peptic ulcer
Reading File
Finding Sources
Searching PubMed
"peptic ulcer"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Here is a comprehensive overview of peptic ulcer disease (PUD), synthesized from multiple authoritative textbooks.
Peptic Ulcer Disease (PUD)
Definition
A peptic ulcer is an ulcerative lesion of the gastric or duodenal mucosa caused by the erosive and digestive action of H⁺ and pepsin. Although the name implies pepsin involvement, acid is the essential driver - peptic ulcers do not occur in the absence of acid, and nearly all can be healed by proton pump inhibitors (PPIs) that render a patient virtually achlorhydric. - Bailey and Love's Short Practice of Surgery, 28th Ed.
Epidemiology
- More than 4 million individuals in the United States are treated annually
- Lifetime risk: ~10% in males, ~4% in females
- Duodenal ulcers are more common than gastric ulcers
- In the US, NSAID use is now the most common cause of gastric ulcers as H. pylori infection rates fall and low-dose aspirin use rises in the aging population - Robbins & Kumar Basic Pathology
Sites
- Most common: first part of the duodenum and lesser curve of the stomach
- May also occur at gastroenteric stoma (post-surgical), esophagus (from acid reflux), and in a Meckel's diverticulum (ectopic gastric epithelium)
- Ulcers tend to form at junctions between different epithelial types, in the epithelium least resistant to acid damage
Pathophysiology
PUD results from an imbalance between protective and damaging forces at the gastroduodenal mucosa.
Protective factors:
- Mucus gel barrier
- Bicarbonate (HCO₃⁻) secretion by epithelial cells - neutralizes H⁺ before it reaches cells
- Prostaglandin E₂ - maintains the barrier, stimulates HCO₃⁻ secretion
- Mucosal blood flow
- Growth factors
Damaging factors:
- H⁺ and pepsin
- Helicobacter pylori infection
- NSAIDs
- Stress, smoking, and alcohol
For a peptic ulcer to form, there must be: (1) loss of the protective mucous barrier, (2) excessive H⁺/pepsin secretion, or (3) both. - Costanzo Physiology, 7th Ed.
Aetiology
1. Helicobacter pylori
-
70% of PUD cases are associated with H. pylori
- H. pylori colonizes the gastric mucus (often antrum), attaches to epithelial cells, and releases cytotoxins (e.g., CagA toxin) that break down the protective mucous barrier
- It survives in acidic conditions by producing urease, converting urea to NH₃, which alkalinizes the local environment
- Gastric ulcers: barrier defect is primary; net H⁺ secretion is paradoxically lower (leaked into damaged mucosa), causing compensatory hypergastrinaemia
- Duodenal ulcers: H. pylori decreases antral somatostatin → hypergastrinaemia → parietal cell hyperplasia → hyperacidity → antral metaplasia in duodenum → H. pylori colonizes duodenum → impairs duodenal HCO₃⁻ secretion
Only 5-10% of infected individuals develop ulcers, suggesting host factors and strain variation matter.
2. NSAIDs
- Suppress prostaglandin synthesis → impair HCO₃⁻ secretion and mucosal blood flow → impair healing
- Low-dose aspirin is an increasingly important contributing factor in the elderly
3. Other Cofactors
- Cigarette smoking - reduces mucosal blood flow, increases relapse rate
- Corticosteroids - suppress prostaglandin synthesis
- Zollinger-Ellison syndrome - gastrin-secreting tumour (gastrinoma) causes massive, constitutive acid production; ulcers may occur in stomach, duodenum, and even jejunum
- Hypercalcaemia (hyperparathyroidism, renal failure) - stimulates gastrin production
- Alcohol-related cirrhosis, COPD, chronic renal failure - all associated with increased PUD risk - Robbins & Kumar Basic Pathology
Clinical Features
- Epigastric pain - gnawing or burning, often nocturnal
- Pain relieved by food or antacids (classic for duodenal ulcer)
- Duodenal and gastric ulcer symptoms are clinically indistinguishable
- Nausea is common
- Alarm symptoms requiring prompt endoscopy: weight loss, vomiting, melena/hematochezia, persistent symptoms despite treatment, age >50
Diagnosis
| Test | Notes |
|---|---|
| Endoscopy | Most sensitive; mandatory for alarm symptoms, age >50, gastric ulcers (to exclude malignancy) |
| Urea breath test | Sensitivity/specificity >90%; detects active infection; useful to confirm eradication |
| Stool antigen test | Detects active infection; recommended only with locally validated tests |
| Serology (IgG) | Diagnoses past or current infection; persists after eradication - NOT useful for confirming cure |
| Rapid urease test / biopsy | Invasive; used at endoscopy |
| ¹³C-urea breath test | Based on H. pylori urease converting ¹³C-urea to ¹³CO₂, which is exhaled and measured |
Source: Schwartz's Principles of Surgery, 11th Ed.; Harrison's Principles of Internal Medicine, 22nd Ed.
