I now have comprehensive textbook content. Let me compile the complete guide.
ABG Interpretation and Treatment Plan
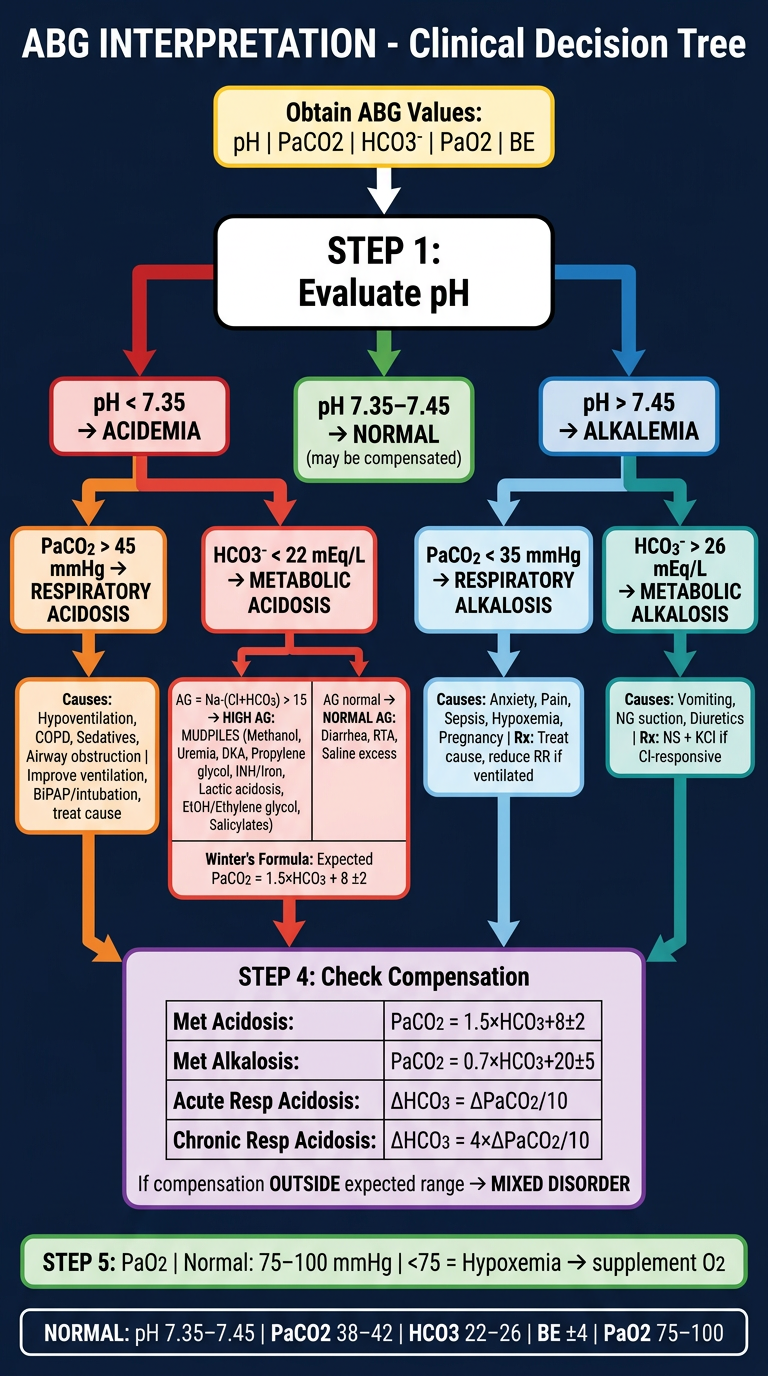
Normal Values (Reference)
| Parameter | Normal Value | Range |
|---|
| pH | 7.40 | 7.35 - 7.45 |
| PaCO2 | 40 mmHg | 38 - 42 mmHg |
| PaO2 | 100 mmHg | 75 - 100 mmHg |
| HCO3- | 24 mEq/L | 22 - 26 mEq/L |
| Base Excess | 0 | -4 to +4 |
Step-by-Step ABG Interpretation
Step 1 - Evaluate the pH
- < 7.35 = Acidemia
- > 7.45 = Alkalemia
- 7.35 - 7.45 = Normal (may still have a compensated disorder)
Step 2 - Evaluate PaCO2 (Respiratory Component)
- In respiratory disorders, PaCO2 changes opposite to pH:
- PaCO2 high + pH low = Respiratory acidosis
- PaCO2 low + pH high = Respiratory alkalosis
- In metabolic disorders, PaCO2 changes same direction as pH (compensation)
Step 3 - Evaluate HCO3- (Metabolic Component)
- HCO3- < 22 = Metabolic acidosis
- HCO3- > 26 = Metabolic alkalosis
Step 4 - Evaluate Base Excess (BE)
- BE is the amount of base needed to titrate 1 L of blood to pH 7.4 at 37°C
- > +4 = Metabolic alkalosis
- < -4 (base deficit) = Metabolic acidosis
Step 5 - Assess Oxygenation (PaO2)
- PaO2 < 75 mmHg = Hypoxemia
- Do not overlook this - hypoxemia may drive or accompany an acid-base disorder
Checking for Adequate Compensation
Always verify that compensation is appropriate. If it is not, a mixed disorder is present.
| Primary Disorder | Compensation Formula |
|---|
| Metabolic acidosis | PaCO2 = 1.5 × [HCO3-] + 8 ± 2 (Winter's Formula) |
| Metabolic alkalosis | PaCO2 = 0.7 × [HCO3-] + 20 ± 5 |
| Acute respiratory acidosis | ↑ HCO3- = ΔPaCO2 / 10 |
| Chronic respiratory acidosis | ↑ HCO3- = 4 × (ΔPaCO2 / 10) |
| Acute respiratory alkalosis | ↓ HCO3- = 2 × (ΔPaCO2 / 10) |
| Chronic respiratory alkalosis | ↓ HCO3- = 4 × (ΔPaCO2 / 10) |
Rule of 15 (quick bedside check for metabolic acidosis):
- HCO3- + 15 should approximately equal the last two digits of pH × 100
- Expected PaCO2 ≈ HCO3- + 15 (for HCO3- > 10)
- For HCO3- < 10: expected PaCO2 ≈ 15 mmHg (± 2)
Metabolic Acidosis
Definition: HCO3- < 22 mEq/L
Calculate the Anion Gap (AG)
AG = Na+ - (Cl- + HCO3-)
- Normal AG: 9 - 15 mmol/L (threshold of 15 used clinically)
Wide Anion Gap Metabolic Acidosis - MUDPILES mnemonic
