Pfn
It looks like your message got cut off! Did you mean to type something specific? Here are a few possibilities:
- PFN (Profilin) - a protein involved in actin polymerization
- PFN (Peripheral Facial Nerve) - a clinical/anatomical topic
- PFN (Proximal Femoral Nail) - an orthopedic implant
- Pfn as an abbreviation for something else entirely
Could you clarify what you're looking for? I'm happy to help once I know what you mean!
PFN -nailing
Reading File
Finding Sources
Finding Sources
Searching the Web
PFN proximal femoral nailing technique indications complications orthopedics
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have enough comprehensive information to write a detailed answer. Let me compile it.
Proximal Femoral Nail (PFN) - Nailing
The PFN is a cephalomedullary intramedullary (IM) nail designed for fixation of proximal femoral fractures. It is inserted antegrade through the greater trochanter and secured into the femoral head-neck fragment with one or two proximal screws.
Indications
Standard (short) PFN:
- Pertrochanteric fractures
- Intertrochanteric fractures (all types; mandatory for unstable fractures)
- Reverse oblique fractures (31-A3)
- Comminuted fractures with loss of medial support
- Fractures without an intact lateral femoral cortex (lateral wall <20.5 mm)
- Subtrochanteric extension
- High subtrochanteric fractures
Long PFN:
- Low and extended subtrochanteric fractures
- Ipsilateral trochanteric + femoral shaft fractures
- Combination trochanteric area/shaft fractures
- Pathological fractures
Why PFN over DHS (Dynamic Hip Screw)?
- Less collapse than SHS plate devices due to the IM buttress effect
- Lower risk of lateral wall fracture
- Better biomechanics for unstable fracture patterns
- Less blood loss and shorter operative time in some series
(Campbell's Operative Orthopaedics 15th Ed., block31)
Classification of Fractures (AO/OTA)
| Type | Description | Stability |
|---|---|---|
| 31-A1 | Single fracture line, no comminution | Stable |
| 31-A2 | Comminuted, separate lesser trochanter fragment | Unstable |
| 31-A3 | Reverse oblique, transverse, or subtrochanteric extension | Very unstable |
PFN/cephalomedullary nail is the implant of choice for A2 and A3 fractures.
Implant Design (Classic AO PFN)
| Component | Detail |
|---|---|
| Nail diameter | Proximal 17 mm; distal 10/11/12 mm |
| CCD angle | 125°, 130°, or 135° |
| Femoral neck screw | 11.0 mm, self-tapping, 80-120 mm |
| Anti-rotation hip pin | 6.5 mm, self-tapping, 55-100 mm |
| ML angle | Anatomical 6° |
| Distal locking bolt | 4.9 mm |
Patient Positioning
- Supine on a fracture table with traction applied
- Affected limb in slight internal rotation (10-15°) and traction
- Hip in 20-30 degrees of flexion
- Fluoroscopy placed contralateral side or between the legs
- Closed reduction confirmed in AP and lateral views - check for:
- Varus deformity
