Induction of labour Explain 8n details
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the content needed to write a comprehensive, detailed answer. Here is the full explanation:
Induction of Labour - Detailed Overview
1. Definition and Background
Induction of labour (IOL) is the artificial initiation of uterine contractions before spontaneous labour begins, with the aim of achieving vaginal delivery. It can be:
- Elective - performed for convenience of the patient or provider, or logistical/psychosocial reasons
- Indicated - performed for a medical, obstetric, or fetal complication where delivery is safer than continuing the pregnancy
The incidence of IOL has risen markedly over decades - from ~9% of all births in 1989 to over 20% today, with significant regional variation.
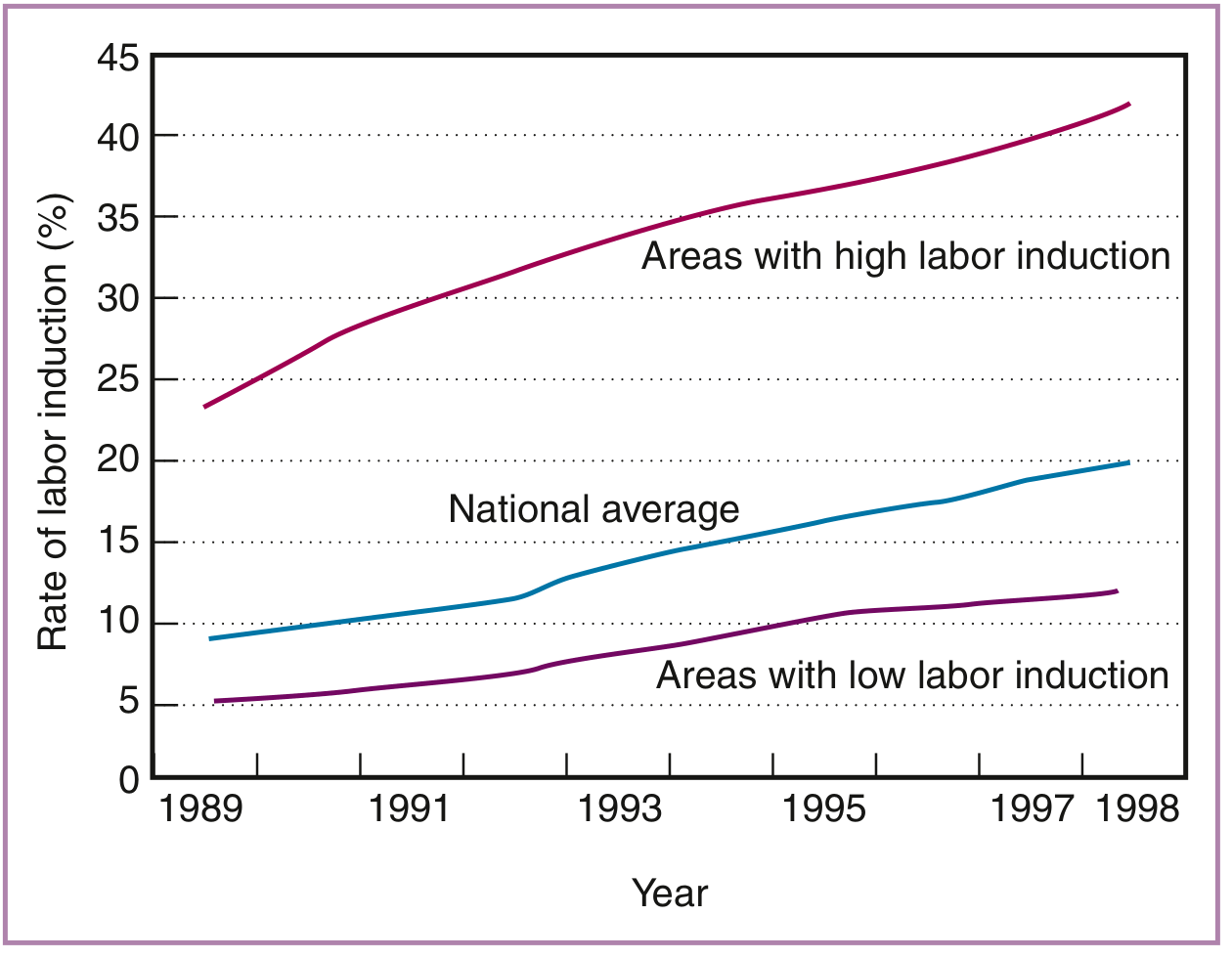
Rising trend in induction rates across the US (Creasy & Resnik's Maternal-Fetal Medicine)
2. Indications
Induction is indicated when the benefits of delivery outweigh the risks of continuing the pregnancy. Pregnancy-induced hypertension and post-term pregnancy account for over 80% of inductions.
