Teach me ECG very properly and clearly with picture example
Reading File
Finding Sources
Finding Sources
Searching Images
ECG electrocardiogram normal waves P QRS T labeled diagram
Finding Sources
Searching Images
ECG grid paper small squares large squares time voltage measurement
Searching Images
12 lead ECG placement chest limb leads electrode position
Reading File
Reading File
Searching Images
ECG atrial fibrillation ventricular tachycardia heart block arrhythmia comparison
Loading Image
Reading File
Searching Images
ST elevation myocardial infarction STEMI ECG changes acute MI
Loading Image
Loading Image
Loading Image
Searching Images
ECG axis deviation left right hexaxial system lead I aVF quadrant
Loading Image
Loading Image
Searching Images
bundle branch block left right LBBB RBBB QRS morphology ECG
I now have all the images and content needed. Let me compile the comprehensive ECG guide:
📈 A Complete Guide to ECG Interpretation
Based on Costanzo Physiology, Braunwald's Heart Disease, Harrison's Principles of Internal Medicine, and peer-reviewed sources.
1. What Is an ECG?
An electrocardiogram (ECG or EKG) records tiny electrical potential differences on the body surface that reflect the sequence of depolarization and repolarization of the heart muscle. Because the heart does not depolarize all at once — atria before ventricles, in a specific spatial sequence — measurable voltage differences arise between body surface points. Electrodes placed on the skin capture these voltages over time and plot them as a waveform on grid paper.
2. The ECG Grid
Standard ECG paper runs at 25 mm/second with a calibration of 10 mm = 1 mV (amplitude).
| Division | Size | Time | Voltage |
|---|---|---|---|
| Small square | 1 mm | 0.04 s | 0.1 mV |
| Large square | 5 mm (5 small) | 0.20 s | 0.5 mV |
Quick rule: 5 large squares = 1 second. Heart rate = 300 ÷ number of large squares between R waves (for regular rhythms).
3. The 12 Leads — Where the Electrodes Go
A 12-lead ECG gives 12 different "views" of the same cardiac electrical activity. You place 10 physical electrodes; the machine calculates 12 leads mathematically.
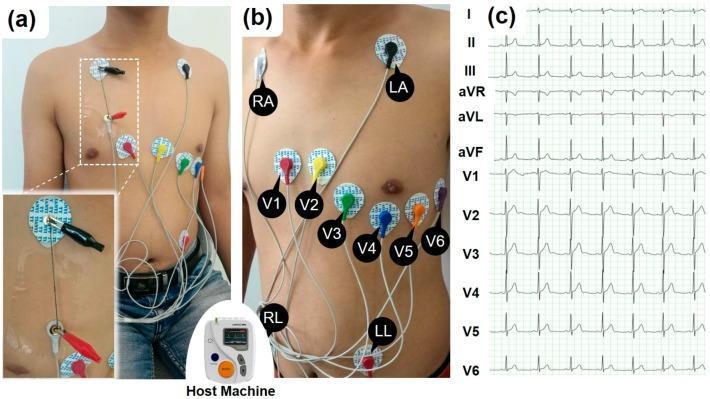
Limb Leads (Frontal Plane)
| Lead | What it "sees" |
|---|---|
| I | Left side of heart (lateral) |
| II | Inferior surface |
| III | Inferior surface |
| aVR | Right shoulder — looks "into" the heart cavity |