Treatment
Antisecretory Therapy
- PPIs are first-line (omeprazole, lansoprazole, etc.) - suppress H⁺/K⁺ ATPase (proton pump) irreversibly
- H₂ receptor antagonists (e.g., ranitidine, famotidine) - second-line
- NSAID-associated ulcer: stop the NSAID and begin a PPI (4-week course often sufficient)
H. pylori Eradication
Eradication is mandatory in H. pylori-positive PUD. Successful eradication eliminates ulcer recurrence and the need for long-term PPI. It also reduces rebleeding from 20% to ~3%.
Treatment regimens (Goldman-Cecil Medicine):
| Regimen | Components | Duration |
|---|---|---|
| Triple therapy (if clarithromycin resistance <15%) | PPI + clarithromycin + amoxicillin (or metronidazole) | 7-14 days |
| Bismuth quadruple therapy | PPI + bismuth + metronidazole + tetracycline | 7-14 days |
| Non-bismuth quadruple (concomitant) | PPI + amoxicillin + metronidazole + clarithromycin | 10-14 days |
| Salvage/rescue | PPI + amoxicillin + two alternative antibiotics (levofloxacin, rifabutin, etc.) | per sensitivity |
Treatment algorithm:
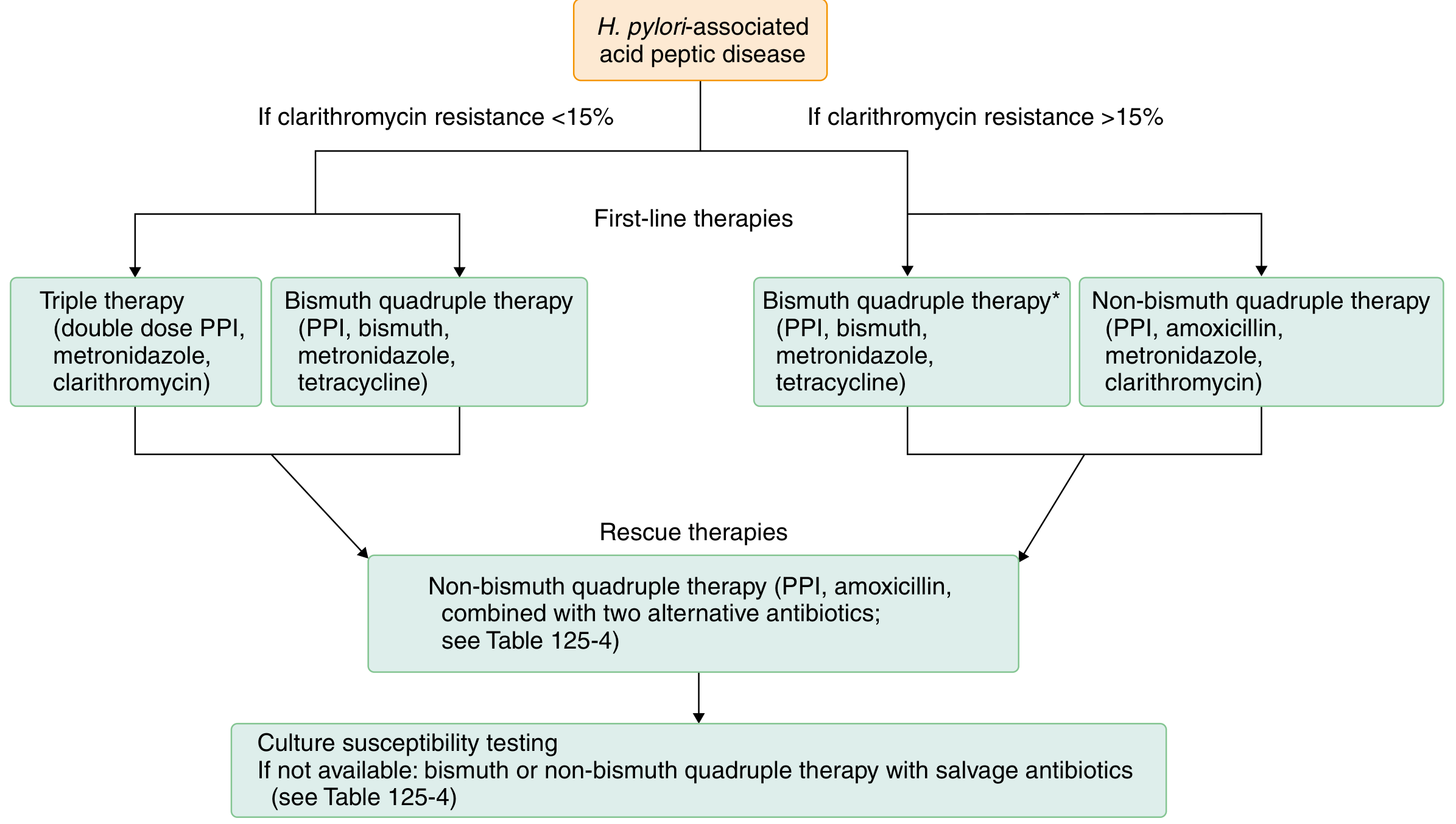
Key principle: If clarithromycin resistance >15% in the local area, bismuth quadruple or non-bismuth quadruple therapy is preferred over standard triple therapy.
Complications
| Complication | Key Points |
|---|---|
| Bleeding | Most common complication; Rockall score stratifies rebleeding/mortality risk |
| Perforation | Primarily surgical treatment; conservative management possible in selected cases |
| Gastric outlet obstruction (stenosis) | From fibrosis/oedema at pylorus |
| Malignancy | Gastric ulcers may be malignant - always biopsy; duodenal ulcers rarely malignant |
Rockall Score (for UGI bleed risk stratification): variables include age, pulse, blood pressure, comorbidities, diagnosis, and endoscopic stigmata. Score ≥8 carries ~41% rebleeding rate and ~41% mortality. - Sleisenger & Fordtran's GI and Liver Disease