- Posterior sag
- Excessive internal rotation (especially when greater trochanter is detached from distal segment)
Surgical Technique (Step-by-Step)
Entry Point
- Incision at or just proximal to the greater trochanteric tip
- Entry point: tip of greater trochanter (for standard PFN) or slightly medial to the piriformis fossa (for piriformis entry nails)
- Entry in line with the IM canal in both AP and lateral views
Nail Insertion
- Insert ball-tipped guide pin down the femoral canal to the physeal scar; measure for nail length
- Ream sequentially to 1.5 mm larger than nail diameter (typically 10-mm nail → ream to 11.5 mm)
- If anterior bow of femur is significant, ream 2 mm over nail diameter
- Assemble nail and insert with guide facing anteriorly to use the bow of the nail
- Rotate guide laterally after nail is ~halfway down the canal
- Monitor with lateral fluoroscopy throughout to avoid anterior cortical perforation
- Evaluate anteversion - nail, guide, and femoral head/neck must all be aligned on lateral view
Nail Angle Selection
- Prefer 130° nail as a default
- Nails with CCD angle less than the native neck-shaft angle (NSA) → risk of varus malreduction
- Measure contralateral hip NSA fluoroscopically for reference
Proximal Screw Placement
- Small lateral incision through skin and fascia
- Drill sleeve placed on lateral femoral cortex
- Guide pin advanced to within 5 mm of subchondral bone in the center-center position of the femoral head (confirmed on both AP and lateral)
- Measure lag screw length
- Ream for lag screw; tap in good bone quality
- Insert lag screw - compress as per manufacturer instructions
For InterTAN (twin-screw design):
- Place derotation bar first inferior to guide pin
- Then place compression screw after lag screw
- Relax traction before final compression
Distal Locking
- Insert 1 or 2 distal screws for dynamic or static locking
- Short nails: distal interlocking is optional for standard oblique fractures
- Long nails: distal locking required
Tip-Apex Distance (TAD) - Critical Concept
TAD = distance (AP view) + distance (lateral view) from tip of lag screw to apex of femoral head
- TAD < 25 mm → associated with the lowest rate of screw cut-out
- TAD > 25 mm → significantly increased cut-out risk
- Note: TAD may not apply equally to helical blade designs - medial blade migration reported even with TAD <20 mm
- Helical blades have higher fixation failure (OR 1.88) vs standard lag screws
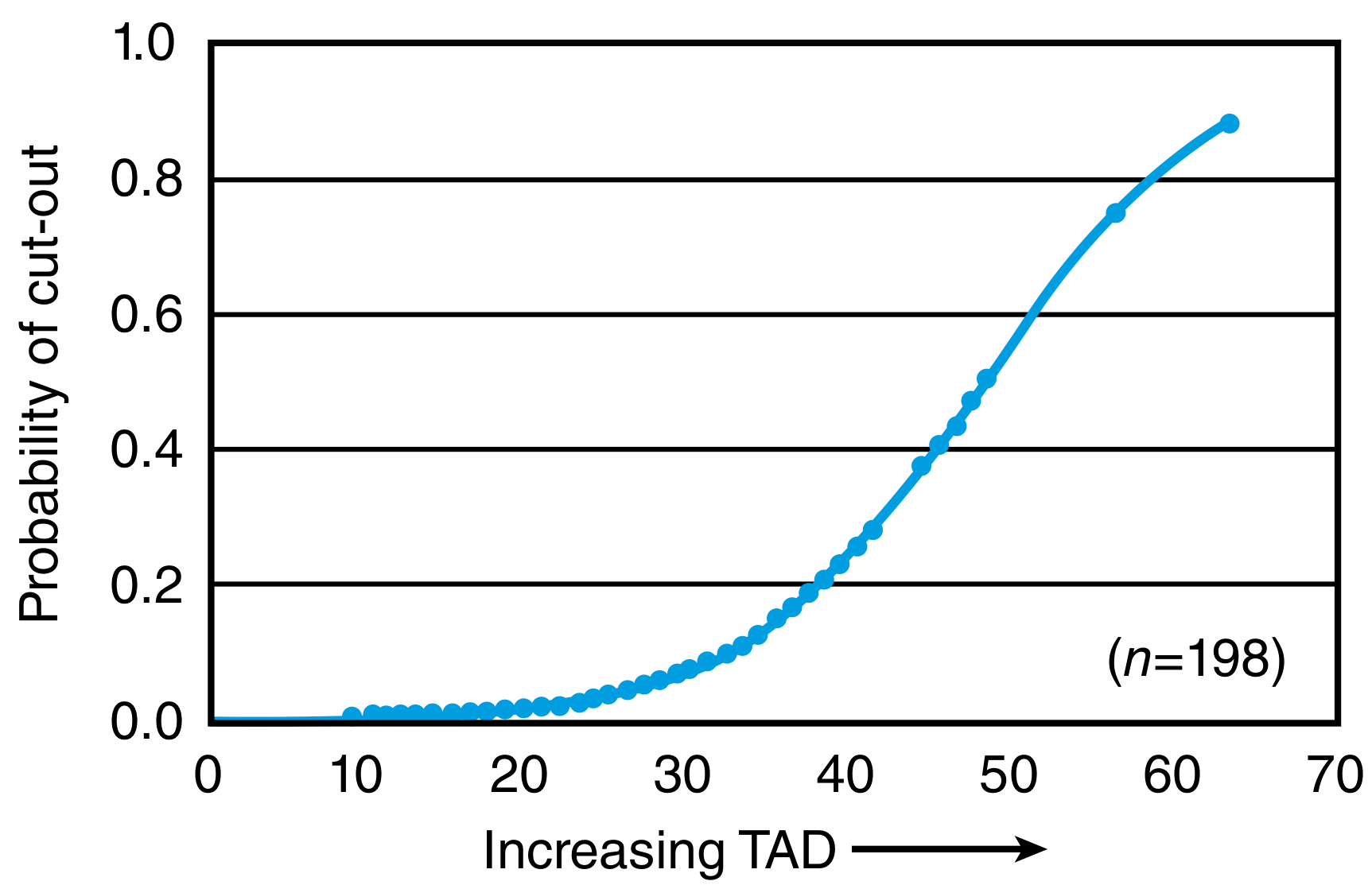
(Campbell's Operative Orthopaedics 15th Ed., p.3451)
Complications
| Complication | Details |
|---|---|
| Screw cut-out | Most common failure; prevented by TAD <25 mm, center-center placement |
| Anterior cortical perforation | Due to nail-femur bow mismatch; risk increased with posterior entry point; use long nail cautiously |
| Varus malreduction | Associated with nail CCD < native NSA; check contralateral hip |
