amniotic fluid and its disorders in obs
Reading File
Finding Sources
Finding Sources
Searching PubMed
"amniotic fluid" AND "disorders" AND obstetrics
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
I now have comprehensive data from Creasy & Resnik's Maternal-Fetal Medicine. Let me compile a thorough, well-structured answer.
Amniotic Fluid and Its Disorders in Obstetrics
Source: Creasy & Resnik's Maternal-Fetal Medicine: Principles and Practice
1. What Is Amniotic Fluid?
Amniotic fluid (AF) is essential for normal fetal growth and development. Its key roles include:
- Cushioning - protects the fetus from mechanical trauma
- Bacteriostatic properties - helps maintain a sterile intrauterine environment
- Space for movement - allows fetal mobility and supports normal development of lungs and limbs
- Diagnostic access - provides fetal cells and metabolic byproducts; used in amniocentesis (first performed in 1956 for sex determination)
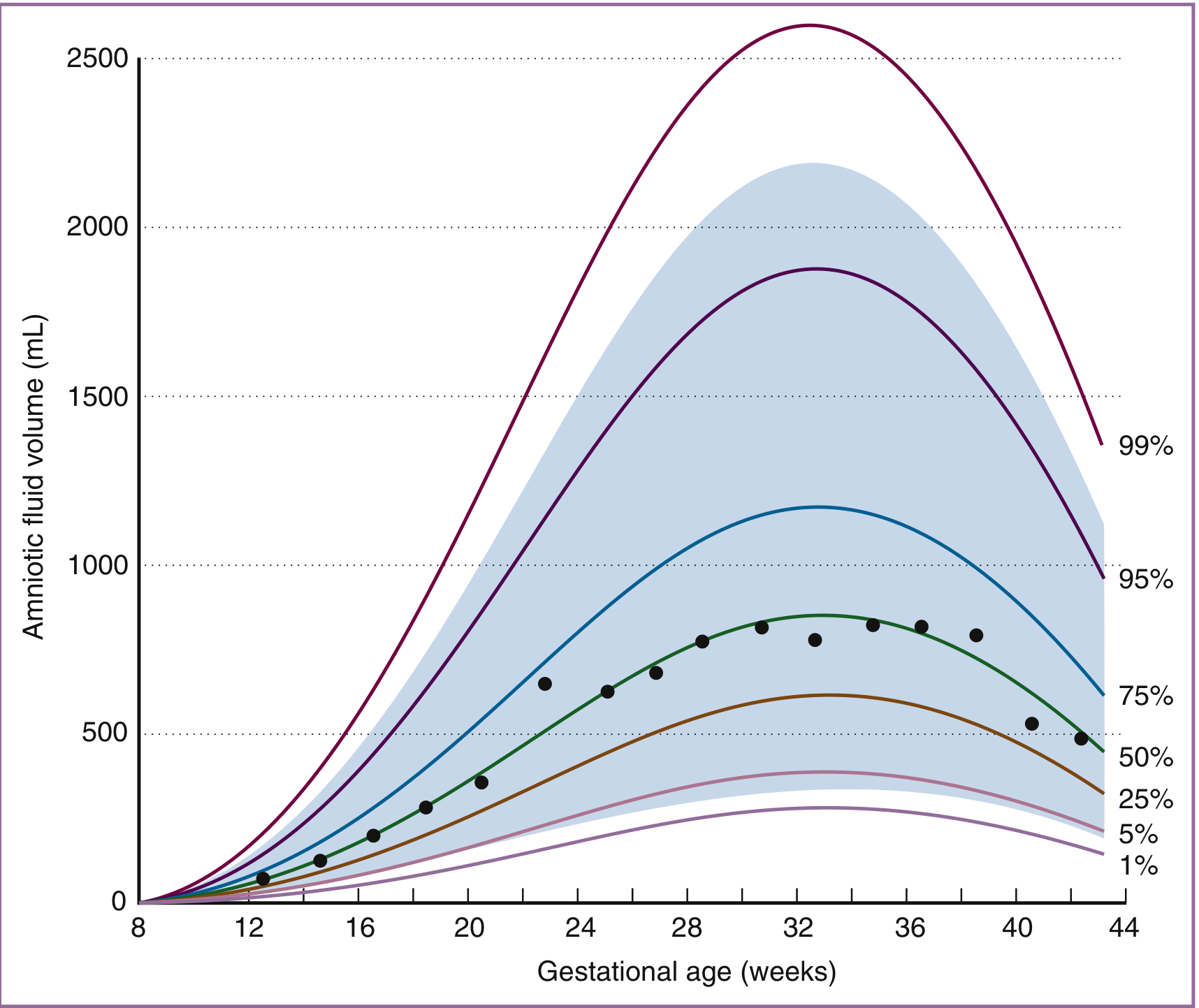
2. Volume of Amniotic Fluid
AF volume changes predictably throughout pregnancy:
| Gestational Age | AF Volume |
|---|---|
| 8 weeks | < 10 mL |
| 22 weeks | ~630 mL |
| 28 weeks | ~770 mL |
| 34-36 weeks | Maximum (~800 mL) |
| 41 weeks | ~515 mL |
| Post-term | Falls ~33% per week |
Key dynamics:
- Volume increases at 10 mL/week early in fetal period, peaks at 50-60 mL/week at 19-25 weeks
- After 34 weeks, volume falls at 60-70 mL/week at 40 weeks
- The late-pregnancy decline is a physiologic progression, not an aberration
3. Composition of Amniotic Fluid
First trimester:
- Isotonic with maternal/fetal plasma
- Minimal protein
