Bicolumnar plating of tibia steps
Reading File
Finding Sources
Finding Sources
Searching the Web
bicolumnar plating tibia surgical steps technique
Finding Sources
Finding Sources
Reading Web Page
bicolumnar plating tibia surgical steps technique
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive information to provide a detailed, well-structured answer. Let me compile the full response.
Bicolumnar (Dual) Plating of the Tibial Plateau - Surgical Steps
Bicolumnar plating (also called dual plating) is the definitive surgical technique for high-energy Schatzker type V and VI bicondylar tibial plateau fractures (OTA/AO 41-C). It involves independent fixation of both the lateral and medial (posteromedial) columns through two separate incisions, achieving rigid stability of both condyles.
Concept and Rationale
The tibia's proximal articular surface is conceptualized as two columns:
- Lateral column - lateral tibial plateau, addressed via anterolateral approach
- Medial column - posteromedial plateau, addressed via posteromedial approach
Single-incision dual plating historically resulted in a "dead bone sandwich" effect with infection rates of 73-87%. The modern two-incision technique reduces this to 4.7-8.4%.
A staged protocol is the standard of care: joint-spanning external fixation first (to allow soft tissue recovery), then definitive bicolumnar plating at 7-14 days when the soft tissue envelope allows (skin wrinkling sign).
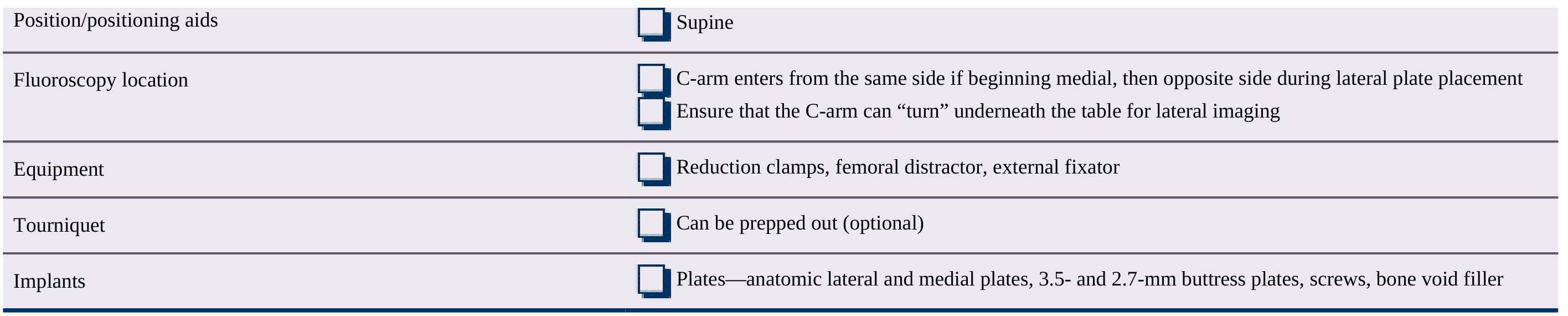
Preoperative Planning Checklist
| Parameter | Detail |
|---|---|
| Table | Radiolucent |
| Position | Supine |
| Fluoroscopy | C-arm enters from the same side when starting medially, then switches to opposite side for lateral plate placement; must be able to "turn" under the table for lateral imaging |
| Equipment | Reduction clamps, femoral distractor, external fixator |
| Tourniquet | Optional (can be prepped out) |
| Implants | Anatomic lateral and medial locking plates; 3.5- and 2.7-mm buttress plates; screws; bone void filler |
Step-by-Step Technique
Step 1 - Patient Positioning
- Supine on a radiolucent table
- Hip bumped to neutral extremity rotation
- Leg elevated on a radiolucent platform
- Leg brought toward a figure-of-four position to access the posteromedial side first (external rotation)
- Pneumatic tourniquet applied (optional)
- Fluoroscopic C-arm confirmed functional before draping
Step 2 - Plan Incisions Before External Fixator Pin Placement
This is a critical pre-operative step: draw out planned incisions before placing any external fixator pins to avoid placing pins in the surgical field. Previous pin sites in the surgical field dramatically increase infection risk.