| Excessive internal rotation | Common when GT not attached to distal fragment; careful fluoroscopic monitoring required |
| Lateral wall fracture | If lateral wall <20.5 mm, do not use SHS; use IM nail |
| Medial screw migration | More common with helical blade than with lag screw |
| Intraoperative fracture extension | Especially in narrow canals; ream adequately, do not hammer forcefully |
| Non-union | Uncommon; risk rises with malreduction |
| Limb shortening | Less with IM nail than with SHS device |
PFN vs. PFNA (Antirotation)
| Feature | PFN (classic) | PFNA |
|---|---|---|
| Proximal fixation | 2 screws (lag screw + hip pin) | Single helical blade |
| Rotational stability | Two-screw anti-rotation | Blade compacts cancellous bone |
| Osteoporotic bone | Moderate | Better (blade compaction) |
| Current use | Being replaced by PFNA | Preferred modern design |
The PFNA replaced the classic PFN; the blade achieves rotational and angular stability through a single element by compacting cancellous bone, which is especially advantageous in osteoporotic bone.
Short vs. Long Nail
| Short PFN | Long PFN | |
|---|---|---|
| Indications | Standard/stable IT fractures | Reverse oblique, subtrochanteric, pathological, shaft involvement |
| Distal locking | Optional | Required |
| Risk | Less anterior perforation risk | Higher perforation risk (bow mismatch) |
Key Pearls
- Reduce before you nail - nail does not reduce the fracture
- Nail with guide anteriorly first, rotate laterally after halfway insertion
- Use a 10 mm nail in most intertrochanteric fractures; larger diameter does not improve outcomes and may increase anterior perforation risk
- Always confirm center-center position on both AP and lateral before inserting lag screw
- Relax traction before final compression to allow fracture fragments to seat
- If nail does not advance easily → ream more; do not hammer aggressively (risk of fracture extension)
- Learning curve is significant; meticulous instrument use is essential as all steps are cannulated
(Sources: Campbell's Operative Orthopaedics 15th Ed. 2026, block31; Miller's Review of Orthopaedics 9th Ed., block6; AO Foundation PFNA guidelines)
Tell me about neck of femur fracture
Reading File
Finding Sources
Finding Sources
Searching the Web
neck of femur fracture classification Garden Pauwels management 2024
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have thorough coverage of NOF fractures. Let me compile a comprehensive, well-structured answer.
Neck of Femur (NOF) Fracture
A fracture of the femoral neck is one of the most common and serious injuries in orthopaedic surgery. It predominantly affects elderly osteoporotic patients after a low-energy fall, but in young patients it is usually the result of high-energy trauma. The 1-year mortality in elderly patients is approximately 30%.