- Very low oxygen tension
- High concentration of sugar alcohols (product of anaerobic metabolism)
- Arises as a transudate of plasma - through nonkeratinized fetal skin or across uterine decidua/placenta
Second half of pregnancy (mid-trimester onward):
- Fetal urine becomes the major component (fetus produces dilute urine)
- AF osmolality falls to ~85-90% of maternal serum osmolality (drops by 20-30 mOsm/kg with advancing gestation)
- AF urea, creatinine, and uric acid increase to 2-3x fetal plasma levels
- The entire volume of AF turns over on a daily basis - a highly dynamic system
4. Production and Resorption - Sources and Sinks
| Source/Sink | Role |
|---|---|
| Fetal urine | Major source in second half of pregnancy |
| Fetal lung fluid | Secreted into AF |
| Fetal swallowing | Major route of resorption (~500-1000 mL/day near term) |
| Intramembranous (IM) flow | Water crosses amnion into fetal vasculature |
| Transmembranous flow | Across uterine wall to maternal circulation |
The amnion is a "leaky" epithelium with significant water flux potential, comparable to renal tubular epithelium. IM flow can be modulated to maintain AF volume homeostasis - for example, when fetal swallowing is experimentally blocked, IM flow increases to normalize volume.
5. Ultrasound Assessment of AF Volume
Two main methods are used clinically:
- Maximum Vertical Pocket (MVP) - single deepest pocket
- Amniotic Fluid Index (AFI) - sum of MVP in four uterine quadrants
Both can be used; subjective assessment is also acceptable. Per ISUOG guidelines, AFI and MVP are used to classify volume as normal, reduced, or excessive.
