CXR findings in lung collapse
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive content from Grainger & Allison's Diagnostic Radiology. Let me compile the full answer.
CXR Findings in Lung Collapse (Atelectasis)
Source: Grainger & Allison's Diagnostic Radiology, Chapter 7 - Lobar Collapse
Overview
Collapse (atelectasis) refers to loss of lung volume. The two cardinal features on CXR are:
- Increased opacity of the affected lobe
- Volume loss - inferred by direct and indirect signs
A collapsed lobe appears dense because retained secretions/fluid replace air; however, nearly complete collapse is needed before opacity becomes obvious on CXR.
Direct Signs of Volume Loss
These are the most reliable signs:
| Sign | Details |
|---|---|
| Fissure displacement | Most reliable direct sign; displaced in a characteristic direction depending on lobe affected |
| Crowding of vessels and bronchi | Pulmonary vessels and bronchi pack together within the collapsed lobe; often an early sign |
| Hilar elevation | Classic sign of upper lobe collapse; the ipsilateral hilum rides superiorly |
| Hilar depression / small hilum | Lower lobe collapse; the collapsed lobe obscures the lower lobe artery, making the hilum appear small rather than clearly depressed |
| Bronchial displacement | Upper lobe collapse swings the ipsilateral main bronchus horizontally; lower lobe collapse swings it vertically |
Indirect Signs of Volume Loss
These reflect compensatory changes in adjacent structures:
| Sign | Details |
|---|---|
| Compensatory hyperinflation | Remaining ipsilateral lobes expand to fill the space; hyperlucent on CXR |
| Mediastinal shift | Toward the side of collapse; upper lobe collapse shifts the superior mediastinum; lower lobe collapse is often less dramatic |
| Tracheal deviation | Toward the side of collapse in upper/whole lung collapse |
| Hemidiaphragm elevation | Particularly the posterior portion in lower lobe collapse |
| Elevation of hilum | Ipsilateral hilum pulled upward in upper lobe collapse |
