Anatomy of the abdomen
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Finding Sources
I now have excellent material and diagrams. Let me compile the comprehensive answer.
Anatomy of the Abdomen
Sources: Gray's Anatomy for Students; General Anatomy and Musculoskeletal System (THIEME Atlas); Mulholland & Greenfield's Surgery
1. Boundaries and Surface Landmarks
The abdomen is the region of the trunk between the thorax and the pelvis. Its surface boundaries are:
- Superior: costal margin (separates it from the thoracic wall)
- Inferior: inguinal ligament (anterior superior iliac spine to pubic tubercle), iliac crest, and pubic symphysis
- Deep superior boundary: the diaphragm, which can rise as high as the 4th costal cartilage during forced expiration on the right
The upper part of the abdominal cavity projects above the costal margin, so organs like the liver, stomach, and spleen are protected by the thoracic cage.
2. Abdominal Regions and Planes
The abdomen is divided using horizontal planes referenced to lumbar vertebral levels. The key planes are shown below:
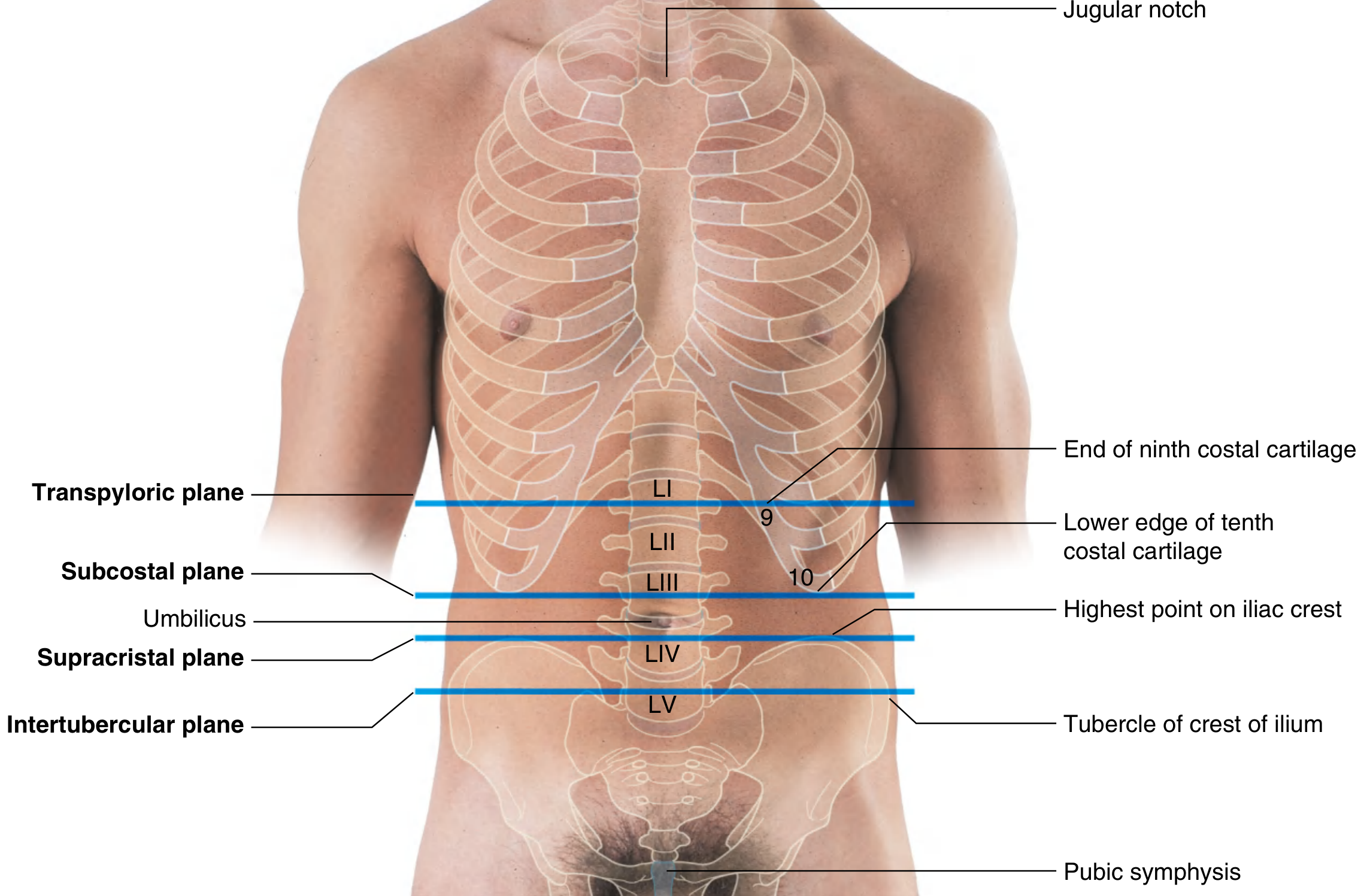
| Plane | Landmark | Vertebral Level |
|---|---|---|
| Transpyloric plane | Medial ends of 9th costal cartilages; midway between jugular notch and pubic symphysis | L1 |
| Subcostal plane | Lower edge of 10th costal cartilage | L3 |
| Supracristal plane | Highest point of iliac crest | L4 |
| Intertubercular plane | Tubercles of iliac crest | L5 |
The umbilicus normally lies at the level of the L3/L4 disc.
