Liquid biopsy
Reading File
Finding Sources
Searching PubMed
"liquid biopsy" AND cancer
Searching the Web
liquid biopsy clinical applications 2025 2026
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
I now have rich textbook content and a high-quality diagram. Let me compile the full answer.
Liquid Biopsy
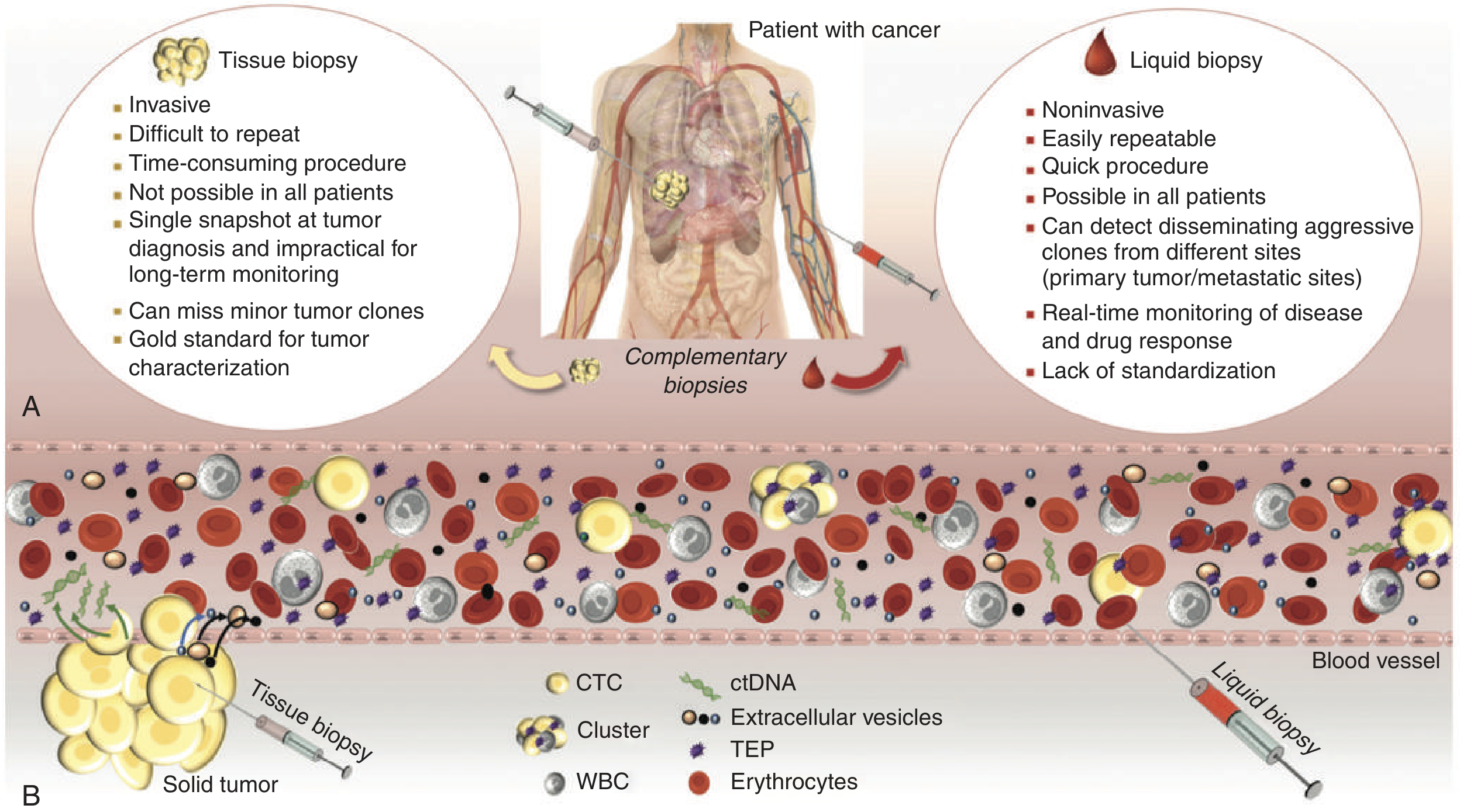
Figure: Tissue and liquid biopsies as complementary approaches. Liquid biopsy collects CTCs, ctDNA, extracellular vesicles, and tumour-educated platelets (TEPs) from a peripheral blood draw. - Tietz Textbook of Laboratory Medicine, 7th Ed.