6. Disorders of Amniotic Fluid
A. Polyhydramnios (Hydramnios) - Excess AF
Definition: AFI > 24-25 cm or MVP > 8 cm
Classification by AFI:
| Grade | AFI |
|---|---|
| Mild | 25-30 cm |
| Moderate | 30.1-35 cm |
| Severe | > 35.1 cm |
Causes:
- Impaired fetal swallowing - neurologic abnormalities, obstructions
- GI anomalies - esophageal atresia, tracheoesophageal fistula
- Respiratory anomalies - congenital diaphragmatic hernia
- Maternal diabetes mellitus - fetal hyperglycemia leads to osmotic diuresis
- Fetal anemia - increased cardiac output and urine flow
- Twin-to-twin transfusion syndrome (TTTS) - recipient twin
- Idiopathic - no identifiable cause in many cases
- Hypoproteinemia with decreased maternal plasma oncotic pressure
Consequences / Complications:
- Preterm birth (PTB): 18.5% with mild, 21.8% with moderate, 14.3% with severe polyhydramnios
- Uterine overdistension triggers inflammatory cytokines (IL-1β, TNF-α, IL-6, IL-8, CCL2, PGE2, PGF2α) - causing preterm labor
- The underlying cause (congenital malformations, diabetes) determines PTB risk more than the fluid volume itself
- Maternal discomfort, dyspnea
- Malpresentation
- Cord prolapse
- Placental abruption (after rapid decompression)
B. Oligohydramnios - Reduced AF
Definition: AFI < 5 cm or MVP < 2 cm
Causes:
- Renal agenesis / bilateral renal anomalies - no urine production (Potter sequence)
- Posterior urethral valves / lower urinary tract obstruction - leads to oligohydramnios, pulmonary hypoplasia, renal dysplasia, Potter facies, clubfeet
- Placental insufficiency / uteroplacental insufficiency - reduced fetal perfusion reduces urine output
- Post-term pregnancy - AF falls 33%/week after 41 weeks (physiologic)
- Rupture of membranes (PPROM/PROM) - loss of AF
- Maternal dehydration - osmotic mechanism; rehydration can reverse it
Consequences:
- Pulmonary hypoplasia - AF is required for normal lung development; severe oligohydramnios early in pregnancy is particularly dangerous
- Limb deformities - restricted fetal movement
- Potter sequence - renal agenesis → oligohydramnios → pulmonary hypoplasia, Potter facies (flat nose, low-set ears, epicanthal folds), limb contractures
- Fetal distress - cord compression, fetal hypoxia
- Perinatal mortality - higher with severe oligohydramnios
- Intrauterine growth restriction (IUGR) association
C. Amniotic Fluid Embolism (AFE)
AFE is a rare but potentially fatal obstetric emergency:
Nature: A "spectrum disorder" - not precisely an embolism nor strictly amniotic fluid-related. It reflects a breach in the normal physiologic barrier between mother and fetus, with an abnormal maternal response to fetal tissue exposure - similar to systemic inflammatory response syndrome (SIRS) and anaphylaxis.
Diagnostic Triad (SMFM/AFE Foundation criteria):
- Hemodynamic compromise (cardiovascular collapse)
- Respiratory compromise
- Disseminated intravascular coagulopathy (DIC)
Clinical features:
- Sudden cardiovascular collapse and cardiac arrest
- Severe hypoxia
- DIC with hemorrhage
- Often occurs during labor, delivery, or within 30 minutes postpartum
Management (supportive - no specific treatment):
- Early intubation + 100% O2 + PEEP
- High-quality CPR immediately for cardiac arrest
- If AFE occurs before delivery → emergent cesarean delivery to improve maternal resuscitation and fetal survival
- Large-bore IV access + arterial line
- Transesophageal echocardiography after intubation - to manage pulmonary hypertension and cardiac failure
- Pressors, inotropes, pulmonary vasodilators as needed
- ECMO - consider after prolonged arrest or severe ventricular dysfunction unresponsive to medical management
- Massive transfusion: Packed RBCs : FFP : Platelets in 1:1:1 ratio
- TEG / ROTEM point-of-care testing for coagulopathy guidance
- Note: Recombinant activated Factor VIIa is controversial - a systematic review found it may worsen outcomes in AFE
Cannot be predicted or prevented.
7. Summary Table
| Feature | Polyhydramnios | Oligohydramnios |
|---|---|---|
| Definition | AFI > 24-25 cm / MVP > 8 cm | AFI < 5 cm / MVP < 2 cm |
| Key causes | GI obstruction, diabetes, fetal anemia, TTTS, idiopathic | Renal agenesis, LUTO, placental insufficiency, PROM, post-term |
| Complications | PTB, malpresentation, cord prolapse, abruption | Pulmonary hypoplasia, limb deformities, Potter sequence, IUGR |
| Mechanism of PTB | Uterine overdistension → inflammatory cytokines | - |
| Key diagnostic tool | Ultrasound (AFI/MVP) | Ultrasound (AFI/MVP) |
References: Creasy & Resnik's Maternal-Fetal Medicine: Principles and Practice - Chapter 4 (Amniotic Fluid Dynamics, Ross & Beall) and Chapter 18 (Amniotic Fluid Embolism, p. 6137-6146).
This is a shared conversation. Sign in to Orris to start your own chat.