Medical/Obstetric Indications
- Pregnancy-induced hypertension / Pre-eclampsia / Eclampsia
- Gestational or pre-existing diabetes mellitus
- Premature rupture of membranes (PROM / PPROM)
- Post-term pregnancy (> 42 weeks) - associated with increased perinatal death, fetal macrosomia, meconium aspiration, dystocia
- Fetal growth restriction (FGR) / Intrauterine growth retardation
- Intrauterine fetal death (IUFD) / Fetal demise
- Chorioamnionitis (intra-amniotic infection)
- Rh isoimmunization / significant alloimmunization
- Oligohydramnios or polyhydramnios
- Non-reassuring antepartum fetal testing
- Maternal chronic renal, cardiac, or pulmonary disease
- Obstetric cholestasis (intrahepatic cholestasis of pregnancy)
Logistical/Psychosocial (Elective) Indications
- Distance from hospital / risk of precipitous delivery
- Rapid prior labours
- Psychological or emotional factors (patient request, partner availability)
- Scheduling for physician/hospital coverage
3. Contraindications
Absolute contraindications mirror those for spontaneous labour and vaginal delivery:
- Previous classical (vertical) uterine incision
- Prior uterine surgery with entry into the cavity (e.g. myomectomy)
- Active genital herpes infection
- Placenta or vasa praevia
- Umbilical cord prolapse
- Transverse or oblique fetal lie
- Cephalopelvic disproportion (CPD)
Relative contraindications:
- Previous low-transverse caesarean section (increased uterine rupture risk; misoprostol is especially cautioned)
- Grand multiparity
- Non-vertex presentation
- Severe fetal compromise where vaginal delivery is unlikely to succeed
4. Pre-induction Assessment - The Bishop Score
The Bishop Scoring System (1964) is the standard tool to quantify cervical readiness (ripeness) for labour. It has a maximum score of 13.
| Factor | 0 | 1 | 2 | 3 |
|---|---|---|---|---|
| Dilation (cm) | 0 | 1-2 | 3-4 | 5-6 |
| Effacement (%) | 0-30 | 40-50 | 60-70 | 80 |
| Station | -3 | -2 | -1 or 0 | +1 or +2 |
| Consistency | Firm | Medium | Soft | - |
| Position | Posterior | Middle | Anterior | - |
Interpretation:
- Score ≥ 9: Favourable - likelihood of successful vaginal delivery approaches that of spontaneous labour. Average duration of labour ~4 hours in multiparas.
- Score ≥ 8: When oxytocin is used, success approaches spontaneous labour.
- Score 6-8: Induction can proceed; cervical ripening may help.
- Score < 6: Unfavourable cervix - cervical ripening is recommended before oxytocin.
- Score ≤ 5 in nulliparas: ~50% risk of failed induction.
Dilation is the single most important component of the Bishop score. A simplified 3-component scoring system (dilation + station + effacement) has been shown to predict vaginal delivery as well as the traditional 5-component system.
5. Cervical Ripening Methods
When the cervix is unfavourable, ripening is required before induction proper.
A. Non-Pharmacological Methods
1. Membrane (Amniotic) Sweeping / Stripping
- The examining finger is inserted through the cervical os and swept circumferentially to detach the membranes from the lower uterine segment
- Stimulates local prostaglandin release
- Requires at least some cervical dilation
- Risks: Rupture of membranes, infection, bleeding, irregular contractions
- Generally safe, especially near post-dates
2. Foley (Balloon) Catheter
- A 16-26 Fr Foley catheter is placed through the cervical os and inflated with 30-60 mL of saline
- Applies mechanical pressure to the lower uterine segment, stimulating local prostaglandin release
- Cervical ripening by mechanical dilation
- Compared with intravaginal PGE2: similar C-section rates, less likely to cause uterine hyperstimulation, but lower rate of delivery within 24 hours
- Preferred in women with prior caesarean section (lower uterine rupture risk than prostaglandins)
3. Laminaria Tents
- Hygroscopic cervical dilators made from dried seaweed (Laminaria digitata or japonica)
- Available in small, medium, large sizes
- Absorb moisture, expand, and progressively dilate the cervix overnight
4. Amniotomy (Artificial Rupture of Membranes - ARM)
- Amnihook is used to rupture the membranes when the cervix is already favourable (Bishop ≥ 6, vertex engaged, cervix ≥ 2 cm dilated, partially effaced)
- Triggers prostaglandin release, stimulates contractions
- Keettel's large series: only 3.4% needed additional oxytocin when cervix was favourable
