What's the development of midget embryology
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information to provide a thorough answer about midget cell embryology/development in the retinal visual system. Let me compile the full response.
Midget Cells: Development and Embryology
"Midget" in anatomical and neuroscience contexts refers to a specific class of retinal ganglion cells (RGCs) - the midget cells (also called Pβ or B cells, or P-type ganglion cells). They are the most numerous RGC type in the primate retina (~70% of all RGCs) and form the foundation of the parvocellular (P) visual pathway. Here is a complete account of their development and circuit organization.
1. Origin and Cellular Identity
Midget cells are a subtype of retinal ganglion cell. Like all retinal neurons, they originate from multipotent retinal progenitor cells (RPCs) in the developing neuroepithelium of the optic cup, which itself derives from the diencephalon (forebrain).
- The retina is embryologically a direct outgrowth of the central nervous system - the optic vesicle evaginates from the forebrain at around week 4 of human gestation, then invaginates to form the bilayered optic cup
- The inner layer of the optic cup becomes the neural retina, while the outer layer becomes the retinal pigment epithelium (RPE)
- Retinal ganglion cells are among the first neurons to differentiate in the neural retina - this is a conserved rule of retinal histogenesis ("early-born" neurons)
2. Retinal Histogenesis and the "Birth Order" of Neurons
Retinal neurons are generated in a conserved sequence:
| Neuron Type | Approximate Birth Order |
|---|---|
| Retinal ganglion cells (including midget precursors) | First |
| Horizontal cells | Early |
| Cone photoreceptors | Early |
| Amacrine cells | Mid |
| Rod photoreceptors | Late |
| Bipolar cells (including midget bipolar) | Late |
| Müller glia | Last |
Midget RGCs and their dedicated midget bipolar cells are the two principal components of the midget circuit. Because bipolar cells are born later, the midget circuitry is assembled in a temporally staggered fashion - the ganglion cell scaffold is laid down first, and then the bipolar cell connects to it.
3. The Midget Circuit - Structural Organization
The defining anatomical feature of the midget system is its one-to-one (private line) connectivity in the central retina (fovea and parafovea):
- A single midget bipolar cell receives input from one cone photoreceptor only
- That midget bipolar cell excites one midget ganglion cell
- This strict 1:1:1 connectivity (cone → midget bipolar → midget RGC) underlies the extremely high spatial resolution of the central visual field
As Kandel's Principles of Neural Science states:
"In the central region of the primate retina, the midget bipolar cell receives input from a single cone and excites a P-type ganglion cell. This explains why the centers of P-cell receptive fields are so small." - Principles of Neural Science, 6th Ed.
This private-line architecture is a primate-specific specialization. In more peripheral retina, the convergence ratio increases (multiple cones to one midget RGC).
4. Morphological Properties
Compared to the other major class - parasol cells (M-type, magnocellular pathway):
| Feature | Midget Cells (P-type) | Parasol Cells (M-type) |
|---|---|---|
| Also known as | Pβ / B cells | Pα / A cells |
| Cell body size | Small | Large |
| Dendritic field | Small | Large |
| Axon diameter | Smaller | Larger |
| Receptive field | Small (fine detail) | Large (gross features/motion) |
| Proportion of RGCs | ~70% | ~10% |
| Spectral tuning | Color opponent (red-green) | Achromatic contrast |
- Neuroanatomy through Clinical Cases, 3rd Ed.