| Letter | Cause |
|---|
| M | Methanol, muscle injury (rhabdomyolysis), metformin |
| U | Uremia (renal failure) |
| D | Diabetic ketoacidosis (DKA), alcoholic or starvation ketoacidosis |
| P | Propylene glycol, paraldehyde |
| I | Isoniazid, iron |
| L | Lactic acidosis |
| E | Ethanol, ethylene glycol |
| S | Salicylates, short gut |
Normal Anion Gap Metabolic Acidosis (Hyperchloremic)
Causes: diarrhea, GI fistulas, excessive NG suctioning, renal tubular acidosis (RTA), excessive normal saline administration
Delta Gap (for wide AG acidosis)
Used to detect a concurrent metabolic alkalosis or normal-AG acidosis:
- Delta AG = measured AG - 15
- Delta HCO3- = 24 - measured HCO3-
- If Delta AG ≈ Delta HCO3- → pure wide AG metabolic acidosis
- If Delta AG > Delta HCO3- → concurrent metabolic alkalosis
- If Delta AG < Delta HCO3- → concurrent normal AG acidosis
Treatment
- Treat the underlying cause (DKA: insulin + fluids; lactic acidosis: improve perfusion; renal failure: dialysis)
- For diarrhea/GI losses: correct fluid and electrolytes, address source
- Sodium bicarbonate: generally reserved for severe acidosis (pH < 7.1 or HCO3- < 5) or non-anion-gap acidosis; avoid if respiratory compensation is in play without ventilatory support
Metabolic Alkalosis
Definition: HCO3- > 26 mEq/L
Common Causes:
- Vomiting / NG suctioning (hypochloremic, hypokalemic metabolic alkalosis)
- Diuretic use
- Hypovolemia (renal HCO3- retention)
Treatment:
- Treat underlying cause
- For chloride-responsive (chloride loss from vomiting/NG): give normal saline (Cl- replacement) + potassium supplementation
- Stop diuretics if causative
- Judicious fluid resuscitation for hypovolemic patients
Respiratory Acidosis
Definition: PaCO2 > 42 mmHg (hypercapnia) with pH < 7.35
Causes: Hypoventilation from:
- CNS depression (sedatives, opioids, stroke, TBI)
- Neuromuscular disease (myasthenia gravis, Guillain-Barré, hypophosphatemia)
- Airway obstruction (COPD, asthma, foreign body)
- Severe pneumonia, pulmonary edema, ARDS
Treatment:
- Improve ventilation: supplemental O2, non-invasive positive pressure ventilation (BiPAP/CPAP), or intubation/mechanical ventilation if severe
- For COPD: target SpO2 88-92% to avoid abolishing hypoxic drive