- Cannot be reversed once performed; risk of cord prolapse if head not engaged
5. Breast Stimulation / Acupuncture - historically used; evidence limited.
B. Pharmacological Methods
1. Dinoprostone (Prostaglandin E2 - PGE2)
Two commercially available forms:
| Preparation | Dose/Form | Route | Interval |
|---|---|---|---|
| Prepidil | 0.5 mg in 2.5 mL gel | Intracervical | Repeat once in 6-12 hours if minimal change |
| Cervidil | 10 mg slow-release insert | Intravaginal | Single 12-hour insert |
- Cervidil has a retrieval system - can be removed if uterine hyperstimulation occurs (advantage over gel)
- May or may not cause uterine contractions; cervical softening appears independent of contraction number
- Previous caesarean section is NOT an absolute contraindication for dinoprostone
- Oxytocin may then be used if spontaneous labour does not ensue
2. Misoprostol (Prostaglandin E1 - PGE1)
- Synthetic PGE1 (Cytotec); FDA-approved for gastric ulcers; used off-label for induction
- More potent than dinoprostone; associated with shorter time to delivery and lower C-section rates in meta-analyses
- Protocol:
- 25 μg vaginally (one-quarter of 100-μg tablet) into vaginal fornix
- Repeat after 4 hours if minimal change
- Hold if: ≥2 contractions in 10 minutes, Bishop score ≥ 8, active labour, or non-reassuring FHR
- Do NOT give oxytocin within 2 hours of last misoprostol dose
- Maximum duration: 24 hours
- Oral misoprostol 100 mg every 3-4 hours is also safe and effective
- Caution / Avoid in women with prior caesarean section or uterine surgery - significantly increased uterine rupture risk
- For fetuses < 28 weeks: 200-400 μg vaginally or orally every 4 hours
3. Oxytocin
The preferred pharmacologic agent when the cervix is already favourable or after successful ripening.
Administration:
- IV infusion only, via infusion pump
- Diluted in lactated Ringer's or normal saline: typically 10-20 units in 1 L (= 10-20 mU/mL)
- Steady-state plasma levels reached ~40 minutes after starting infusion
Dosing Protocols:
| Protocol | Starting Dose | Increment | Interval |
|---|---|---|---|
| Low-dose | 0.5-2 mU/min | 1-2 mU/min | Every 30-60 min |
| High-dose | 4-6 mU/min | 2-6 mU/min | Every 15-40 min |
- Goal: Contractions 2-3 minutes apart, 45-60 second duration, 50-75 mmHg intensity, normal resting tone between contractions
- ~90% of patients respond to ≤ 16 mU/min
- Doses > 20 mU/min have antidiuretic (vasopressin-like) effects - risk of water intoxication and hyponatremia (coma, convulsions, death)
- Continuous EFM and uterine activity monitoring mandatory throughout
6. Confirming Dates Before Induction
Before any elective induction, gestational age must be confirmed by at least one of:
- Fetal heart tones present for 30 weeks (Doppler) or 20 weeks (fetoscope)
- 36 weeks since positive β-hCG
- Crown-rump length at 6-12 weeks confirming GA ≥ 39 weeks
- Ultrasound at 13-20 weeks confirming GA ≥ 39 weeks
- Documented fetal lung maturity by amniocentesis (if < 39 weeks)
Gestational age of at least 39 weeks is required for elective induction to minimize neonatal respiratory morbidity ("wet lung syndrome").