| aVL | Left shoulder — lateral |
| aVF | Left foot — inferior |
Precordial (Chest) Leads — V1 to V6
Placed across the chest from right to left; they view the heart in the horizontal plane:
- V1–V2: Right ventricle / septal
- V3–V4: Anterior (septum + anterior wall)
- V5–V6: Lateral left ventricle
4. The Normal ECG Waveform — P, QRS, T
This is the most fundamental diagram in ECG interpretation:

Each Component Explained
🔵 P Wave — Atrial Depolarization
- Represents depolarization of the atria (SA node fires → atria contract)
- Normal duration: < 0.12 s (3 small squares)
- Normal amplitude: < 2.5 mm
- Upright in leads I, II, aVF; inverted in aVR
- Absent P wave → think atrial fibrillation or junctional rhythm
🔵 PR Interval — AV Node Conduction
- Measured from start of P to start of QRS
- Represents time from atrial depolarization → start of ventricular depolarization — includes conduction through the AV node
- Normal: 0.12–0.20 s (3–5 small squares)
- Prolonged PR (>0.20 s) = 1st-degree AV block
- Short PR (<0.12 s) = pre-excitation (e.g., WPW syndrome)
🔵 QRS Complex — Ventricular Depolarization
- Three waves collectively representing depolarization of both ventricles
- Q: first negative deflection
- R: first positive deflection
- S: negative deflection after R
- Normal duration: < 0.12 s (3 small squares)
- Despite ventricles being larger than atria, QRS ≈ P wave duration because the His-Purkinje system conducts much faster than atrial tissue
- Wide QRS (>0.12 s) = bundle branch block, ventricular rhythm, or pre-excitation
🔵 ST Segment — Early Ventricular Repolarization
- The flat (isoelectric) portion after the QRS, before the T wave
- Corresponds to the plateau phase of the ventricular action potential
- Elevation → injury/infarction, pericarditis
- Depression → ischemia, posterior MI, digoxin effect
🔵 T Wave — Ventricular Repolarization
- Represents repolarization of the ventricles
- Normally upright in I, II, V3–V6; inverted in aVR; variable in III, aVL, V1
- Peaked T waves → hyperkalemia (early)
- Inverted T waves → ischemia, strain, post-MI, PE
🔵 QT Interval — Total Ventricular Activity
- Measured from start of QRS to end of T wave
- Represents full ventricular depolarization + repolarization
- Normal corrected QTc: < 0.44 s in men; < 0.46 s in women
- Prolonged QTc → risk of torsades de pointes; caused by drugs, hypokalaemia, hypomagnesaemia, long QT syndrome