Definition
Liquid biopsy extracts molecular information from a tumour by detailed analysis of circulating tumour-derived material in the bloodstream (or other body fluids). Unlike solid tissue biopsy - which provides a single snapshot and cannot always be repeated - liquid biopsy can be performed serially from a peripheral blood draw to monitor tumour genome and transcriptome evolution over time. - Tietz Textbook of Laboratory Medicine, 7th Ed., p. 2843
Sources of Material (Components)
| Component | Abbreviation | What it is |
|---|---|---|
| Circulating tumour cells | CTCs | Intact tumour cells that have intravasated into blood from primary or metastatic sites |
| Circulating tumour DNA | ctDNA | Short fragments of tumour-derived cell-free DNA released by apoptotic/necrotic tumour cells |
| Circulating miRNAs | - | Small non-coding RNAs shed by tumour cells, often packaged in exosomes |
| Extracellular vesicles / exosomes | EVs | Membrane-enclosed particles carrying DNA, RNA, and proteins from the tumour |
| Tumour-educated platelets | TEPs | Platelets whose RNA cargo is altered by tumour-derived signals |
Circulating Tumour Cells (CTCs)
- First described by Thomas Ashworth in 1869.
- CTCs originate from primary and metastatic tumours, enter circulation, and may extravasate to seed distant organs.
- CellSearch system (FDA-cleared): positive selection using anti-EpCAM antibodies for breast (2004), colorectal (2008), and prostate cancer (2008).
- In breast cancer, ≥5 CTCs per 7.5 mL blood before neoadjuvant therapy increases recurrence risk >6-fold, independent of primary tumour response.
- High CTC count correlates with decreased progression-free survival (PFS) and overall survival (OS) in operable and metastatic breast cancer.
- A new staging category cM0(i+) was introduced to capture patients with isolated circulating/disseminated tumour cells.
- CTCs undergo epithelial-to-mesenchymal transition (EMT), allowing them to evade EpCAM-based detection; mesenchymal-like CTCs are enriched in therapy-refractory patients.
CTC Isolation Strategies
- Positive selection - magnetic beads coated with EpCAM antibodies (e.g., CellSearch). Limitation: misses EpCAM-negative/mesenchymal CTCs.
- Negative selection - deplete WBCs (anti-CD45/CD61), leaving CTCs regardless of EpCAM status (e.g., RosetteSep system).
- Label-independent / physical methods - exploit larger CTC size (vs. 8-10 µm leukocytes), deformability, density; use microfluidic chips, filtration membranes, magnetic sifters, or density-gradient centrifugation (Ficoll).
Circulating Tumour DNA (ctDNA)
- Cell-free DNA shed by tumour cells into circulation, carrying tumour-specific somatic mutations, copy number variants, methylation patterns, and structural rearrangements.
- Detected by:
- Digital PCR (ddPCR) - highly sensitive quantification of known mutations.
- Next-generation sequencing (NGS) / massively parallel sequencing (MPS) - broad mutation profiling.
- BEAMing (beads, emulsion, amplification, magnetics).
- FDA-approved clinical assay: FoundationOne Liquid CDx - detects mutations in 311 genes to guide therapy selection in NSCLC and other cancers.
- ctDNA fraction of cell-free DNA is often very low (<1% in early-stage cancer), making sensitivity the main challenge.
Extracellular Vesicles and miRNA
- Exosomes (30-150 nm) carry tumour-derived proteins, mRNA, miRNA, and DNA; they fuse with recipient cells and can reprogram the tumour microenvironment.
- A 2025 systematic review and meta-analysis confirmed exosome biomarkers in breast cancer have significant diagnostic value.
- Circulating miRNAs are stable in plasma (protected within exosomes or bound to proteins) and show cancer type-specific expression patterns.