Perforated Peptic Ulcer
- Treatment is primarily surgical (omental patch repair / closure)
- Some haemodynamically stable patients without peritoneal contamination may be managed conservatively
Surgery (Now Rarely Indicated)
With effective medical therapy, elective surgery for uncomplicated PUD is essentially obsolete. Surgery is reserved for:
- Perforation
- Uncontrolled haemorrhage unresponsive to endoscopic therapy
- Obstruction not responding to medical management
- Recurrent ulceration despite maximal medical therapy
Gastric vs. Duodenal Ulcer: Summary
| Feature | Gastric Ulcer | Duodenal Ulcer |
|---|---|---|
| Mechanism | Mucosal barrier defect (primary) | Excess H⁺ secretion (primary) |
| Acid secretion | Normal or low | High |
| H. pylori association | Common | Very common |
| Malignancy risk | Yes - must biopsy | Rare |
| Pain timing | Food may worsen | Food relieves (classic) |
| Relative frequency | Less common | More common |
Sources: Costanzo Physiology 7th Ed.; Bailey & Love Surgery 28th Ed.; Robbins & Kumar Basic Pathology; Schwartz's Surgery 11th Ed.; Goldman-Cecil Medicine; Harrison's Principles of Internal Medicine 22nd Ed.
Recent evidence note: A 2024 meta-analysis (PMID: 38818853) found endoscopic therapy is superior to medical management alone for peptic ulcers with adherent clots. A 2025 Cochrane review (PMID: 40337979) confirmed PPIs are effective for preventing NSAID-induced ulcers. Increasing clarithromycin resistance is a recognized cause of triple therapy failure (PMID: 40132025 - pharmacist-led interventions improve eradication outcomes).
Pseudo membranous cholitis
Finding Sources
Searching PubMed
"Clostridioides difficile" AND colitis
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive information from Harrison's (22nd Ed.), Robbins & Kumar, Jawetz Microbiology, and Grainger & Allison's Radiology. Here is the full review.