Anatomy & Blood Supply
The blood supply to the femoral head is the key factor governing all major complications of NOF fractures. The medial femoral circumflex artery (MFCA) gives off the superior and inferior retinacular arteries that run along the femoral neck within the joint capsule. The superior retinacular artery is the dominant supply to the femoral head; the inferior retinacular artery also contributes significantly.
- Fractures that disrupt this retinacular supply (especially displaced fractures) risk avascular necrosis (AVN) of the femoral head
- The femoral neck is intracapsular - there is no periosteum, so healing depends on endosteal callus and is less robust
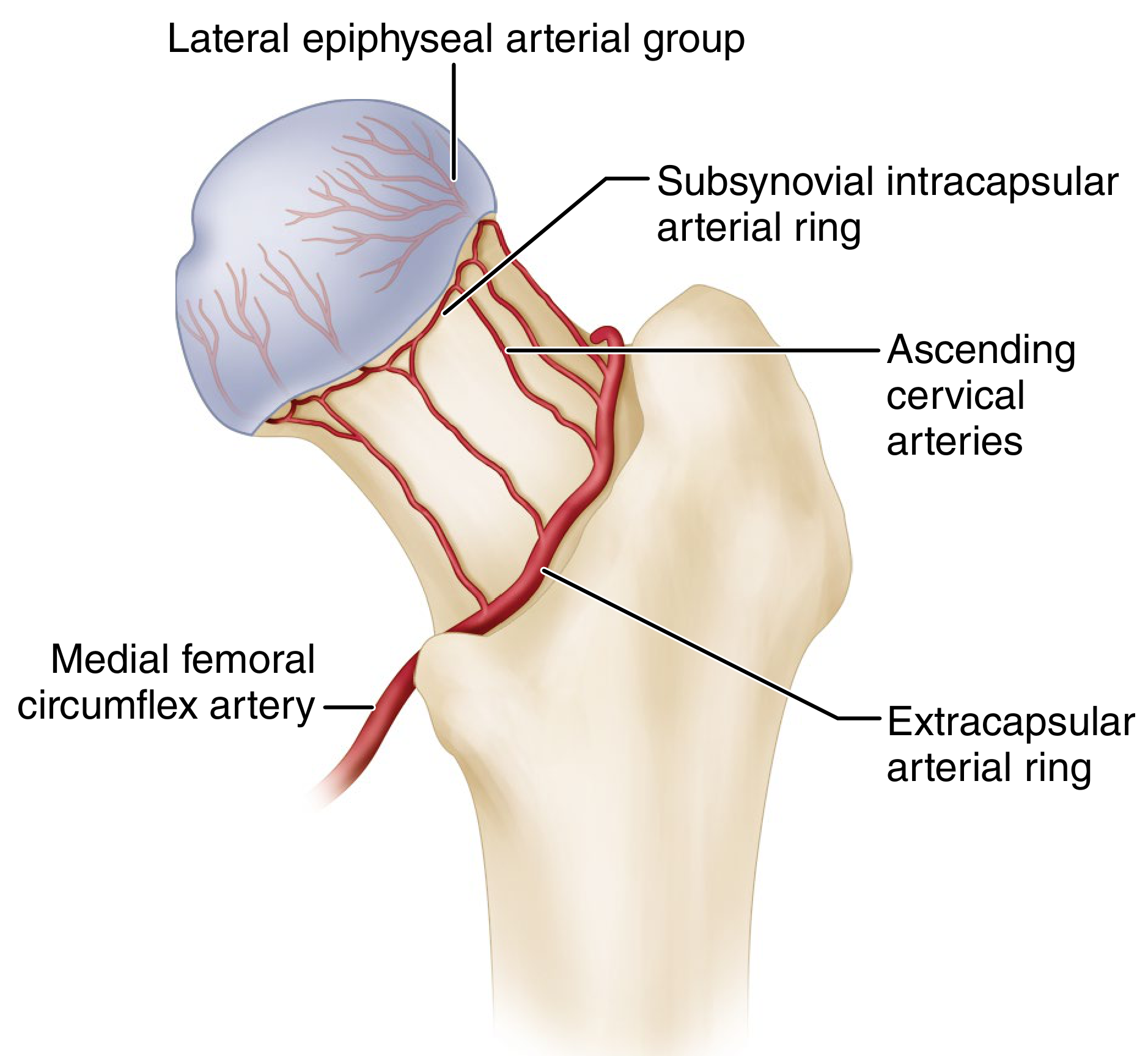
(Campbell's Operative Orthopaedics 15th Ed., p.3432)
Classification
1. By Location
| Type | Location |
|---|---|
| Subcapital | Just below the femoral head (most common) |
| Transcervical | Mid-neck |
| Basicervical | At the base of the neck (extracapsular; behaves more like intertrochanteric) |
2. Garden Classification (Most Widely Used)
Based on degree of displacement on AP radiograph:
| Grade | Description | Displaced? | Trabecular Pattern |
|---|---|---|---|
| I | Incomplete; valgus impacted | No | Trabeculae angulated (compressed) |
| II | Complete; nondisplaced | No | Trabeculae aligned |