Clinical Applications
| Application | Detail |
|---|---|
| Treatment selection | Detect targetable mutations (e.g., EGFR, KRAS, ALK, BRCA) when tissue is unavailable or heterogeneous |
| Resistance monitoring | Serial sampling reveals emergence of resistance mutations (e.g., T790M in NSCLC on EGFR TKIs) before clinical/radiological progression |
| Minimal residual disease (MRD) | Detect residual ctDNA after surgery/chemotherapy to predict relapse |
| Early cancer detection | Multi-marker panels (ctDNA + proteins) - CancerSEEK approach |
| Prenatal diagnosis | Cell-free fetal DNA in maternal blood for trisomies 13, 18, 21 and sex chromosome aneuploidies (non-invasive prenatal testing, NIPT) |
| Tumour heterogeneity | Samples all metastatic sites simultaneously, overcoming single-biopsy sampling bias |
Liquid Biopsy vs. Tissue Biopsy
| Feature | Tissue Biopsy | Liquid Biopsy |
|---|---|---|
| Invasiveness | Invasive, risk of complications | Minimally invasive (venepuncture) |
| Repeatability | Difficult to repeat | Easily repeatable for serial monitoring |
| Accessibility | Not always feasible (location, patient fitness) | Possible in virtually all patients |
| Tumour representation | Single site snapshot; can miss minor clones | Samples from all tumour sites and metastases |
| Real-time monitoring | Impractical | Yes - tracks drug response and resistance |
| Gold standard for diagnosis | Yes (histopathology) | Not yet a replacement for initial diagnosis |
| Standardisation | Well established | Still being standardised |
Both are viewed as complementary - tissue biopsy remains the gold standard for initial diagnosis and histopathological characterisation, while liquid biopsy adds value for therapy monitoring, MRD, and repeat molecular profiling. - Tietz Textbook of Laboratory Medicine, 7th Ed., p. 2879
Current Regulatory Landscape (2025-2026)
- FoundationOne Liquid CDx - FDA-approved comprehensive ctDNA panel (311 genes).
- Guardant360 CDx - FDA-approved for NSCLC, colorectal, and breast cancer companion diagnostics.
- Carelon clinical guidelines (updated June 2026) formally define appropriate use criteria for genetic liquid biopsy in cancer management and surveillance.
- The global liquid biopsy market reached USD 7.05 billion in 2025, projected at ~USD 24-27 billion by 2035 (CAGR ~13-14.5%), driven largely by NGS (65% market share by technology).
Challenges and Future Directions
- Standardisation - Preanalytical variables (blood tube type, transport time, processing) and analytical differences across platforms make interlaboratory comparison difficult. International initiatives (CANCER-ID, ELBS consortium) are addressing this.
- Sensitivity in early-stage cancer - ctDNA levels are extremely low in localised disease; multi-marker combinations (ctDNA + protein markers) improve sensitivity.
- Clinical validation - Large, prospective, multicentre trials (e.g., SOLAL-CELIGNY) are required for FDA/CLIA approval of individual assays.
- Tumour-of-origin identification - Methylation patterns in ctDNA can indicate the organ of origin, enabling multi-cancer early detection (MCED) tests.
- CTC characterisation - Proteomic and transcriptomic profiling of individual CTCs beyond genomics is maturing; RNA-level analysis can reveal which organ site is likely to be colonised.
Recent Evidence (2024-2026)
- A 2024 meta-analysis (JAMA Network Open) confirmed that elevated circulating tumour DNA correlates with worse survival in metastatic breast cancer.
- A 2025 systematic review characterised liquid biopsy biomarkers for cervical cancer, identifying ctDNA, miRNA, and CTCs as promising markers.
- A 2025 review on breast cancer therapeutics highlighted integration of liquid biopsy in monitoring treatment response to CDK4/6 inhibitors and antibody-drug conjugates.
Sources: Tietz Textbook of Laboratory Medicine, 7th Ed. (Ch. 71) | Robbins & Kumar Basic Pathology | PubMed PMIDs 39235812, 40311726, 41226541, 41752108
This is a shared conversation. Sign in to Orris to start your own chat.