- Bradley and Daroff's Neurology in Clinical Practice
5. Receptive Field Development
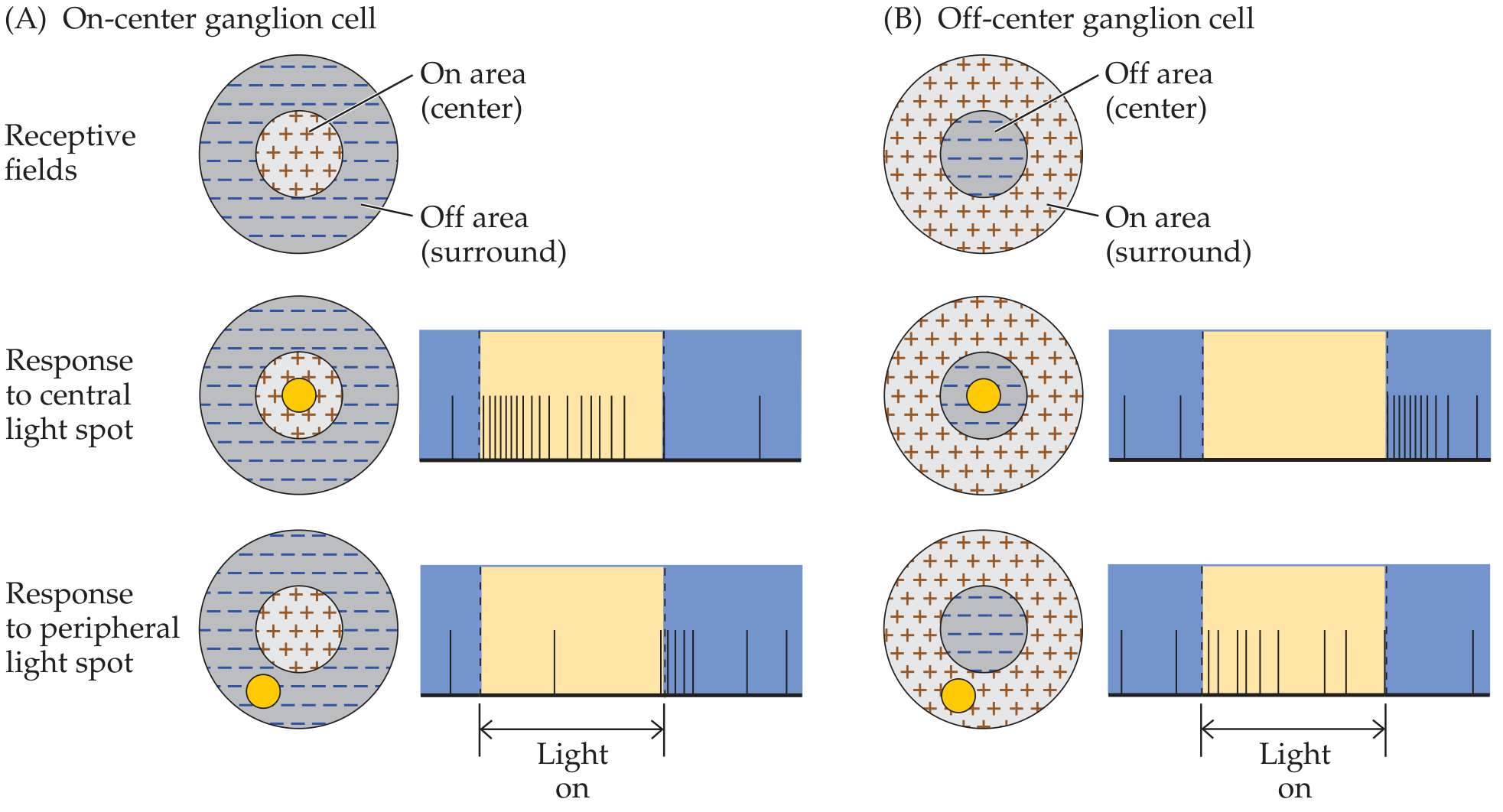
Midget cells develop center-surround receptive fields, which arise from lateral inhibitory circuits involving horizontal cells and amacrine cells:
- Horizontal cells in the outer plexiform layer mediate surround inhibition at the photoreceptor-bipolar synapse
- Amacrine cells in the inner plexiform layer further sharpen the surround in the inner retina
- ON-center midget cells are excited by light in the center of their receptive field and inhibited by the surround; OFF-center midget cells respond in the opposite manner
- Both ON and OFF midget cell subtypes exist
The center-surround architecture is shared across species but the exquisitely small center (a single cone's input) is unique to the primate midget system and only fully develops as the fovea matures postnatally.
