Vitiligo
Reading File
Finding Sources
Searching PubMed
vitiligo
Searching the Web
vitiligo pathophysiology treatment 2025 2026 guidelines
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have comprehensive textbook content and images. Let me compile the full, well-structured response.
Vitiligo
Definition
Vitiligo is an acquired, autoimmune skin disease characterized by progressive loss of epidermal melanocytes, resulting in well-demarcated milky-white macules and patches. Hair within affected areas may also depigment (poliosis/leukotrichia). It affects approximately 0.5-1% of the world population, with some regions of India reporting prevalence above 8%.
- Dermatology 2-Volume Set 5e, p. 1307
- Andrews' Diseases of the Skin, p. 1001
Epidemiology
- Prevalence: ~0.5-1% globally
- Peak onset: ages 10-30; ~50% of cases begin before age 20
- No definitive sex predilection, though females are over-represented in clinical populations (possibly due to greater healthcare-seeking behavior)
- Up to 30% of patients have an affected first-degree relative; 7% of first-degree relatives of probands have vitiligo
- Monozygotic twin concordance ~23%, confirming additional environmental contribution
- Fitzpatrick's Dermatology, p. 1360; Dermatology 2-Volume Set 5e, p. 1307
Pathogenesis
Vitiligo pathogenesis is multifactorial, involving genetic susceptibility, melanocyte intrinsic defects, oxidative stress, and adaptive autoimmunity.
Key Pathway (IFN-γ → JAK-STAT → CXCL9/10 Axis)
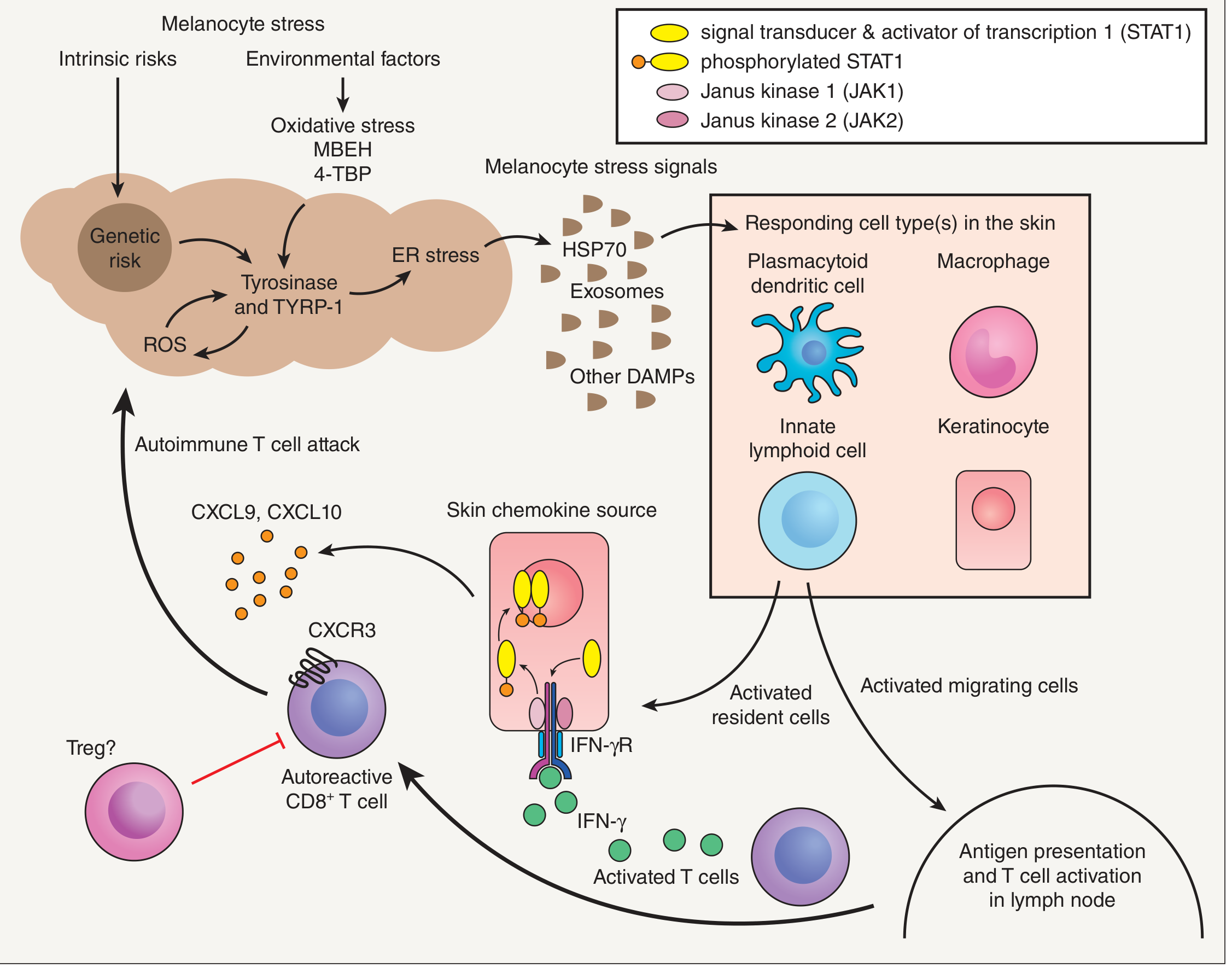
The sequence of events:
- Genetic risk + environmental triggers (oxidative stress, chemical exposures such as MBEH or 4-tertiary butyl phenol) cause melanocyte stress - including ER stress, ROS generation, and tyrosinase/TYRP-1 abnormalities
- Stressed melanocytes release DAMPs (HSP-70, HMGB1, exosomes) into the skin
- DAMPs activate plasmacytoid dendritic cells and innate lymphoid cells, which secrete IFN-α and IFN-γ
- IFN-γ signals through its receptor (IFN-γR) on keratinocytes via JAK1/JAK2 → STAT1 phosphorylation
- Phosphorylated STAT1 drives transcription of CXCL9 and CXCL10