Pseudomembranous Colitis (PMC)
Definition
Pseudomembranous colitis (PMC) is the most severe form of Clostridioides difficile infection (CDI) - a unique colonic disease acquired most commonly in association with antimicrobial use and the consequent disruption of normal colonic microbiota. It is the most commonly diagnosed diarrheal illness acquired in the hospital in the United States. - Harrison's Principles of Internal Medicine, 22nd Ed.
Organism
- Clostridioides difficile (formerly Clostridium difficile) - obligately anaerobic, gram-positive, spore-forming bacillus
- Spores are found widely in nature - especially in hospital and chronic-care facility environments, where they can persist for months on surfaces
- Spores survive gastric acid, germinate in the small bowel, and colonize the lower intestinal tract when microbiota is disrupted
Epidemiology
- Estimated 462,100 cases in the US in 2017 (most common healthcare-associated infection)
- Rate of fecal colonization is ~1-3% in community residents vs. ≥20% in adults hospitalized >2 weeks
- CDI burden decreased by 24% between 2011-2017, primarily due to reductions in healthcare-associated cases; community-associated CDI rates were unchanged
- Asymptomatic fecal carriage in healthy neonates is very common - infants rarely develop disease (lack mucosal toxin receptors)
- Hospital epidemics can be attributed to a single strain or multiple simultaneous strains
Risk Factors
| Category | Factors |
|---|---|
| Antibiotics | Clindamycin, ampicillin, cephalosporins (2nd/3rd gen), fluoroquinolones; all antibiotics carry some risk |
| Host factors | Age >65, severe underlying illness, GI surgery, immunosuppression |
| Healthcare exposure | Hospitalization, nursing home residence, electronic rectal thermometers, enteral tube feeding |
| Medications | PPI use (modest risk, mainly relevant if already on antibiotics), antacids |