6. Projection: Parvocellular Pathway
Midget RGC axons travel in the optic nerve, partially decussate at the optic chiasm (nasal fibers cross; temporal fibers stay ipsilateral), and then project via the optic tract to layers 3-6 of the lateral geniculate nucleus (LGN) - the parvocellular layers:
- The LGN has 6 layers total: layers 1-2 are magnocellular (M/parasol input), layers 3-6 are parvocellular (P/midget input), with thin koniocellular intercalated layers between
- The parvocellular layers receive exclusively midget RGC input and carry red-green color opponency and fine spatial detail
- After the LGN, midget pathway information projects to V1 (primary visual cortex), then to V2 and V4 (color processing in the fusiform gyrus - the ventral "what" stream)
"Parvocellular layers get input from the midget retinal ganglion cells, which are the most numerous in the primate retina (~70%) and carry red-green opponent information." - Principles of Neural Science, 6th Ed.
7. Functional Role
The midget/parvocellular system is specialized for:
- High spatial acuity (fine detail perception)
- Color vision (red-green opponent signals from L and M cones)
- Sustained (tonic) responses to maintained stimuli
- Object recognition (feeds the ventral "what" stream to V4 and inferotemporal cortex)
Summary
The midget cell system develops from the neural retina (diencephalic origin), with ganglion cells being among the earliest neurons born. The hallmark midget circuit (1 cone → 1 midget bipolar → 1 midget RGC) is established as retinal progenitors differentiate in sequence, and the center-surround receptive fields are sculpted by lateral inhibitory interneurons (horizontal and amacrine cells). Midget axons project to the parvocellular LGN layers and ultimately drive the cortical pathways for color discrimination and fine spatial detail.
Sources:
- Neuroanatomy through Clinical Cases, 3rd Ed. (Blumenfeld)
- Principles of Neural Science, 6th Ed. (Kandel et al.)
- Bradley and Daroff's Neurology in Clinical Practice
Midgut sey
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
I now have everything needed for a comprehensive answer. Here is the full response on midgut embryology:
Midgut Embryology
1. What is the Midgut?
The primitive gut tube is suspended from the posterior abdominal wall and is divided into three segments - foregut, midgut, and hindgut - each with its own arterial supply:
| Segment | Artery | Adult Derivatives |
|---|---|---|
| Foregut | Celiac artery | Esophagus to 2nd part of duodenum (proximal to ampulla) |
| Midgut | Superior mesenteric artery (SMA) | Distal duodenum to proximal 2/3 of transverse colon |
| Hindgut | Inferior mesenteric artery | Distal 1/3 transverse colon to upper anal canal |
The midgut specifically gives rise to:
- Duodenum distal to the ampulla of Vater
- Entire small intestine (jejunum and ileum)
- Cecum, appendix, ascending colon, and proximal 2/3 of transverse colon
2. Early Midgut Development (Week 3-5)
- By week 3, the embryonic intestine begins segmental development; the septum transversum demarcates foregut from midgut