5. Heart Rate Calculation
Regular rhythm:
$$\text{Heart Rate} = \frac{300}{\text{Number of large squares between R waves}}$$
| Large squares (R-R) | Rate (bpm) |
|---|---|
| 1 | 300 |
| 2 | 150 |
| 3 | 100 |
| 4 | 75 |
| 5 | 60 |
| 6 | 50 |
Normal: 60–100 bpm | Bradycardia: <60 | Tachycardia: >100
For irregular rhythms (e.g., AF): count number of QRS complexes in a 6-second strip and multiply by 10.
6. Normal Sinus Rhythm (NSR)
Here is what a completely normal 12-lead ECG looks like:
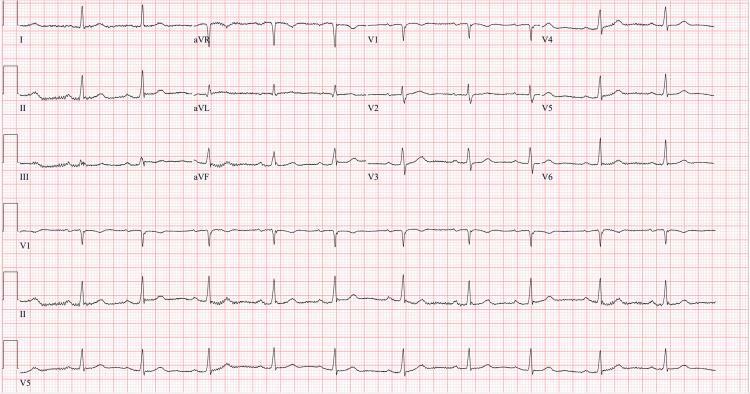
Criteria for Normal Sinus Rhythm:
- Rate 60–100 bpm
- Regular P waves — one before every QRS
- P wave upright in II, inverted in aVR
- PR interval 0.12–0.20 s
- QRS < 0.12 s
- Normal axis (0° to +90°)
7. The Electrical Axis
The mean QRS axis tells you the overall direction of ventricular depolarization in the frontal plane. It is determined using the hexaxial reference system:
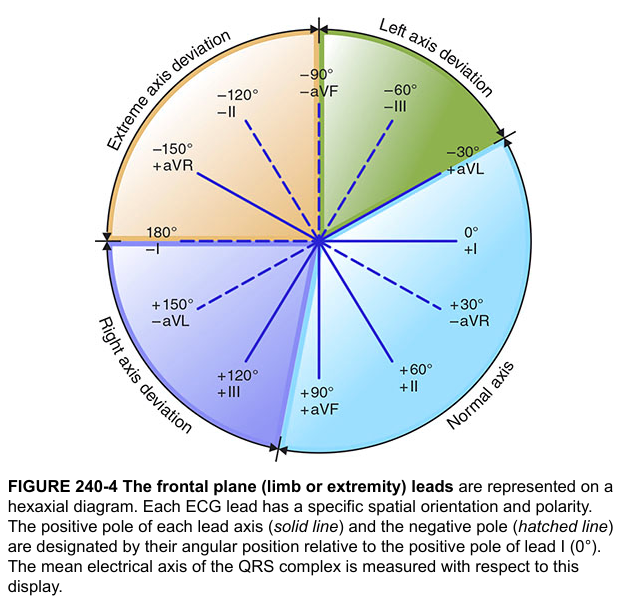
Quick Axis Check (Lead I + aVF method)
| Lead I | aVF | Axis |
|---|---|---|
| ➕ Positive | ➕ Positive | Normal (0° to +90°) |
| ➕ Positive | ➖ Negative | Left axis deviation (LAD) |
| ➖ Negative | ➕ Positive | Right axis deviation (RAD) |
| ➖ Negative | ➖ Negative | Extreme/northwest axis |
Causes of LAD: Left anterior fascicular block, inferior MI, LVH, LBBB
Causes of RAD: RVH, PE, lateral MI, RBBB, normal in children
8. A Systematic Approach to ECG Reading
Use this step-by-step method every time — never skip steps:
1. RATE → Fast/normal/slow?
2. RHYTHM → Regular or irregular?
3. P WAVES → Present? Shape? One per QRS?
4. PR INTERVAL → 0.12–0.20 s?
5. QRS → Narrow (<0.12 s) or wide?
6. ST SEGMENT → Isoelectric, elevated, or depressed?
7. T WAVES → Upright? Inverted? Peaked?
8. QT INTERVAL → Prolonged?
9. AXIS → Normal, left, right?
10. COMPARE → With old ECG if available
9. Common ECG Patterns
9A. ST Elevation MI (STEMI) — Anterior

Recognising MI by territory:
| ST elevation leads | Territory | Artery |
|---|---|---|
| V1–V4 | Anterior | LAD |
| V1–V6 + I, aVL | Anterolateral | Proximal LAD |
| II, III, aVF | Inferior | RCA (80%) or LCx |
| I, aVL, V5–V6 | Lateral | LCx or diagonal |
| V1–V3 depression (reciprocal) | Posterior | RCA or LCx |
Reciprocal changes (depression in leads opposite to elevation) confirm true STEMI and help localise it.