The lowest-risk beta-lactams are penicillin/beta-lactamase inhibitor combinations (e.g., piperacillin/tazobactam).
Pathogenesis
Three sequential events are required for CDI to develop:
- Antibiotic exposure - disrupts normal gut microbiota, creating susceptibility
- Exposure to toxigenic C. difficile - via spore ingestion (hand-to-mouth in hospital environment)
- Inadequate host immune response - (most patients after events 1+2 do NOT develop CDI; a strong IgG antibody response to toxin A is protective)
The Two Main Toxins
| Toxin | Type | Mechanism |
|---|---|---|
| Toxin A | Enterotoxin | Potent neutrophil chemoattractant; glucosylates Rho GTPases; disrupts actin cytoskeleton |
| Toxin B | Cytotoxin | More important virulence factor (toxin A-negative/toxin B-positive strains cause disease; reverse is not true); glucosylates Rho GTPases |
Both toxins cause:
- Loss of cell shape, adherence, and tight junctions
- Fluid leakage → diarrhea
- Cytokine release, apoptosis, capillary leakage
- Pseudomembrane formation
A third toxin - binary toxin CDT - is present in all isolates of the epidemic NAP1/BI/027 hypervirulent strain (responsible for recent global outbreaks). - Jawetz Microbiology 28th Ed.; Harrison's 22nd Ed.
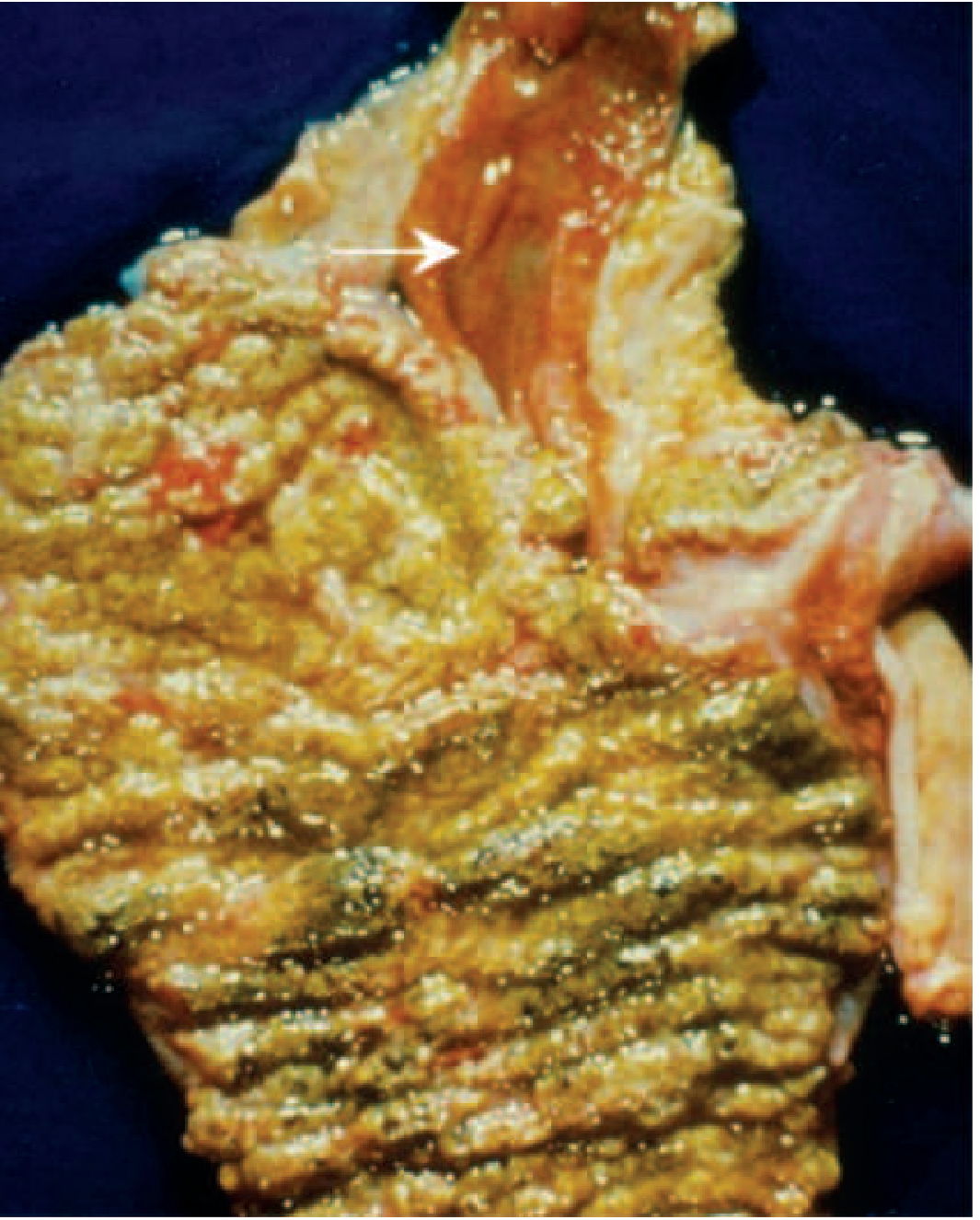
Pathology / Morphology
Gross Appearance
- Pseudomembranes initially appear as 1-2 mm whitish-yellow plaques confined to colonic mucosa
- Intervening mucosa appears unremarkable early on
- As disease progresses, plaques coalesce into larger, confluent membranes covering the entire colon wall
- Whole colon is usually involved; 10% of patients have rectal sparing
- Transverse colon is the most frequently affected segment on imaging
Autopsy specimen showing confluent pseudomembranes covering the cecum (note terminal ileum sparing, arrow):
Microscopic Appearance
- Surface epithelium is denuded and necrotic in focal areas
- Superficial lamina propria has dense neutrophil infiltrate with occasional fibrin thrombi in capillaries
