
- D) T10
Q4. Segmental arteries of the kidney are:
- A) Freely anastomosing
- B) End arteries ✓
- C) Branches of the renal vein
- D) Located in the renal pelvis
End arteries = no anastomoses → occlusion causes wedge-shaped infarction.
Q5. Cortical tissue extending between medullary pyramids is called:
- A) Minor calyx
- B) Renal sinus
- C) Columns of Bertin (renal columns) ✓
- D) Vasa recta
Q6. Juxtamedullary nephrons differ from cortical nephrons in that they:
- A) Lack a glomerulus
- B) Are more numerous (85%)
- C) Have longer loops of Henle extending into deep medulla ✓
- D) Do not have efferent arterioles
Q7. The left suprarenal vein drains into:
- A) Inferior vena cava
- B) Left renal vein ✓
- C) Aorta
- D) Left gonadal vein
Right suprarenal vein → IVC directly; Left suprarenal vein → left renal vein.
Q8. Which zone of the adrenal cortex is responsible for cortisol production?
- A) Zona glomerulosa
- B) Zona fasciculata ✓
- C) Zona reticularis
- D) Adrenal medulla
Q9. Which structure passes through the renal hilus?
- A) Renal artery, renal vein, ureter
- B) Renal artery and ureter only
- C) Renal artery, renal vein, ureter, lymphatics, and nerves ✓
- D) Ureter and renal vein only
Q10. The arcuate arteries of the kidney are located at:
- A) Cortical surface
- B) Corticomedullary junction ✓
- C) Renal sinus
- D) Deep medulla
Q11. Chromaffin cells of the adrenal medulla are embryologically derived from:
- A) Mesoderm (same as adrenal cortex)
- B) Neural crest cells ✓
- C) Endoderm
- D) Lateral plate mesoderm
Adrenal cortex → mesoderm; Adrenal medulla → neural crest (modified sympathetic neurons).
Q12. Which anterior relation of the right kidney has NO peritoneum between them?
- A) Liver
- B) 2nd part of duodenum ✓
- C) Right colic flexure
- D) Small intestine
The duodenum is also retroperitoneal, so it lies directly against the right kidney without a peritoneal layer.
📋 Quick Summary Table — All 4 Topics
| Topic | Most Tested Values/Facts |
|---|
| Glomerular Filtration | GFR = 125 mL/min; Inulin = gold standard; FF = 20%; Net filtration pressure ~10 mmHg |
| Kidney Histology | PCT = brush border + eosinophilic; DCT = no brush border, wide lumen; JG cells → renin; Macula densa = DCT |
| Tubular Processing | Glucose 100% reabsorbed (PCT, SGLT2); Tm glucose ~375 mg/min; threshold ~180 mg/dL; Aldosterone → Na reabsorption; ADH → AQP2 |
| Kidney & Suprarenal Anatomy | Kidneys T12–L3 retroperitoneal; Right kidney lower; Renal artery at L1–L2; End arteries; Right adrenal vein → IVC; Left → renal vein; Zona fasciculata = cortisol |
Sources: Guyton & Hall Textbook of Medical Physiology (9780443111013); Medical Physiology — Boron & Boulpaep (9780323319737); Harrison's Principles of Internal Medicine, 21st Ed.; Ganong's Review of Medical Physiology, 26th Ed.