| III | Complete; partial displacement | Yes | Trabeculae misaligned |
| IV | Complete; full displacement | Yes | Head rotates; trabeculae realign with acetabulum |
Key points:
- Garden I + II = nondisplaced (stable) → internal fixation
- Garden III + IV = displaced (unstable) → arthroplasty in elderly, ORIF in young
- Interobserver reliability is low across all 4 grades; most surgeons use the simplified displaced vs. nondisplaced dichotomy
- Garden III vs. IV differentiation: in III, neck and head still in contact but trabecular patterns are misaligned; in IV, complete loss of contact but head trabeculae re-align with acetabulum
- Limitation: Garden classification does not account for sagittal plane angulation. Garden I/II fractures with ≥20 degrees of sagittal angulation (retroversion) should not be managed as stable fractures
3. Pauwels Classification
Based on the angle of the fracture line relative to the horizontal - predicts shear forces at the fracture:
| Type | Angle | Biomechanics |
|---|---|---|
| I | 0-30° | Compressive forces dominate; most stable |
| II | 30-50° | Mixed compressive and shear |
| III | >50° | Shear forces dominate; most unstable, highest failure risk |
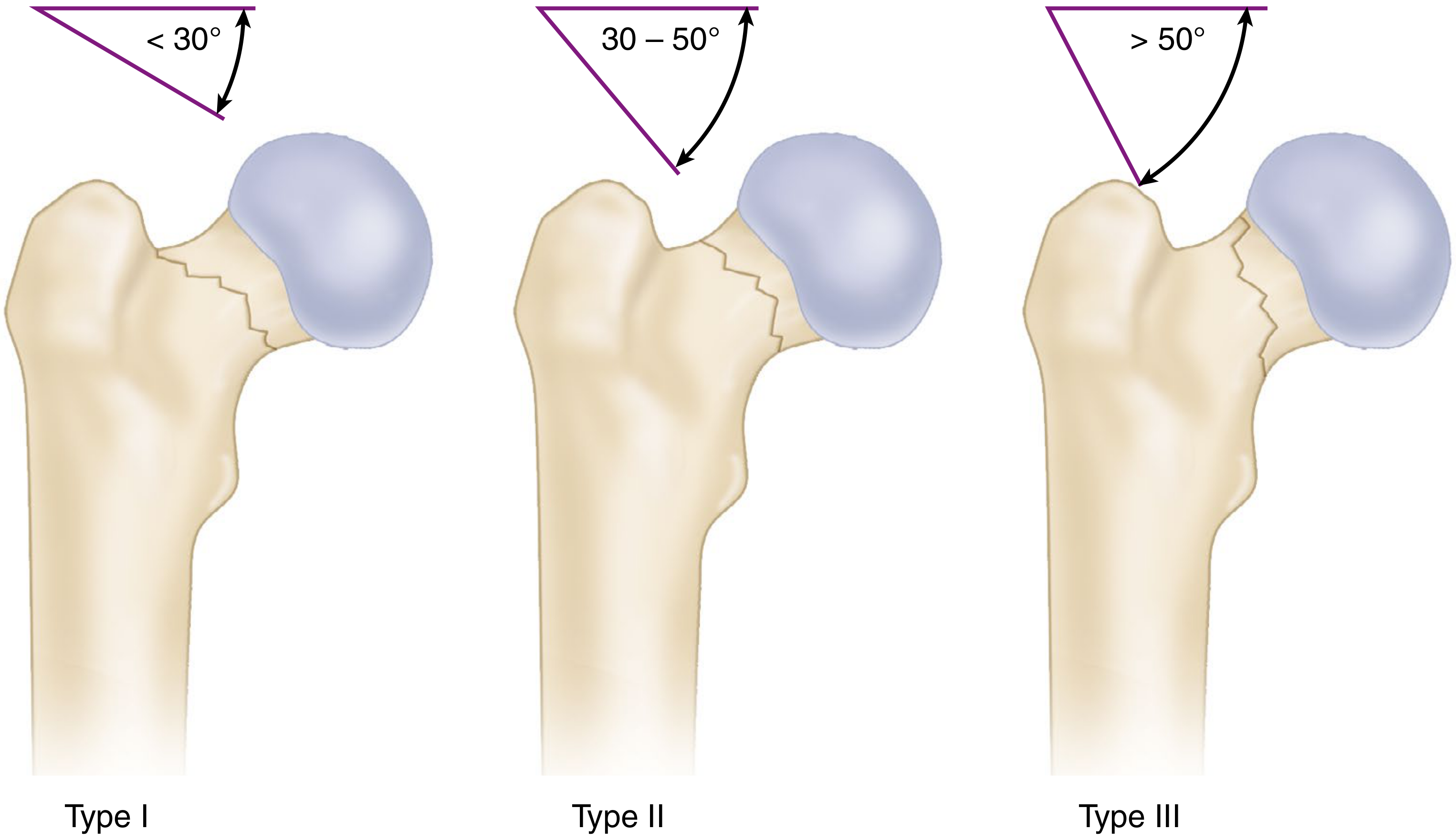
(Campbell's Operative Orthopaedics 15th Ed., p.3433)