7. Complications
| Complication | Notes |
|---|---|
| Uterine hyperstimulation | >50% contractions of moderate-strong intensity in a 10-minute window; risk of placental abruption |
| Fetal heart rate abnormalities | Tachycardia, decelerations, loss of variability |
| Failed induction | ~2x increased C-section risk in nulliparas with unfavourable cervix |
| Uterine rupture | Especially with misoprostol in women with prior uterine scar |
| Cord prolapse | Especially with amniotomy if head not engaged |
| Fetal acidosis / distress | From uterine hyperstimulation reducing uteroplacental perfusion |
| Iatrogenic prematurity | If dates are miscalculated - neonatal respiratory morbidity |
| Neonatal respiratory morbidity | Wet lung syndrome / persistent fetal circulation if delivered before 39 weeks |
| Water intoxication | With high-dose oxytocin (> 20 mU/min) in aqueous fluid - hyponatremia |
| Precipitous delivery | Rapid uncontrolled delivery causing maternal/fetal trauma |
| Increased NICU admission | Electively induced labours associated with higher NICU rates vs spontaneous labour |
8. Management of Hyperstimulation
If uterine hyperstimulation occurs:
- Assess FHR immediately
- If FHR non-reassuring:
- IV fluid bolus 1000 mL
- Lateral (left) positioning of mother
- Oxygen 10 L/min via non-rebreather mask
- Discontinue/reduce oxytocin (or remove Cervidil insert)
- Consider terbutaline 0.25 mg subcutaneously as tocolytic
- If FHR remains non-reassuring → prepare for immediate delivery (vaginal or caesarean)
Note: Misoprostol and Prepidil gel cannot be removed once administered - unlike Cervidil insert or oxytocin infusion. This is a key practical consideration. Terbutaline should always be available (at least 2 doses) before initiating prostaglandins.
9. Special Situations
Prior Caesarean Section
- Previous low-transverse incision + uterus < 28 weeks: use misoprostol (200-400 μg dosing)
- Previous low-transverse incision + uterus > 28 weeks: oxytocin + Foley catheter ripening (avoid misoprostol)
- Previous classical incision: repeat caesarean is appropriate (IOL contraindicated)
Post-term Pregnancy (> 42 weeks)
- Risks: increased perinatal death, macrosomia, meconium aspiration, labour dystocia
- Induction reduces these risks
- Cochrane review confirms IOL at/beyond term improves birth outcomes
Optimal Timing
- Risk of cerebral palsy is lowest at delivery at 40 weeks - earlier or later increases risk
- The ARRIVE trial (Grobman et al., 6000+ nulliparas) showed elective induction at 39 weeks vs waiting until 41 weeks had no increase in C-section rate and no adverse outcomes
Fetal Demise
- Complete blood count, type and screen on admission; fibrinogen if demise > 4 weeks (DIC risk)
- < 28 weeks: misoprostol 200-400 μg vaginally/orally every 4 hours
-
28 weeks: misoprostol 25-50 μg or standard oxytocin infusion
- Allow spontaneous placental delivery; avoid cord traction to minimize retained placenta
- Rh-negative mothers: administer RhD immune globulin
10. Summary Algorithm
Is induction indicated?
↓ Yes
Confirm gestational age ≥ 39 weeks (elective) OR outweighs risk (indicated)
↓
Assess Bishop score
↓
Score < 6 (unfavourable)?
→ YES: Cervical ripening first
- PGE2: Dinoprostone gel (Prepidil) or insert (Cervidil)
- PGE1: Misoprostol 25 µg vaginally q4h [avoid if prior C-section scar]
- Mechanical: Foley catheter [preferred if prior C-section]
→ NO (Score ≥ 6, ripe cervix):
- Amniotomy (if vertex engaged, cx ≥ 2 cm)
- Oxytocin IV infusion (low-dose or high-dose protocol)
↓
Continuous EFM + uterine monitoring throughout
↓
Goal: Adequate active labour → Vaginal delivery
↓
If hyperstimulation or FHR non-reassuring → Resuscitate + consider C-section
Sources:
- Creasy & Resnik's Maternal-Fetal Medicine: Principles and Practice, Chapter 40 (Induction of Labor)
- Pfenninger and Fowler's Procedures for Primary Care, Chapter 163 (Labor Induction)
- Textbook of Family Medicine, 9th Edition, Chapter 20
What is cerviprime gel What is uterine hyperstimulation What is adequate contractions
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
I have all the content needed. Here is the detailed answer for all three questions:
1. Cerviprime Gel
What it is
Cerviprime is the brand name of Dinoprostone 0.5 mg intracervical gel - a pharmaceutical preparation of naturally occurring Prostaglandin E2 (PGE2) used for cervical ripening before induction of labour.
It is the same drug as Prepidil (another brand name used in the USA). In India, Cerviprime is the commonly used brand.
