Nephritic syndrome
Reading File
search_medical_text
nephritic syndrome etiology pathophysiology clinical features
search_medical_text
nephritic syndrome diagnosis management treatment glomerulonephritis
search_medical_image
nephritic syndrome glomerulonephritis pathology
GradeResponse
GradeResponse
GradeResponse
Nephritic syndrome is a clinical syndrome caused by inflammatory injury of the glomeruli, classically presenting with:
- Hematuria (often cola/tea-colored urine, RBC casts)
- Hypertension
- Azotemia (acute kidney injury pattern)
- Oliguria
- Mild to moderate proteinuria (usually less than nephrotic range)
- Edema (often periorbital)
A classic morphologic correlate is proliferative GN with possible crescents on biopsy, as seen in pathology references on rapidly progressive GN ([webpathology image description]).
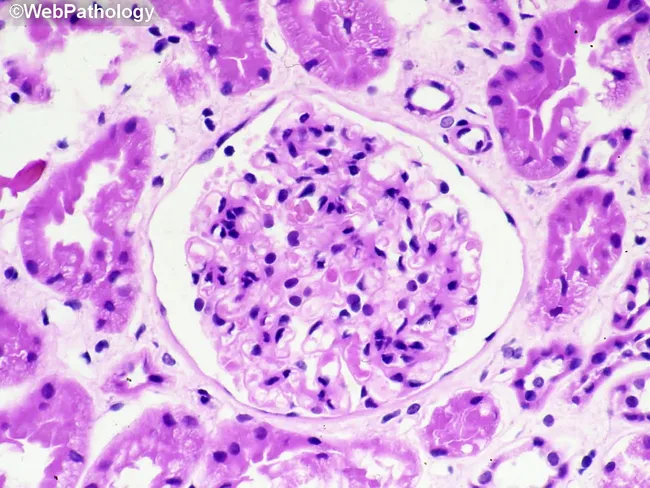
Source: webpathology (image record on crescentic glomerular injury)
Common causes (by mechanism)
- Post-infectious / infection-related GN
- IgA nephropathy / IgA vasculitis
- Lupus nephritis
- ANCA-associated pauci-immune GN
- Anti-GBM disease (Goodpasture spectrum)
- Membranoproliferative/C3 glomerulopathy (complement-mediated)
KDIGO 2021 provides disease-specific diagnostic and treatment pathways across these glomerular disorders (KDIGO Glomerular Diseases Guideline update, Management of Glomerular Diseases, p. 27).
Diagnostic approach
- Urinalysis + microscopy: dysmorphic RBCs, RBC casts, proteinuria
- Renal function: creatinine, BUN, electrolytes
- Serology guided by suspicion:
- C3/C4
- ASO/anti-DNase B (post-strep context)
- ANA, anti-dsDNA (lupus)
- ANCA
- Anti-GBM antibodies
- Hepatitis B/C, HIV when indicated
- Kidney biopsy in most significant/rapidly progressive cases to define subtype and urgency of immunosuppression
Management principles
- Supportive care for all:
- Salt/fluid restriction
- Loop diuretics for edema
- BP control (often RAAS blockade when appropriate)
- Treat triggers (eg, active infection)
- Cause-specific immunotherapy when indicated:
- High-dose steroids ± cyclophosphamide/rituximab for severe crescentic immune GN (depending on subtype)
- Plasmapheresis in selected anti-GBM disease/severe pulmonary hemorrhage contexts
- Lupus/ANCA/IgA regimens tailored to biopsy and severity
KDIGO emphasizes structured diagnosis, risk stratification, and subtype-specific therapy rather than one uniform regimen for all nephritic presentations (KDIGO 2021 guideline update, p. 27).
Nephritic vs nephrotic (quick contrast)
- Nephritic: inflammatory, hematuria + HTN + AKI, less proteinuria
- Nephrotic: heavy proteinuria, hypoalbuminemia, generalized edema, hyperlipidemia
If you want, I can give you a one-page exam-style table of nephritic causes with complement levels, IF patterns, and key serologies.
This is a shared conversation. Sign in to Orris to start your own chat.