| Herniation of contralateral lung | Especially the right lung crossing anterior midline in left lung collapse (seen on lateral view as anterior hyperlucency) |
Special CXR Signs
Golden's S Sign (S Sign of Golden)
Seen in right upper lobe collapse due to central carcinoma. The collapsed lobe creates a peripheral concavity, while the central tumour mass creates a convexity - together forming a reverse-S or sigmoid curve along the displaced horizontal fissure.
Air Bronchogram
- Seen when airways remain patent within collapsed/consolidated lung
- On CXR, suggests the collapse is NOT due to endobronchial obstruction (e.g., pneumonia causing passive collapse)
- Caution: on CT, air bronchograms can still be present peripherally even with a central obstructing mass (due to collateral air drift or tumour necrosis) - so this sign is less reliable on CT than on CXR
Lobar Collapse Patterns
Right Upper Lobe (RUL) Collapse
- Horizontal fissure and upper half of oblique fissure displace upward
- Opacified lobe forms a wedge at the right apex, with increased paramediastinal density
- On PA CXR may mimic an apical fluid cap
- Lateral view: superior displacement of the oblique fissure confirms it
- Tight collapse = roughly triangular anterior wedge on CT
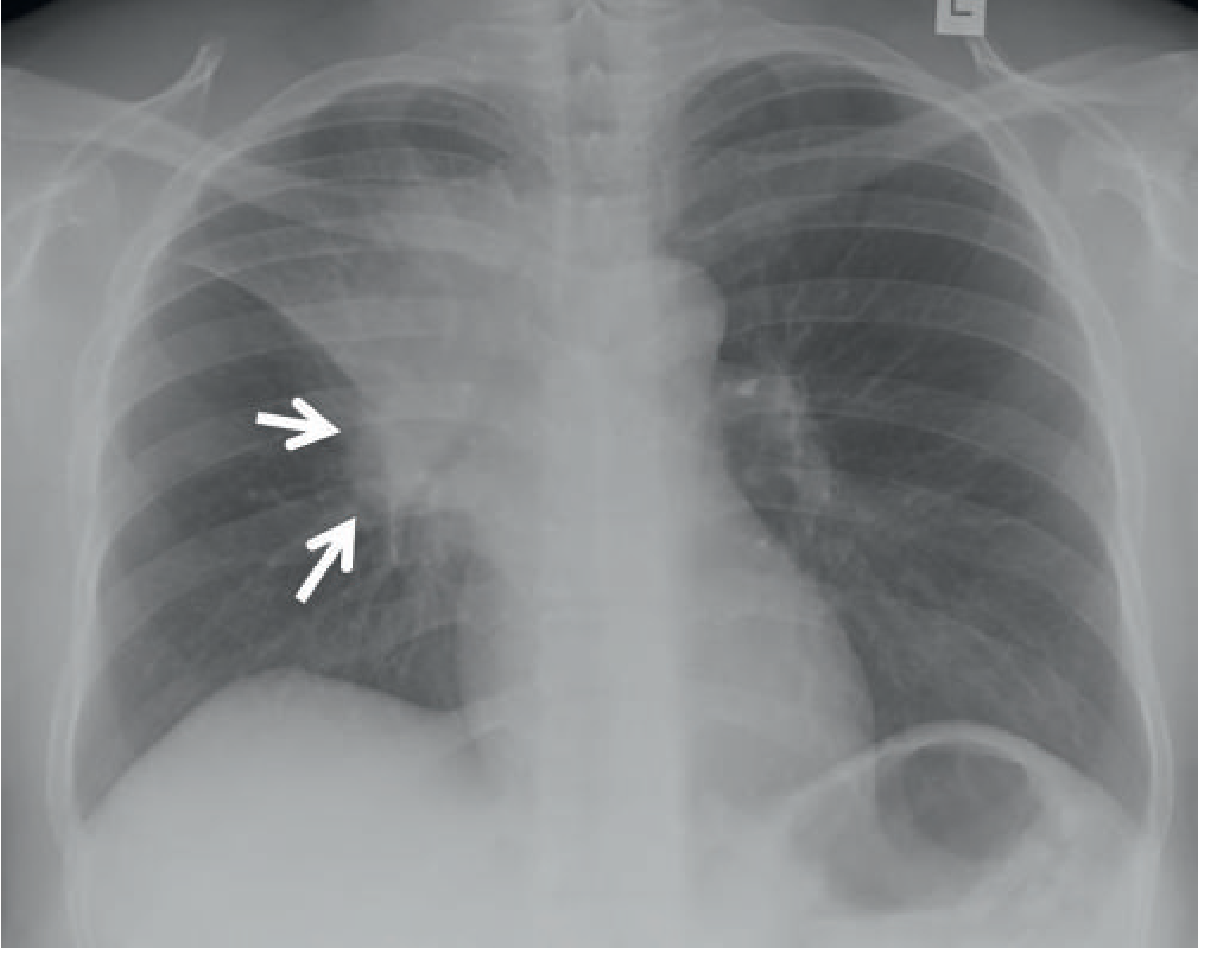
Right Middle Lobe (RML) Collapse
- Both fissures (horizontal and oblique) displace toward each other
- On PA CXR, only a subtle haziness near the right heart border (loss of right heart border = silhouette sign)
- Lateral view: classic triangular wedge with apex pointing toward the hilum - much better demonstrated than on PA
- Middle lobe syndrome: chronic RML collapse with bronchiectasis, classically from focal bronchostenosis (e.g. post-TB)
Left Upper Lobe (LUL) Collapse
- More subtle on PA CXR than RUL (no horizontal fissure on the left)
- Creates a veil-like haziness over the entire left hemithorax
- The aortic knuckle margin may be lost (silhouette sign)
- Lateral view: oblique fissure swings forward - the collapsed lobe lies anteriorly against the chest wall