Higher Pauwels angle → increased shear → requires stronger fixation (e.g., trochanteric lag screw, medial buttress plate)
Clinical Features
History:
- Elderly: trivial fall, often with pre-existing osteoporosis
- Young: high-energy RTA, fall from height
Symptoms and Signs:
- Pain in groin/hip, inability to weight bear
- Shortened, externally rotated limb (in displaced fractures)
- In impacted (Garden I) fractures, patient may still be able to partially weight-bear → diagnosis can be missed
Investigations:
- AP pelvis and lateral hip X-ray (first line)
- MRI - gold standard for occult fractures (CT may miss non-displaced fractures)
- CT - useful for assessing posterior comminution before surgery
Treatment Decision Framework
NOF Fracture
|
├── Nondisplaced (Garden I/II)
| └── Internal fixation (cannulated screws × 3)
| [young AND elderly - preserves femoral head]
|
└── Displaced (Garden III/IV)
|
├── Young patient (physiologically <60 yrs)
| └── URGENT ORIF (within 6-12 hrs)
| [preserve femoral head]
|
└── Elderly patient
|
├── Low functional demands / comorbid
| └── Hemiarthroplasty
|
└── Active, independent, good bone quality
└── THA (Total Hip Arthroplasty)
Operative Management
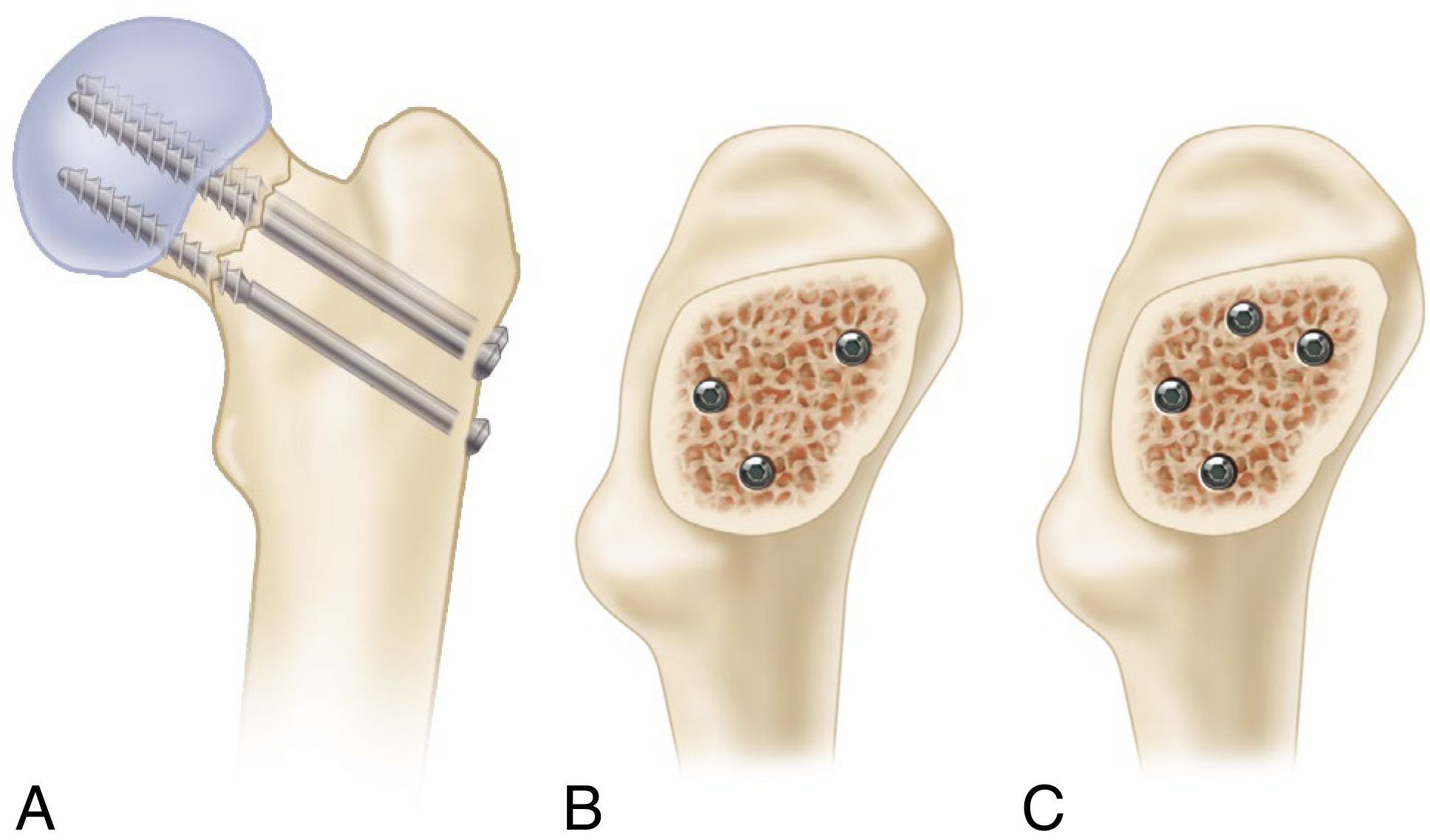
A. Cannulated Screw Fixation (Internal Fixation)
Indications: Garden I and II (nondisplaced); young patients with any displaced fracture (urgent)
Technique (Campbell's):
- Supine on fracture table; closed reduction using Whitman technique (traction, abduction, extension, then internal rotation)
- Assess reduction with fluoroscopy - use Garden alignment index:
- AP view: angle between medial femoral shaft and compressive trabeculae = 160-180 degrees (< 160° = varus; > 180° = excessive valgus)
- Lateral view: angulation ~180°; >20° deviation = unacceptable retroversion/anteversion
- Look for "S-shaped" or "reverse S-shaped" curves of femoral neck concavity meeting femoral head convexity - useful intraoperative alignment check
- Three partially threaded cancellous screws (6.5, 7.0, or 7.3 mm) in inverted triangle configuration
- One inferior screw along the calcar
- Two superior screws (anterosuperior and posterosuperior)
- Screws should abut cortical bone inferiorly and posteriorly to resist displacement
- Starting points must be above the lesser trochanter (distal starts → increased peri-implant subtrochanteric fracture risk)
- Guide pins advanced just short of articular surface; subtract 5 mm for screw length
- Fourth screw in diamond configuration may be used for significant posterior comminution - use extreme care (risk of extraosseous placement posteriorly)
Important: Varus malreduction strongly correlates with fixation failure - never accept varus!