Using two vertical (midclavicular) lines and two horizontal planes, the abdomen is divided into 9 regions: right hypochondrium, epigastrium, left hypochondrium, right flank (lateral), umbilical, left flank (lateral), right iliac fossa, hypogastrium (pubic), and left iliac fossa. A simpler clinical system divides the abdomen into 4 quadrants (right upper, left upper, right lower, left lower) by vertical and horizontal lines through the umbilicus.
3. Layers of the Abdominal Wall
From superficial to deep, the anterolateral wall has the following layers:
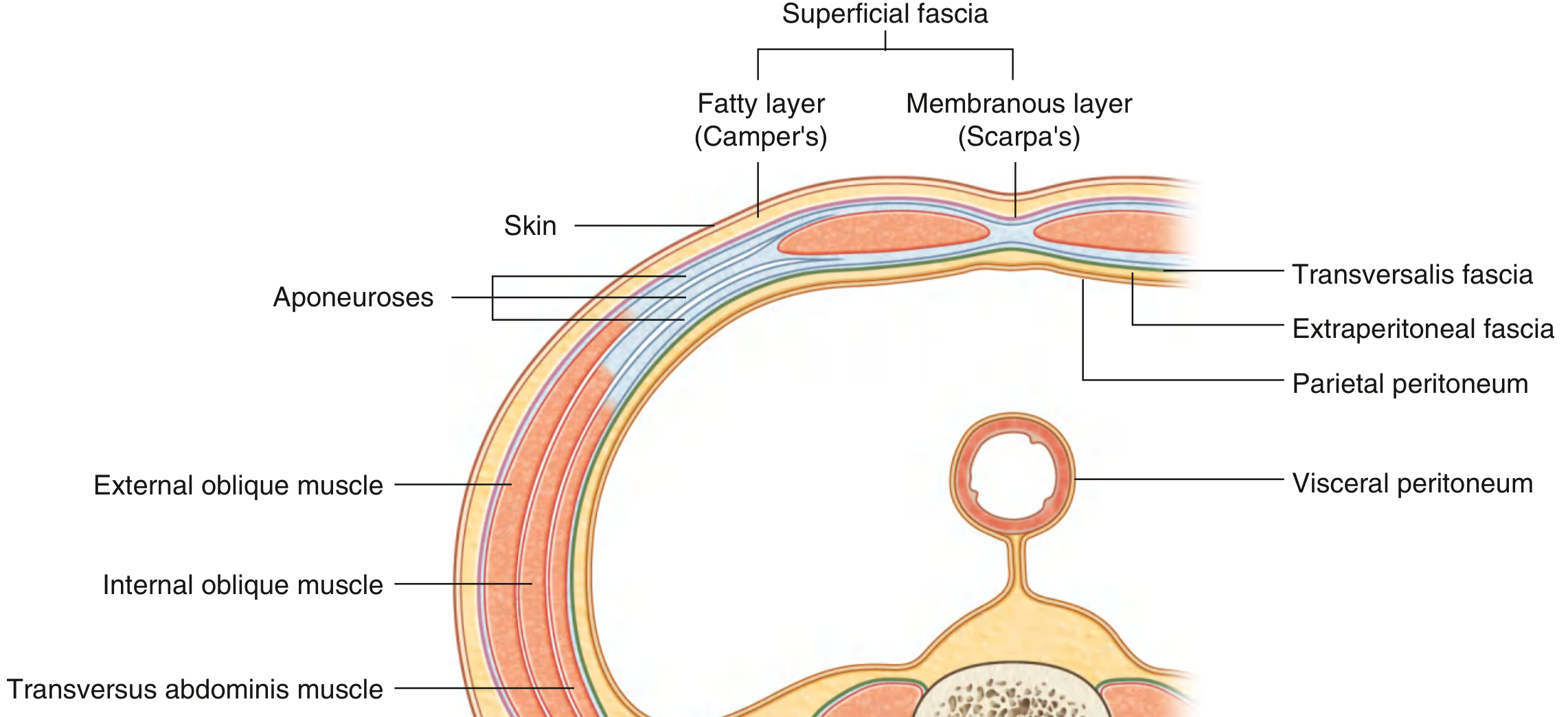
- Skin
- Superficial fascia - two layers:
- Camper's fascia (fatty layer): contains superficial epigastric and superficial circumflex iliac vessels; lymphatics drain into inguinal nodes
- Scarpa's fascia (membranous layer): fuses below the inguinal ligament with the fascia lata of the thigh
- Muscles and aponeuroses (see below)
- Transversalis fascia - lines the deep surface of transversus abdominis
- Extraperitoneal (preperitoneal) fascia - contains variable fat
- Parietal peritoneum
4. Muscles of the Abdominal Wall

Flat muscles (anterolateral group)
| Muscle | Fiber direction | Key features |
|---|---|---|
| External oblique | Inferomedial | Most superficial flat muscle; aponeurosis forms inguinal ligament inferiorly and superficial inguinal ring medially |
| Internal oblique | Superomedial | Middle layer; inferior border forms roof of inguinal canal; gives rise to cremaster muscle in males |
| Transversus abdominis | Horizontal | Deepest flat muscle; aponeurosis passes posterior to rectus above the arcuate line, anterior below it |