Step 3 - Posteromedial (Medial Column) Approach - Done First
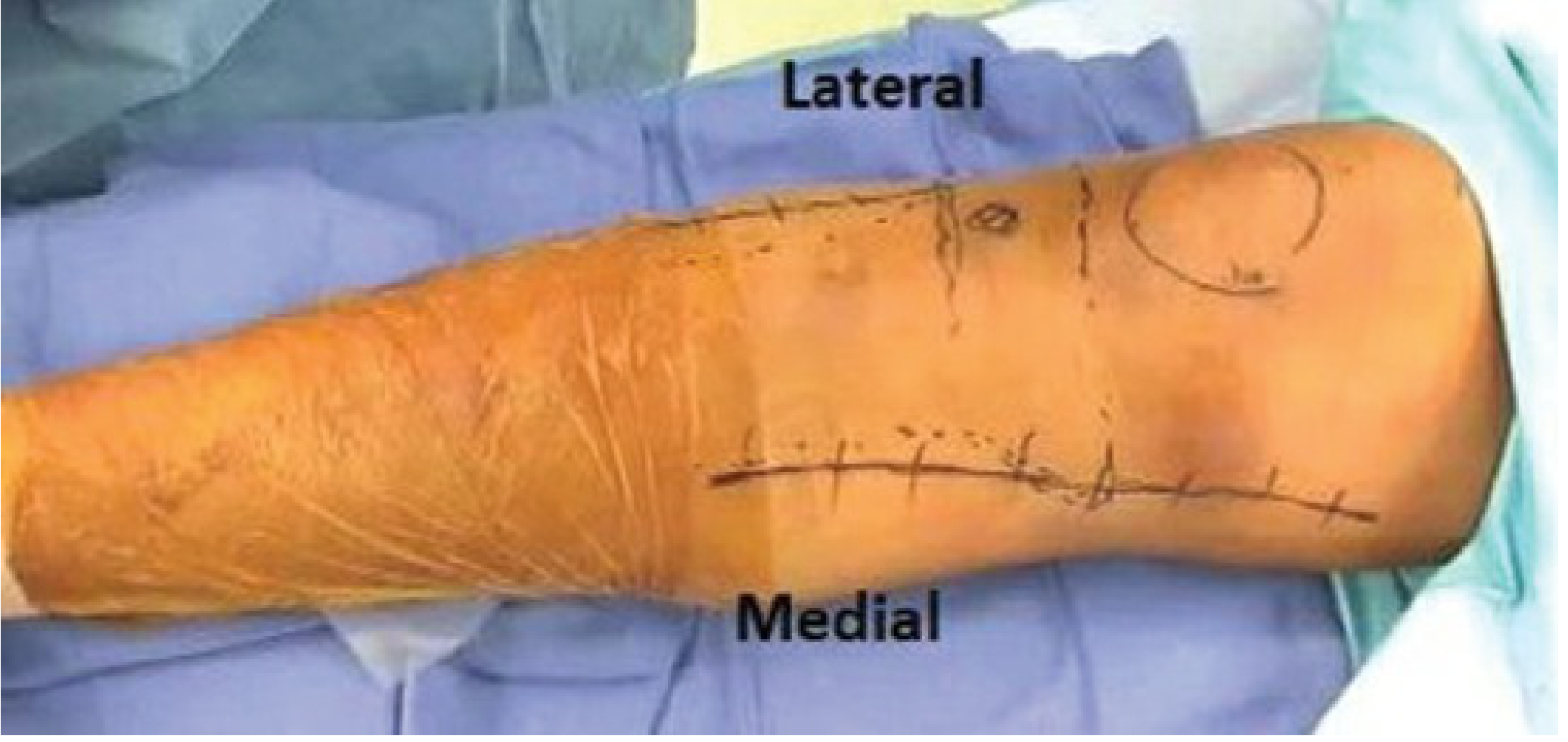
Figure: The anterolateral (lateral) and posteromedial (medial) incisions are nearly 180 degrees apart, so skin bridge compromise is not a concern.
Incision: Longitudinal incision approximately 2 cm posterior to the posteromedial border of the tibial shaft.
Deep dissection:
- Subcutaneous plane - protect the saphenous nerve and vein
- Blunt dissection through the deep fascia
- Deep interval lies between the posterior border of the pes anserine tendons (retracted anteriorly) and the medial head of the gastrocnemius (retracted posteriorly)
- A retractor under the gastrocnemius medial head protects popliteal fossa neurovascular structures
- The popliteus origin is lifted and retracted laterally to directly expose the posteromedial fracture apex
Fracture reduction:
- Use large and small reduction forceps, awls, and elevators
- Intraoperative distraction (manual or with femoral distractor)
- Assess articular reduction fluoroscopically (joint visualization through posteromedial approach is limited)
Fixation - Medial Antiglide Plate:
- Apply a 3.5-mm (or small-fragment LCP/locking) buttress/antiglide plate along the posterior cortex of the medial tibia
- Interfragmentary screws may be placed through the proximal portion of the plate
- Target medial screws anteriorly initially to avoid traversing the articular fracture until the entire joint is reduced
- Limit the number of medial screws initially - excessive medial fixation can interfere with subsequent lateral reduction
Step 4 - Anterolateral (Lateral Column) Approach - Done Second
Incision: Along the anterolateral tibia, starting 1 cm lateral to the anterior tibial crest proximally, extending toward Gerdy's tubercle.