- Damaged crypts are distended by mucopurulent exudate that "erupts" to the surface - classic "volcano" or "summit" lesion appearance
Endoscopic (A) and histological (B) views - note the tan pseudomembranes and the volcano-eruption pattern from crypts:
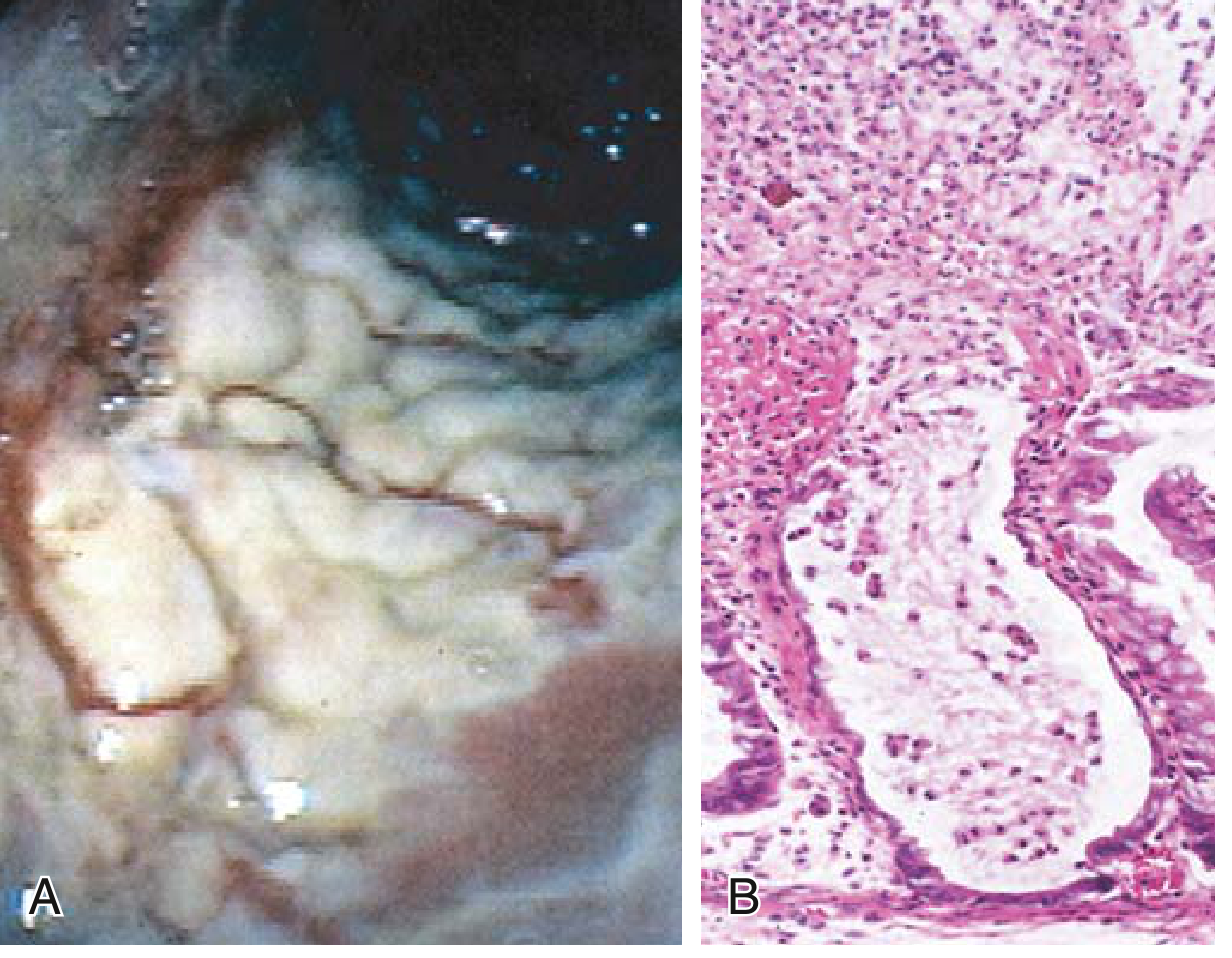
- Robbins & Kumar Basic Pathology
Clinical Features
| Feature | Description |
|---|---|
| Watery diarrhea | Most common presentation; may be >10 stools/day |
| Abdominal cramping | Common |
| Fever | Present in more severe cases |
| Leukocytosis | Hallmark; WBC ≥15,000 common; ≥20,000 suggests fulminant disease |
| Dehydration | From profuse diarrhea |
| Fecal leukocytes / occult blood | May be present |
| Grossly bloody diarrhea | Rare |
Fulminant CDI
- ~5% of cases; carries high mortality
- Patient may lack diarrhea - mimics acute surgical abdomen
- Sepsis (hypotension, fever, tachycardia), toxic megacolon, ileus, colon perforation
- Peripheral leukocytosis ≥20,000 WBCs/μL is a warning sign
Diagnosis
| Test | Notes |
|---|---|
| Nucleic acid amplification test (NAAT/PCR) | Detects toxin A/B genes; highly sensitive; positive alone = colonization, not necessarily disease |
| Stool toxin EIA (enzyme immunoassay) | Detects toxin A and/or B; positive in disease context = CDI |
| Two-step algorithm | NAAT + toxin EIA together - positive on both = active CDI |
| Anaerobic toxigenic culture | Gold standard for research; too slow for clinical use |
| Sigmoidoscopy/colonoscopy | Visualizes pseudomembranes; useful in patients without diarrhea (fulminant) |
| Abdominal CT | Non-specific; markedly thickened mucosa, submucosal oedema, "accordion sign" (nodular mucosal thickening), pericolic fat stranding, ascites in ~40%; CT normal in ~39% of cases |
| Plain AXR | Abnormal in ~1/3 of cases; colonic dilatation, thumbprinting, thickened haustra |
- Grainger & Allison's Diagnostic Radiology; Jawetz Microbiology 28th Ed.