- Reverse contributing factors: naloxone for opioid overdose, flumazenil for benzo overdose
- Do not overcorrect in chronic respiratory acidosis - normalizing PaCO2 too quickly causes metabolic alkalosis (post-hypercapnic alkalosis)
Respiratory Alkalosis
Definition: PaCO2 < 38 mmHg with pH > 7.45 (hyperventilation)
Causes:
- Anxiety/hyperventilation syndrome
- Pain, fever, sepsis
- Pregnancy (progesterone-driven)
- Hypoxemia (compensatory hyperventilation)
- Salicylate toxicity (early stage), hepatic encephalopathy, CNS disease
Treatment:
- Treat underlying cause
- Anxiety-driven: rebreathing, reassurance, anxiolytics
- If on mechanical ventilation: reduce respiratory rate or tidal volume
- Correct hypoxemia if present
Mixed Disorders - Key Clues
| Pattern | Think of |
|---|
| pH normal, PaCO2 high, HCO3- high | Chronic respiratory acidosis with full metabolic compensation |
| pH very abnormal despite "normal" PaCO2 and HCO3- | Mixed opposing disorders canceling each other |
| Compensation exceeds predicted range | Second primary disorder present |
| AG metabolic acidosis + high HCO3- | Concurrent metabolic alkalosis (Delta gap > Delta HCO3-) |
Quick Bedside Algorithm
pH < 7.35 → Acidemia
├── PaCO2 > 45 → Respiratory acidosis
│ └── Is HCO3- appropriately elevated? If not → Mixed
└── HCO3- < 22 → Metabolic acidosis
└── Calculate AG → Wide vs. Normal AG
└── Check compensation with Winter's Formula
pH > 7.45 → Alkalemia
├── PaCO2 < 35 → Respiratory alkalosis
│ └── Is HCO3- appropriately low? If not → Mixed
└── HCO3- > 26 → Metabolic alkalosis
└── Chloride-responsive vs. chloride-resistant
VBG vs. ABG Note
A venous blood gas (VBG) is a reasonable screening alternative:
- VBG pH is ~0.03 lower than ABG pH
- VBG PCO2 is ~5-9 mmHg higher than PaCO2
- PvCO2 < 45 mmHg has ~100% NPV for ruling out significant hypercapnia
- VBG + SpO2 (pulse oximetry) covers most patients; reserve ABG for complex cases or severe respiratory illness
(Current Surgical Therapy 14e, p. 1608; Rosen's Emergency Medicine, p. 1481)
If you have a specific ABG result you'd like interpreted (pH, PaCO2, PaO2, HCO3-, clinical context), paste the values and I'll walk through a full interpretation with a targeted treatment plan.