- By week 5, the midgut is suspended from the dorsal abdominal wall by a short mesentery and communicates with the yolk sac via the vitelline (omphalomesenteric) duct
- Rapid elongation begins, forming the primary intestinal loop, with the vitelline duct at its apex
- The loop has two limbs:
- Cephalic (proximal) limb - gives rise to distal duodenum, jejunum, and proximal ileum
- Caudal (distal) limb - gives rise to distal ileum, cecum, appendix, ascending colon, and proximal 2/3 of transverse colon
3. The Four Key Developmental Stages
The midgut undergoes four predictable, sequential processes:
(a) Elongation
- Rapid lengthening of the gut loop outpaces growth of the abdominal cavity
- The liver also grows rapidly at this time, occupying much of the available intraabdominal space
- This combination makes it physically impossible for the gut to remain in the abdomen
(b) Physiological Umbilical Herniation (Weeks 6-10)
- Week 6: The primary intestinal loop protrudes into the umbilical cord (physiological umbilical herniation) - this is a normal developmental event, not a pathological hernia
- Week 7: The small intestine begins to rotate counterclockwise around the axis of the SMA
- Week 9: Continued intestinal growth causes further herniation; the gut rotates an initial 90 degrees counterclockwise while outside the abdomen
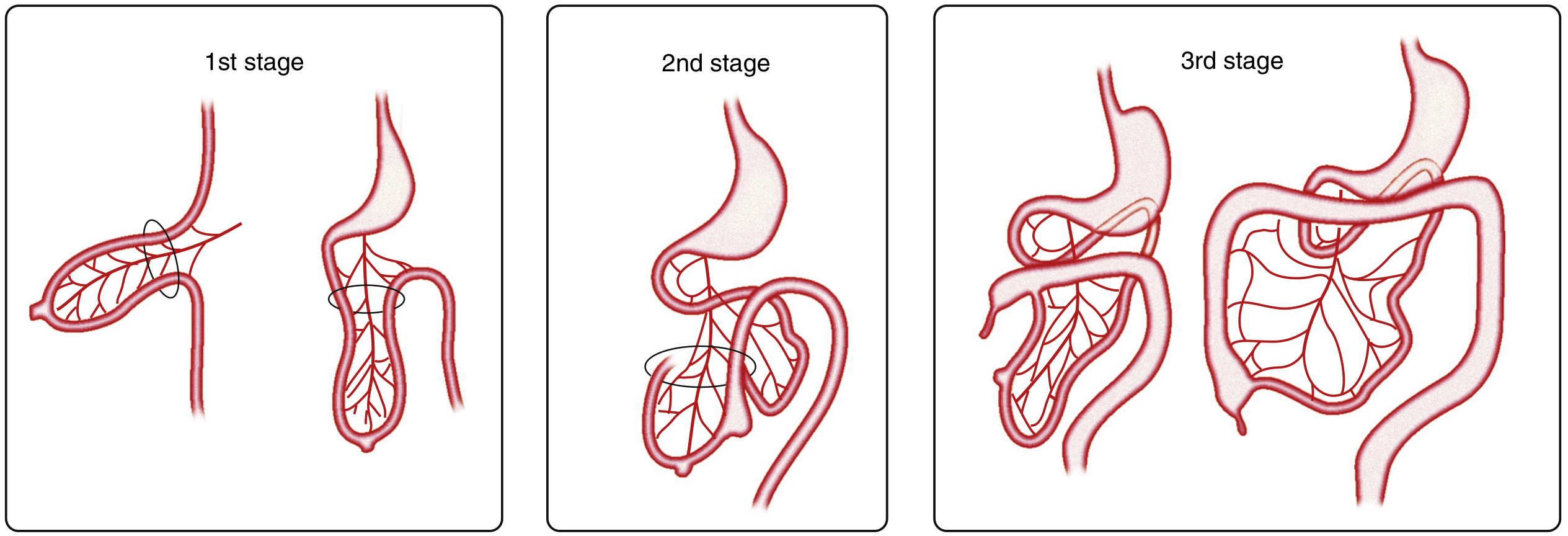
(c) 270° Counterclockwise Rotation
- Week 10-11: The intestines return to the abdominal cavity, rotating a further 180 degrees counterclockwise, for a total of 270 degrees of counterclockwise rotation around the SMA axis
- The jejunum returns first, filling the left half of the abdominal cavity (left upper quadrant)
- The ileum returns next, filling the right half
- The colon enters last: the cecum initially lies in the right upper quadrant (RUQ), then descends to the right iliac fossa, placing the ascending colon and hepatic flexure in the right abdomen
The diagram below shows the 3 stages of normal intestinal rotation:
(d) Fixation
- After the ascending and descending colon reach their final positions, their mesenteries fuse with the posterior peritoneum - they become retroperitoneal
- The ascending and descending mesocolon fuses with the parietal peritoneum (Toldt's fascia develops)
- The transverse mesocolon fuses with the posterior wall of the greater omentum
- The mesentery of the jejunum and ileum remains free, running from the duodenojejunal flexure (ligament of Treitz) to the ileocecal junction
4. Lumen Formation: Canalization
- By weeks 7-10, the gut lumen is temporarily obliterated by rapid endodermal cell proliferation
- This is followed by recanalization - vacuoles form within the epithelial mass and coalesce to restore the lumen
- Failure of recanalization (particularly in the duodenum) leads to intestinal atresia or stenosis
- Villus formation begins at week 8, progressing proximal to distal
- Crypts appear by week 12; intestinal enzymes reach adult activity levels by week 14
5. Cecum and Appendix Development