- CXCL9/10 recruit autoreactive CD8+ T cells expressing CXCR3 to the skin
- These T cells kill melanocytes through direct cytotoxicity
- Resident memory T cells (CD69+, CD103+, CD49a+) persist in lesional skin, explaining disease relapse at the same sites after treatment
Additional mechanisms:
- Impaired WNT/β-catenin signaling reduces melanocyte precursor differentiation, limiting repigmentation
- Regulatory T cells (Tregs) appear insufficient to suppress the autoreactive response
- Dermatology 2-Volume Set 5e, p. 1307-1308
Clinical Features
Lesion Characteristics
- Well-defined, milky-white macules with smooth, convex margins
- Surrounding skin may be normal or hyperpigmented
- Trichrome vitiligo: three zones - depigmented, intermediate tan, and normal - seen in early disease
- Inflammatory border (red): rare, indicates active disease
- Poliosis: white hairs within lesions (follicular melanocyte loss)
- Depigmented lesions are chalk-white under Wood's lamp (fluoresce bright white), which helps distinguish from hypopigmentation
Subtypes and Distribution
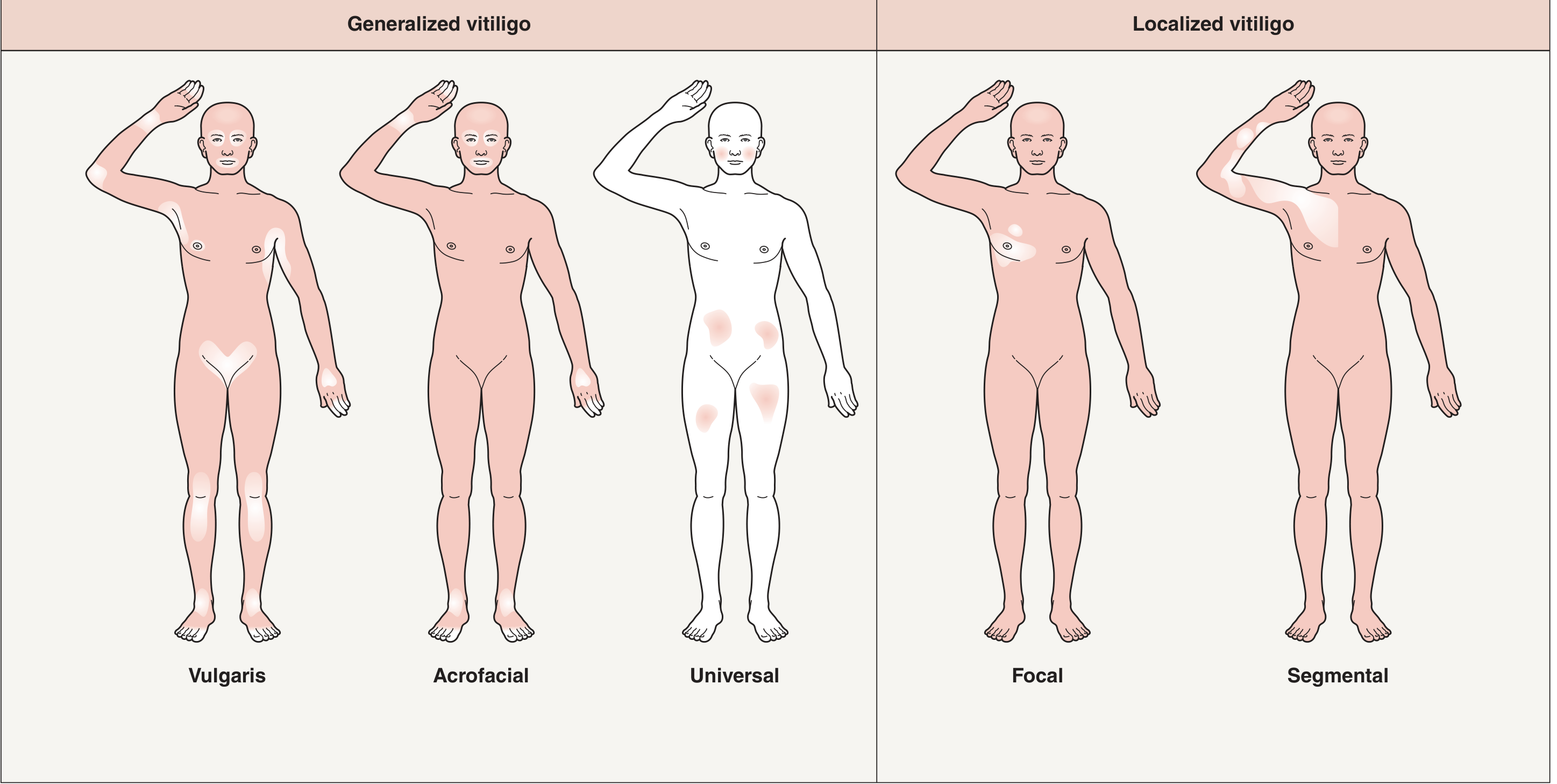
| Type | Description |
|---|---|
| Vulgaris (generalized) | Most common; bilateral, symmetric patches |
| Acrofacial | Distal fingers and facial orifices (lips, periocular) |
| Universal | Near-total body depigmentation |
| Focal | Single or few macules in one area (non-dermatomal) |
| Segmental | Unilateral, block-shaped, along a dermatome-like segment; spreads rapidly over 6-12 months then stabilizes; often involves follicular melanocytes early (poliosis) |
| Mucosal | Lips, genitalia, oral mucosa |
| Mixed | Segmental + non-segmental elements |
Predilection sites: periocular, perioral, dorsal hands, axillae, groin, elbows, knees, nipples, umbilicus, genitalia, anus - areas of friction and around orifices.
Markers of Active Disease (Important for Treatment Timing)
- Confetti lesions: small guttate white spots - indicate rapid spread
- Koebner phenomenon: new lesions at sites of trauma
- Trichrome lesions: intermediate pigmentation zones