Treatment
Step 1 - Stop the offending antibiotic (if possible)
Step 2 - Antibiotic therapy based on severity
| Severity | Treatment |
|---|---|
| Mild-moderate | Oral vancomycin 125 mg QID × 10 days, OR oral fidaxomicin 200 mg BID × 10 days |
| Severe (WBC ≥15,000 or Cr rise) | Oral vancomycin (preferred over metronidazole) |
| Fulminant | Oral/NG vancomycin + IV metronidazole; consider vancomycin retention enema if ileus present |
Metronidazole is NOT recommended for recurrent CDI and has been deprioritized even in initial treatment due to higher failure rates.
Fidaxomicin is superior to vancomycin in reducing recurrence (especially in patients with one prior CDI episode).
Recurrent CDI (15-30% of patients after initial treatment)
| Option | Notes |
|---|---|
| Vancomycin tapered/pulsed | e.g., QID × 10-14 d, then BID × 7 d, then daily × 7 d, then every-other-day × 2-8 weeks |
| Fidaxomicin extended/pulsed | Superior to vancomycin in reducing further recurrences |
| Vancomycin followed by rifaximin | "Chaser" strategy |
| Fecal Microbiota Transplantation (FMT) | Via colonoscopy, nasoduodenal tube, enema, or oral capsules; highly effective for multiple recurrences |
| Rebyota (live-jslm) | FDA-approved microbiota suspension - adjunctive, after completing antibiotics |
| Vowst (live-brpk) | FDA-approved oral spore suspension - adjunctive, for recurrent CDI prevention |
| Bezlotoxumab | Monoclonal antibody against toxin B; reduces rCDI risk by ~10% absolute when given with standard antibiotics in high-risk patients |
Surgical Management (Fulminant CDI)
- Colectomy if no response to medical management
- Best performed before serum lactate reaches 5 mmol/L
- Loop ileostomy with colonic lavage is an alternative that preserves the colon
Complications
| Complication | Notes |
|---|---|
| Recurrence | 15-30% after first episode; risk increases with each recurrence |
| Toxic megacolon | Colonic dilatation >6 cm; risk of perforation |
| Colonic perforation | Life-threatening |
| Sepsis / septic shock | Especially in fulminant disease |
| Death | Up to 11% risk of serious complications with recurrent disease; ~30-day mortality significant in elderly |
Infection Control / Prevention
- Contact precautions (gown + gloves) for all CDI patients
- Hand hygiene with soap and water (alcohol-based hand rubs do NOT kill spores)
- Environmental decontamination with hypochlorite (bleach)-based disinfectants
- Antibiotic stewardship - reducing unnecessary antibiotic use is the most effective preventive measure
- Probiotics have been studied but evidence is not strong enough for routine recommendation
Key Distinguishing Points
| Feature | PMC / CDI |
|---|---|
| Causative organism | Clostridioides difficile |
| Classic trigger | Recent antibiotic use (any class) |
| Hallmark morphology | Volcano/summit lesion; confluent pseudomembranes |
| Key toxins | Toxin A (enterotoxin) + Toxin B (cytotoxin) |
| Key lab finding | Leukocytosis (WBC often very high) |
| Diagnosis | NAAT + stool toxin EIA |
| First-line treatment | Oral vancomycin or fidaxomicin |
| Recurrence management | Fidaxomicin, FMT, Rebyota/Vowst |
Sources: Harrison's Principles of Internal Medicine 22nd Ed.; Robbins & Kumar Basic Pathology; Jawetz Melnick & Adelberg's Medical Microbiology 28th Ed.; Grainger & Allison's Diagnostic Radiology
Recent evidence note (2025): A 2025 Cochrane-level meta-analysis (PMID: 41047657) found that PPIs alone (without antibiotics) are NOT associated with increased CDI risk - clarifying a long-debated question. IBD patients remain a higher-risk group (PMID: 39448963).
This is a shared conversation. Sign in to Orris to start your own chat.