- The cecum appears as a small dilatation (bud) of the caudal limb of the primary intestinal loop at ~week 6
- After returning to the abdomen, it first lies in the RUQ, then descends to the right iliac fossa
- The appendix develops from the distal end of the cecal bud during colonic descent; because it develops during descent, its final position is frequently retrocecal or retrocolonic
6. Mesenteric Development
- As the caudal limb of the intestine moves to the right, the dorsal mesentery twists around the SMA origin
- After the ascending and descending colon become retroperitoneal, their mesenteries fuse with the posterior wall
- The jejunal-ileal mesentery retains its free attachment, extending from the duodenum to the ileocecal junction (a broad-based, fan-shaped structure)
7. Congenital Anomalies from Abnormal Midgut Development
| Anomaly | Embryological Defect |
|---|---|
| Malrotation | Failure of complete 270° rotation; proximal midgut fails to rotate while distal midgut rotates only 90° clockwise |
| Midgut volvulus | Consequence of malrotation - entire midgut hangs on a single narrow SMA pedicle and can twist, causing ischemia/infarction |
| Omphalocele | Failure of the midgut to return to the abdominal cavity at week 10-11; gut remains herniated into the umbilical cord, covered by peritoneum |
| Gastroschisis | Full-thickness abdominal wall defect (not related to umbilical ring) through which bowel herniates without a membrane covering |
| Meckel's diverticulum | Persistence of the vitelline duct; located in the ileum ~2 feet from the ileocecal valve; the "rule of 2s" |
| Intestinal atresia | Type I: failed recanalization (intraluminal web); Types II/IIIa/IIIb/IV: fetal mesenteric vascular accidents |
| Nonrotation | Gut enters abdomen but does not rotate; small bowel lies on right, colon on left |
"Everyone in health care is taught that bilious emesis in a newborn is malrotation and midgut volvulus until proven otherwise." - Fischer's Mastery of Surgery, 8th Ed.
Infants with omphalocele almost invariably have associated malrotation because if the gut never returned to the abdomen, rotation could not have completed. - Miller's Anesthesia, 10th Ed.
Summary Timeline
| Week | Event |
|---|---|
| Week 3 | Primitive gut tube forms; septum transversum separates foregut/midgut |
| Week 5 | Midgut communicates with yolk sac via vitelline duct; primary intestinal loop forms |
| Week 6 | Physiological herniation into umbilical cord begins; cecal bud appears |
| Week 7-8 | Small intestine rotates 90° CCW outside abdomen; lumen temporarily obliterated; villi appear |
| Week 9-10 | Further herniation; gut continues rotating |
| Week 10-11 | Gut returns to abdomen, completing total 270° CCW rotation; cecum descends to RIF |
| Week 12-14 | Crypts form; mesenteric fixation; intestinal enzymes reach adult levels |
Sources:
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease
- Yamada's Textbook of Gastroenterology, 7th Ed.
- Miller's Anesthesia, 10th Ed.
- Mulholland and Greenfield's Surgery, 7th Ed.
- Schwartz's Principles of Surgery, 11th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.