- Inflammatory/erythematous border
- Fitzpatrick's Dermatology, p. 1361
Histopathology
- Complete absence of melanocytes (confirmed by S100 or MART-1/Melan-A staining)
- Usually no inflammatory infiltrate in established lesions
- Lichenoid or spongiotic inflammation at the margins of active lesions
- This explains the occasional scaling or hyperpigmentation around lesion borders
- Andrews' Diseases of the Skin, p. 1001
Differential Diagnosis
| Condition | Distinguishing Features |
|---|---|
| Pityriasis alba | Fine scale, poorly defined margins, slightly papular |
| Tinea versicolor | Fine scale, favors central trunk/back, KOH shows hyphae/yeast |
| Morphea / Lichen sclerosus | Hypopigmented (not depigmented), altered skin texture |
| Pityriasis lichenoides | Scaling papules, history of rash |
| Chemical leukoderma | Occupational history, phenol/catechol exposure; may closely mimic vitiligo |
| Hypopigmented mycosis fungoides | Biopsy needed |
| Post-inflammatory hypopigmentation | History, less well-defined, lighter (not chalk-white) |
Wood's lamp is key: True vitiligo is depigmented (bright white glow), not merely hypopigmented.
- Andrews' Diseases of the Skin, p. 1001
Associations
- Other autoimmune diseases: thyroid disease (Hashimoto's thyroiditis, Graves'), alopecia areata, rheumatoid arthritis, pernicious anemia, type 1 diabetes, lupus, Addison's disease
- Decreased risk of skin cancer (melanoma and keratinocyte cancers) - a protective immune surveillance effect
- Psychiatric comorbidity: anxiety, depression, significant impairment in quality of life; should be assessed and documented at every visit
- Up to 65% of patients in Europe have been told their disease is untreatable - a major management gap
- Fitzpatrick's Dermatology; Andrews' Diseases of the Skin
Treatment
Treatment has two goals: (1) stopping progression, and (2) inducing repigmentation. Many treatments do one but not both. Response is slow - weeks to months. Areas with pigmented hair follicles respond better (hair follicles serve as a melanocyte reservoir for repigmentation).