Straight (strap) muscles
| Muscle | Features |
|---|---|
| Rectus abdominis | Vertical muscle in the rectus sheath; divided by 3-4 tendinous intersections; from pubic crest/symphysis to xiphoid and costal cartilages 5-7 |
| Pyramidalis | Small triangular muscle anterior to rectus abdominis near pubic symphysis; not always present |
Rectus sheath
Above the arcuate line: anterior wall = external oblique aponeurosis + anterior layer of internal oblique aponeurosis; posterior wall = posterior layer of internal oblique + transversus abdominis aponeurosis.
Below the arcuate line: all three aponeuroses pass anterior to rectus abdominis, so the posterior rectus sheath is absent (only transversalis fascia behind).
Linea alba is the midline fibrous raphe formed by decussating aponeurotic fibers of all three flat muscles, running from xiphoid to pubic symphysis.
5. Peritoneum and Peritoneal Cavity
The peritoneum is a thin serous membrane with two layers:
- Parietal peritoneum: lines the walls of the abdominal and pelvic cavities; innervated by somatic afferents (spinal nerves T7-L1) - produces well-localised pain
- Visceral peritoneum: covers the viscera; innervated by visceral (autonomic) afferents - produces poorly localised, referred pain
The peritoneal cavity is the potential space between these two layers. It is closed in men; in women, the uterine tubes open into it (two small openings), making it semi-closed.
Mesenteries are double folds of peritoneum that suspend intraperitoneal organs and transmit their vessels, nerves, and lymphatics. The greater omentum hangs from the greater curvature of the stomach.