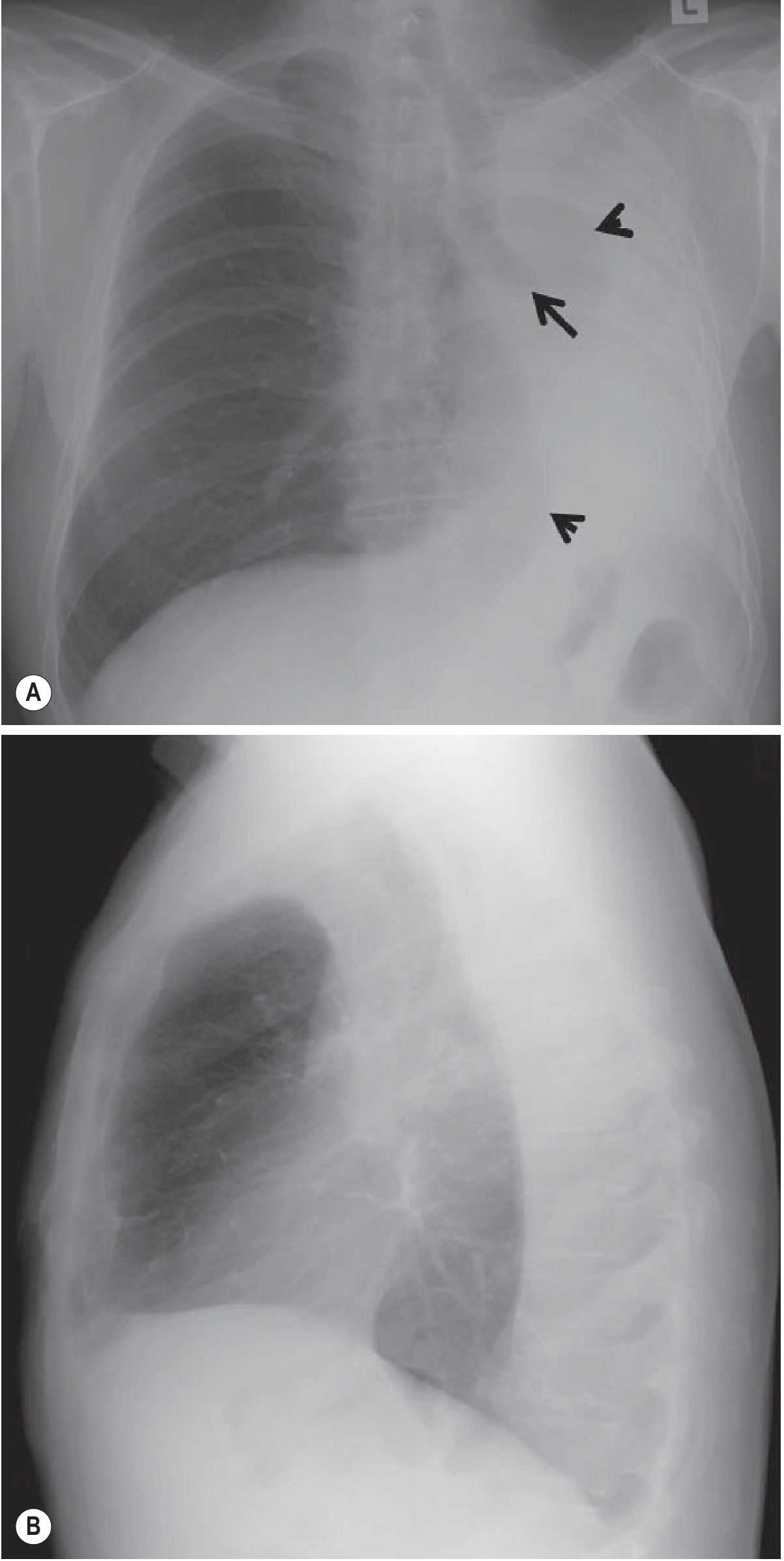
Right and Left Lower Lobe Collapse
- The oblique fissure displaces posteriorly and medially
- Collapsed lobe lies in the posteromedial chest
- On PA CXR: triangular density behind the heart (a wedge-shaped opacity overlying the spine and heart)
- Medial hemidiaphragm contour may be obscured (no longer outlined by aerated lung)
- On lateral CXR: posterior hemidiaphragm may be obscured; importantly, vertebrae appear progressively denser inferiorly - the reverse of normal (normally vertebrae get darker inferiorly as overlying lung increases)
- Elevated hemidiaphragm on the affected side
Total Lung Collapse
- Entire hemithorax opacified
- Massive mediastinal shift toward the side of collapse
- Compensating contralateral lung may herniate across midline
Silhouette Sign
When a collapsed/opacified lobe abuts a mediastinal or diaphragmatic border, that border is obliterated (silhouetted out):
- RML collapse → loss of right heart border
- LUL collapse → loss of left heart border / aortic knuckle
- Lower lobe collapse → loss of diaphragm outline (medial portion)
This sign helps localize which lobe is affected.
Summary Table: Lobar Collapse on PA CXR
| Lobe | Opacity location | Fissure movement | Silhouette sign | Key clue |
|---|---|---|---|---|
| RUL | Right apex/paratracheal | Horizontal fissure up | Right paratracheal | Golden S if tumour |
| RML | Right heart border region | Horizontal down, oblique up | Right heart border lost | Best seen on lateral |
| RLL | Behind heart, right base | Oblique fissure posteromedial | Right hemidiaphragm | Triangular retrocardiac density |
| LUL | Entire left hemithorax (veil) | Oblique swings anterior | Left heart border / aorta | Veil sign |
| LLL | Behind heart, left base | Oblique fissure posteromedial | Left hemidiaphragm | Triangular retrocardiac density |
Grainger & Allison's Diagnostic Radiology, Chapter 7 (Lobar Collapse), Susan J. Copley
This is a shared conversation. Sign in to Orris to start your own chat.