(Campbell's Operative Orthopaedics 15th Ed., p.3435)
B. Femoral Neck System (FNS) and Fixed-Angle Devices
- The FNS (Synthes) is a newer fixed-angle implant showing decreased AVN rates, reduced shortening, and better functional outcomes vs. cannulated screws
- Biomechanically equivalent to dynamic hip screw; superior to multiple cannulated screws
- Proximal femoral locking plates reserved for fractures with significant posterior comminution
- Trochanteric lag screw + medial buttress plate for high Pauwels angle fractures (reduces shear)
C. Sliding Hip Screw (SHS/DHS)
- May be used for femoral neck fractures but carries a higher AVN risk than cannulated screws
- Better suited to basicervical fractures (which are more extracapsular in behaviour)
D. Hemiarthroplasty
Indications:
- Displaced fractures (Garden III/IV) in elderly with low functional demands
- Patients unable to comply with dislocation precautions (dementia, Parkinson's disease)
- Cemented femoral component is recommended for femoral neck fractures
- Unipolar and bipolar prostheses have similar functional results
E. Total Hip Arthroplasty (THA)
Indications:
- Displaced fractures in active, independent elderly patients - provides best functional outcomes
- Pre-existing hip arthritis (OA or RA) - THA preferred over hemiarthroplasty
- Higher dislocation rate than hemiarthroplasty - must counsel patients appropriately
Timing of Surgery
- Surgery within 48 hours reduces mortality
- Young patients with displaced fractures: treat as an orthopaedic emergency (within 6-12 hours if possible) - every hour of delay increases AVN risk
- Preoperative echocardiogram should NOT delay surgery in most cases
- Operate despite recent antiplatelet drug use
- Tranexamic acid (TXA) should be given to reduce blood loss and transfusion requirements
Complications
| Complication | Details |
|---|---|
| Avascular Necrosis (AVN) | Most feared complication; 15-35% after displaced fractures; occurs even in nondisplaced fractures (higher intracapsular pressure paradoxically in Garden I/II); capsulotomy may reduce risk especially in young/nondisplaced |
| Non-union | Higher with varus malreduction, poor fixation, high Pauwels angle |
| Fixation failure / implant cut-out | Up to 30% failure rate with internal fixation overall; higher in sagittal plane deformity (retroversion) |
| Dislocation | More common with THA than hemiarthroplasty |
| Peri-implant fracture | Screw starting points too distal (below lesser trochanter) |
| Leg length discrepancy / shortening | Especially with collapse |
| Infection | Can require staged revision; suppress with antibiotics until union then implant removal |
| 1-year mortality | ~30% in elderly patients |
Osteonecrosis and Non-union
- Osteonecrosis is an ongoing problem even after nondisplaced fractures
- In young patients with nondisplaced fractures, capsulotomy is considered (routine capsulotomy is controversial; most effective when capsule is not torn and intracapsular tamponade may be contributing)
- Valgus intertrochanteric osteotomy is an option for femoral neck non-union/malunion in young patients
- In elderly: non-union and AVN are treated with THA
Special Considerations
Basicervical fractures:
- Located at the base of the neck; partly intracapsular, partly extracapsular
- Behave biomechanically more like intertrochanteric fractures
- Higher failure rate with cephalomedullary nailing (screw cut-out even with TAD <22 mm reported)
- Management debated; options include SHS, IM nail with derotational screw, or arthroplasty in the elderly
Young patients:
- Typically high-energy mechanisms
- Associated injuries common
- Every effort made to preserve the femoral head: urgent ORIF within 6-12 hours
- Failure of fixation → revision ORIF or valgus osteotomy (not immediately to arthroplasty)
Pathological fractures:
- Consider underlying malignancy, Paget's disease, metabolic bone disease
- Long PFN with cephalomedullary fixation for metastatic disease; arthroplasty for lytic lesions in femoral head/neck
(Sources: Campbell's Operative Orthopaedics 15th Ed. 2026; Miller's Review of Orthopaedics 9th Ed.; Rockwood & Green's Fractures in Adults 10th Ed. 2025)
This is a shared conversation. Sign in to Orris to start your own chat.