Organ classification by peritoneal relationship
| Type | Definition | Examples |
|---|---|---|
| Intraperitoneal | Suspended by mesentery; almost completely covered by visceral peritoneum | Stomach, jejunum, ileum, transverse colon, liver, spleen |
| Retroperitoneal | Posterior to parietal peritoneum; only anterior surface covered | Kidneys, ureters, aorta, IVC, duodenum (2nd-4th parts), pancreas (body/tail), ascending and descending colon |
6. Abdominal Viscera
Solid organs
- Liver - occupies the right hypochondrium and epigastrium; right dome reaches 4th intercostal space in mid-clavicular line; divided into right and left lobes by the falciform ligament (functionally, by the portal fissure into 8 Couinaud segments)
- Spleen - left hypochondrium, at ribs 9-11; intraperitoneal; vulnerable to rupture with left lower rib fractures
- Pancreas - retroperitoneal; head lies in the duodenal "C-loop"; tail reaches the splenic hilum; transpyloric plane (L1) passes through the neck
- Kidneys - retroperitoneal; right kidney at T12-L3 (lower than left due to the liver); left at T11-L2
Hollow organs
- Stomach - from cardia (T10) to pylorus (L1, transpyloric plane); intraperitoneal
- Duodenum - 25 cm long C-shaped loop around the head of the pancreas; mostly retroperitoneal; duodenojejunal flexure at L2 (suspended by ligament of Treitz)
- Small intestine - jejunum (upper 2/5, left side, thicker walls, prominent plicae circulares) and ileum (lower 3/5, right side, Peyer's patches); ~6 m long; intraperitoneal
- Large intestine - cecum (right iliac fossa), ascending colon (retroperitoneal), transverse colon (intraperitoneal), descending colon (retroperitoneal), sigmoid colon (intraperitoneal), rectum; identified by taeniae coli, haustra, and appendices epiploicae
- Appendix - arises from posteromedial cecum; McBurney's point (2/3 along a line from umbilicus to ASIS); variable position
- Gallbladder - on the visceral surface of the liver; fundus projects at the tip of the 9th costal cartilage in the midclavicular line; bile duct runs in the hepatoduodenal ligament
7. Major Blood Vessels
Arterial supply
The abdominal aorta enters at T12 through the aortic hiatus and bifurcates into the common iliac arteries at L4 (near the umbilicus):
- Celiac trunk (T12/L1): supplies foregut - left gastric, splenic, common hepatic arteries
- Superior mesenteric artery (L1, transpyloric plane): supplies midgut (distal duodenum to 2/3 of transverse colon)
- Inferior mesenteric artery (L3): supplies hindgut (left 1/3 of transverse colon to upper rectum)
- Renal arteries (L1-2): paired, right longer than left
- Gonadal arteries (L2)
- Inferior phrenic and lumbar arteries: parietal branches
Venous drainage
- Portal vein (formed by superior mesenteric vein + splenic vein behind the neck of the pancreas at L2): drains all gastrointestinal tract blood to the liver
- Inferior vena cava (IVC): formed at L5 by union of common iliac veins; receives renal veins, hepatic veins, and inferior phrenic veins
Portosystemic anastomoses are clinically important at: lower esophagus (varices), anal canal (hemorrhoids), paraumbilical region (caput medusae), retroperitoneum.
8. Nerve Supply
Motor and sensory (somatic - abdominal wall)
- T7-T12 intercostal nerves and L1 (iliohypogastric and ilioinguinal nerves) supply the skin, muscles, and parietal peritoneum of the anterolateral wall
- The nerves travel between internal oblique and transversus abdominis, then enter the rectus sheath
Autonomic (viscera)
- Sympathetic: splanchnic nerves (greater = T5-9, lesser = T10-11, least = T12) relay in the celiac, superior mesenteric, and aorticorenal ganglia
- Parasympathetic: vagus nerve (CN X) supplies foregut and midgut to the splenic flexure; pelvic splanchnic nerves (S2-4) supply hindgut
- Visceral pain: poorly localised, referred to dermatomes corresponding to the sympathetic supply level (e.g., appendix pain referred to periumbilical region via T10)
9. Lymphatic Drainage
- Abdominal viscera drain to preaortic nodes (celiac, superior mesenteric, inferior mesenteric nodes) corresponding to their arterial supply
- Lateral aortic (lumbar) nodes drain the kidneys, adrenals, gonads, and posterior abdominal wall
- All ultimately drain into the cisterna chyli at L1-2, which continues as the thoracic duct
10. Inguinal Region
The inguinal canal is a 4 cm oblique passage through the lower abdominal wall:
- Runs from the deep inguinal ring (just above the midpoint of the inguinal ligament) to the superficial inguinal ring (defect in external oblique aponeurosis, above and medial to pubic tubercle)
- In males: transmits the spermatic cord; in females: transmits the round ligament of the uterus
- Hesselbach's (inguinal) triangle - bounded by: inferior epigastric vessels (laterally), lateral edge of rectus abdominis (medially), inguinal ligament (inferiorly) - site of direct inguinal hernias
Gray's Anatomy for Students, pp. 346-347, 362, 466-468 | General Anatomy and Musculoskeletal System (THIEME Atlas), pp. 197, 213 | Mulholland & Greenfield's Surgery, pp. 3632-3633
This is a shared conversation. Sign in to Orris to start your own chat.