Predictors of Response
- Favorable: face, trunk, areas with high follicular density, pigmented hairs still present in lesional skin, early/active disease
- Unfavorable: hands/feet (acral), mucosae, leukotrichia (white hairs), long-standing disease, segmental vitiligo
1. Topical Corticosteroids
- First-line for localized disease
- Mid- to high-potency agents (e.g., mometasone, clobetasol)
- Risk: skin atrophy, telangiectasias with prolonged use
- Useful for stopping progression
2. Topical Calcineurin Inhibitors (TCIs)
- Tacrolimus 0.1% or pimecrolimus 1% cream
- Preferred for face and flexural areas (fewer atrophy concerns than steroids)
- Effective for halting progression and some repigmentation
- Often combined with phototherapy
3. JAK Inhibitors (emerging/approved)
- Ruxolitinib cream 1.5% (topical JAK1/JAK2 inhibitor): FDA-approved (2022) for non-segmental vitiligo in patients ≥12 years old; first and only FDA-approved topical treatment specifically for vitiligo
- Targets the IFN-γ-JAK-STAT-CXCL9/10 axis directly
- Enhanced repigmentation reported with ruxolitinib cream + NB-UVB combination
- Oral JAK inhibitors (e.g., ritlecitinib, baricitinib) under investigation
- Dermatology 2-Volume Set 5e, p. 2810; off-label ruxolitinib systematic review PMID 40192197
4. Narrowband UVB Phototherapy (NB-UVB)
- Now the gold standard phototherapy for generalized/widespread vitiligo
- Superior to oral PUVA in efficacy and side-effect profile; better color matching of repigmented skin
- Typically 2-3 sessions/week; response assessed after 3-6 months
- Initial dose: 70% of the MED in lesional (depigmented) skin; increase carefully by 5-20% weekly based on barely perceptible erythema
- Important: depigmented skin has increased photosensitivity - dosing must be careful to avoid Koebner phenomenon from burns
- Dermatology 2-Volume Set 5e, p. 2809-2810
5. PUVA (Psoralen + UVA)
- Oral or topical psoralen followed by UVA
- More side effects than NB-UVB (nausea, photocarcinogenesis risk, cataract risk)
- Reserved for cases unresponsive to NB-UVB or where NB-UVB is unavailable
6. Systemic Corticosteroids
- Short pulse courses for rapidly progressive, generalized vitiligo to halt progression
- Not for long-term use
7. Afamelanotide + NB-UVB
- Afamelanotide (α-MSH analogue, subcutaneous implant) + NB-UVB: significantly superior and faster repigmentation vs. NB-UVB alone in RCT
- Effect more pronounced in Fitzpatrick skin types IV-VI
- Dermatology 2-Volume Set 5e, p. 2810
8. Surgical Options
- For stable vitiligo (no progression for ≥1 year)
- Autologous skin grafting (split-thickness, punch grafting, suction blister grafting)
- Melanocyte-keratinocyte transplantation procedure (MKTP)
- Segmental vitiligo often responds well to surgery due to its stability
9. Depigmentation
- For patients with near-universal vitiligo (>80% BSA), depigmentation of remaining skin with monobenzyl ether of hydroquinone (MBEH) or Q-switched laser can achieve a uniform appearance
- Irreversible
Monitoring and Investigations
- TSH, anti-TPO antibodies: screen for thyroid disease at diagnosis and periodically
- Fasting blood glucose: screen for type 1 diabetes
- CBC: screen for pernicious anemia (if suspected)
- ANA: if systemic autoimmune features present
- Psychological assessment: quality of life tools (VASI, SAVES, VIP/VIS scales)
- EADV 2025 Global Guidelines recommend formal QoL assessment at every visit, given the significant psychosocial burden
Key Points Summary
| Feature | Detail |
|---|---|
| Prevalence | 0.5-1% worldwide |
| Mechanism | CD8+ T cell destruction of melanocytes via IFN-γ/JAK/CXCL9-10 axis |
| Most common type | Generalized vulgaris (bilateral, symmetric) |
| First-line topical | Corticosteroids; calcineurin inhibitors (face/flexures) |
| Newest approved Rx | Ruxolitinib 1.5% cream (topical JAK inhibitor, FDA 2022) |
| Best phototherapy | NB-UVB (superior to PUVA, fewer side effects) |
| Reversibility | Only where follicular melanocyte reservoir intact (pigmented hairs) |
| Associated diseases | Thyroid, alopecia areata, T1DM, pernicious anemia |
| Decreased risk | Skin cancer (melanoma + keratinocyte) |
Sources: Fitzpatrick's Dermatology (Ch. 76); Dermatology 2-Volume Set 5e (Ch. 66, Ch. 134); Andrews' Diseases of the Skin (Ch. 36); EADV/Global Vitiligo Task Force 2025 Guidelines; ruxolitinib off-label systematic review (PMID 40192197)
This is a shared conversation. Sign in to Orris to start your own chat.