9B. Atrial Fibrillation (AF)
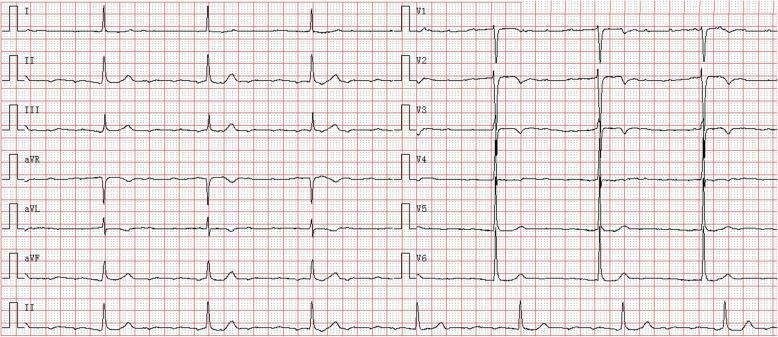
Key features of AF:
- No distinct P waves (replaced by irregular fibrillatory baseline, best seen in V1)
- Irregularly irregular R-R intervals
- Narrow QRS (unless aberrant conduction)
- Ventricular rate 100–180 bpm if uncontrolled
9C. Heart Block (Complete/3rd Degree)
On the AF + complete heart block ECG above: atrial rate ≈180 bpm, ventricular rate ≈43 bpm — with complete AV dissociation (P waves and QRS complexes marching independently).
| Type | PR interval | Dropped beats |
|---|---|---|
| 1st degree | Prolonged >0.20 s, constant | None |
| 2nd degree Mobitz I (Wenckebach) | Progressively lengthens | Yes, then resets |
| 2nd degree Mobitz II | Constant, then suddenly drops | Yes, without warning |
| 3rd degree (complete) | P and QRS unrelated | Total dissociation |
9D. Bundle Branch Blocks
Right Bundle Branch Block (RBBB):
- QRS > 0.12 s
- rSR' ("rabbit ears") in V1
- Wide, slurred S wave in I, V5, V6
- T wave inverted in V1–V2
Left Bundle Branch Block (LBBB):
- QRS > 0.12 s
- Broad notched R wave in I, V5, V6 ("WiLLiaM" pattern)
- Deep QS in V1 ("MoRRoW" pattern)
- No septal Q waves in lateral leads
- New LBBB with chest pain = treat as STEMI equivalent
Memory tip: WiLLiaM MoRRoW — Left bundle = W in V1, M in V6; Right bundle = M in V1, W in V6.
10. Key Normal Values — Quick Reference
| Measurement | Normal Range |
|---|---|
| Heart rate | 60–100 bpm |
| P wave duration | < 0.12 s (< 3 small sq) |
| PR interval | 0.12–0.20 s (3–5 small sq) |
| QRS duration | < 0.12 s (< 3 small sq) |
| QTc (corrected) | < 0.44 s (men), < 0.46 s (women) |
| QRS axis | 0° to +90° (normal) |
| R-wave progression | V1 (small r) → V6 (tall R) |
| ST segment | Isoelectric ± 1 mm |
11. R-Wave Progression
In the precordial leads (V1→V6), the R wave should get progressively taller (and S wave smaller). The transition (where R = S) normally occurs around V3–V4.
- Poor R-wave progression (R remains small through V4) → anterior MI, LBBB, RVH
- Early transition (R > S by V1–V2) → posterior MI, RVH
12. Electrolyte Effects on ECG
| Electrolyte | ECG Change |
|---|---|
| Hyperkalemia | Peaked T → wide QRS → sine wave → asystole |
| Hypokalemia | Flat T, prominent U wave, prolonged QU |
| Hypercalcemia | Short QT |
| Hypocalcemia | Long QT (prolonged ST segment) |
Summary: The 10 Questions to Ask Every ECG
- What is the rate?
- Is the rhythm regular or irregular?
- Are P waves present and normal?
- Is the PR interval 0.12–0.20 s?
- Is the QRS narrow or wide?
- Is the ST segment elevated, depressed, or flat?
- Are T waves normal?
- Is the QT interval prolonged?
- What is the axis?
- Are there signs of hypertrophy, ischaemia, or infarct?
Sources: Costanzo Physiology 7th Ed. | Braunwald's Heart Disease | Harrison's Principles of Internal Medicine 21st Ed. | Images from PMC clinical repository and Harrison's textbook atlas.
This is a shared conversation. Sign in to Orris to start your own chat.