Deep dissection:
- Incise the anterior compartment fascia (preserve a cuff of tissue for closure)
- Elevate the tibialis anterior off the lateral tibial surface subperiosteally if needed
- Lateral meniscus elevated if articular visualization is needed
- Exposure from just below the joint to the mid-shaft
Fracture reduction:
- Restore articular congruity of the lateral plateau
- Reduce depressed fragments by elevating through a cortical window (if present) or through the fracture line
- Use bone void filler (allograft, synthetic, or autograft) to fill subchondral defects
- Place rafting screws close to the articular surface (within 5 mm) before adding void filler - these prevent re-depression
Fixation - Lateral Locking Plate:
- Apply an anatomic proximal tibial locking plate along the lateral cortex
- Position the plate tip just below the joint line
- In the sagittal plane, the plate is slightly anterior to the fibular head
- Fix proximally with locking screws in the plate head - multiple divergent screws raft the articular surface
- Extend distally with locking screws spanning the metaphyseal injury zone using a no-touch / bridge plating technique across the comminuted metaphysis
Step 5 - Confirm Reduction of Both Columns
- Fluoroscopic confirmation of joint congruity in AP and lateral views
- Check mechanical axis alignment: use a Bowie cord (from femoral head to ankle) to verify coronal alignment
- Compare with contralateral limb on fluoroscopy
- Articular step-off should be < 2 mm
- Confirm hardware positioning - no intra-articular screw penetration
Step 6 - Bone Void Filler
- If subchondral defect present after reduction, fill with bone void filler (autograft, allograft, calcium phosphate, or other synthetic substitute)
- Place rafting screws before void filler if possible
Step 7 - Wound Closure
- Irrigate wounds copiously
- Deep fascia closed in layers
- Skin closed over a suction drain (particularly the lateral wound)
- Avoid closing under tension - if skin is compromised, consider leaving open or using VAC
Step 8 - Postoperative Management
- Posterior above-knee splint or back-slab applied immediately
- Non-weight bearing for minimum 8 weeks
- Early range of motion exercises in a hinged brace (once wounds stable) - CPM machine may be used
- Weight bearing progressed guided by clinical and radiographic healing
Key Pitfalls and How to Avoid Them
| Pitfall | Prevention |
|---|---|
| Previous pin sites in surgical field | Plan incisions BEFORE placing external fixator pins |
| Malreduction of posteromedial fragment affecting lateral fixation | Fix posteromedial column first; directly assess fracture reduction |
| Medial screws blocking lateral reduction | Target medial screws anteriorly; limit number of medial screws initially |
| Articular malalignment despite extra-articular reduction | Assess joint reduction fluoroscopically at each step |
| Wound breakdown / deep infection | Staged approach; dual incisions (not single); allow soft tissue recovery; meticulous closure |
| Varus collapse | Adequate medial buttressing; posteromedial column fixation must be completed |
| Limb shortening / malalignment | Use femoral distractor or preexisting external fixator; check Bowie cord axis |
| Injury to saphenous nerve/vein | Careful subcutaneous dissection in posteromedial approach |
| Injury to popliteal structures | Retractor directly on bone under gastrocnemius head |
Summary of Order of Steps
- Staged soft tissue management (temporary ex-fix)
- Preoperative CT planning; draw incisions before pins
- Positioning (supine, figure-of-four for medial first)
- Posteromedial approach - reduce and fix medial column with antiglide/buttress plate (initial limited medial screws)
- Anterolateral approach - reduce lateral plateau, rafting screws, void fill, apply lateral locking plate
- Fluoroscopic confirmation of joint congruity and limb alignment
- Final medial screw placement as needed
- Wound irrigation and layered closure with drains
- Splint application; early ROM, non-weight bearing x 8 weeks
Sources: Rockwood and Green's Fractures in Adults 10th ed 2025, Chapter 62 (Tibial Plateau Fractures, Dual Plating section); Functional Outcomes of Bicolumnar Plating in Schatzker Type V and VI Tibial Plateau Fractures, PMC12276454 (2025).
This is a shared conversation. Sign in to Orris to start your own chat.