Drug Profile
| Feature | Detail |
|---|---|
| Generic name | Dinoprostone |
| Drug class | Prostaglandin E2 (PGE2) analogue |
| Brand names | Cerviprime (India), Prepidil (USA) |
| Formulation | 0.5 mg in 2.5 mL gel |
| Route | Intracervical (placed in the cervical canal, not the vaginal fornix) |
| Storage | Must be stored at -20°C to -10°C (frozen); allow to reach room temperature before use |
Mechanism of Action
The cervix during pregnancy is a firm, fibrous, collagen-rich structure that maintains the pregnancy. In the 4-5 weeks before delivery, it undergoes ripening - a hormone-mediated process where:
- Collagen fibres are broken down and remodelled
- Water content increases (cervix becomes softer, more pliable)
- Proteoglycans and glycosaminoglycans change in composition
- The cervix shortens (effaces) and begins to dilate
Endogenous prostaglandins (especially PGE2) drive this ripening process. Cerviprime works by:
- Directly softening the cervix - stimulates collagenase and matrix metalloproteinase release, breaking down collagen
- Increasing cervical pliability - alters the composition of ground substance
- Sensitizing the uterine myometrium to oxytocin, preparing it for contractions
- Stimulating uterine contractions directly (though cervical effect is independent of contraction number)
Dosing Protocol
- Patient is placed in lithotomy position
- Cervical status assessed (Bishop score measured)
- 0.5 mg gel (the full 2.5 mL syringe) is placed into the cervical canal (intracervically) just below the internal os, using the provided catheter
- Patient remains supine for 15-30 minutes after insertion to prevent gel leakage
- EFM monitoring for minimum 2 hours after insertion
- Repeat once after 6-12 hours if Bishop score has not changed appreciably
- Maximum: 2 doses in 24 hours
- If spontaneous labour does not start, oxytocin may be started after an interval
Comparison: Cerviprime Gel vs Cervidil Insert
| Feature | Cerviprime / Prepidil (Gel) | Cervidil (Insert) |
|---|---|---|
| Drug | Dinoprostone (PGE2) | Dinoprostone (PGE2) |
| Dose | 0.5 mg | 10 mg |
| Route | Intracervical gel | Intravaginal slow-release insert |
| Release | Immediate | Slow-release over 12 hours |
| Removable? | No - cannot be removed | Yes - has retrieval string |
| If hyperstimulation? | Cannot remove; terbutaline needed | Remove insert immediately |
| Duration | Repeat every 6-12 h (max 2 doses) | Single 12-hour application |
Contraindications to Cerviprime
- Previous uterine surgery / caesarean section (relative - prostaglandins increase rupture risk)
- Active uterine contractions
- Fetal distress / non-reassuring CTG
- Active vaginal bleeding
- Ruptured membranes (if gel is to be placed intracervically - risk of infection)
- Hypersensitivity to prostaglandins
- Conditions where vaginal delivery is contraindicated (e.g. placenta praevia)
Key Points About Cerviprime
- It acts primarily on cervical connective tissue - the ripening effect is independent of how many contractions it causes
- Misoprostol (PGE1) is more potent and cheaper; meta-analyses show misoprostol gives shorter time to delivery and lower C-section rate - but misoprostol cannot be removed and carries higher hyperstimulation risk
- Cerviprime/Prepidil is preferred over misoprostol in women with a prior caesarean scar (though still used with caution)
- Always have terbutaline 0.25 mg readily available before using Cerviprime, in case hyperstimulation occurs
2. Uterine Hyperstimulation
Definition
Uterine hyperstimulation (also called uterine tachysystole) is defined as:
More than 5 contractions in any 10-minute window (averaged over 30 minutes), OR contractions of moderate to strong intensity in >50% of contractions in a 10-minute segment.
The older term was "hyperstimulation"; the current preferred ACOG/FIGO terminology is tachysystole.
Two Patterns
| Type | Definition | Significance |
|---|---|---|
| Tachysystole alone | > 5 contractions in 10 min, with normal FHR | Monitor closely; may not need immediate intervention |
| Tachysystole with FHR changes | > 5 contractions in 10 min + non-reassuring FHR (decelerations, bradycardia, loss of variability) | Emergency - requires immediate intervention |
The term hyperstimulation is specifically reserved for tachysystole with associated FHR abnormalities or uterine hypertonus.
Why It's Dangerous
Normal contractions allow blood flow to the intervillous space (where gas and nutrient exchange happens) during the relaxation phase between contractions. When contractions come too fast or too close together:
- Relaxation time between contractions is shortened or eliminated
- Intervillous blood flow is chronically reduced
- Fetal hypoxia and acidosis develop
- Placental abruption may occur (excessive pressure)
- Prolonged uterine hypertonus can cause uterine rupture (especially with prior scar)
Causes
- Oxytocin - most common; dose-dependent; easily managed by reducing/stopping infusion
- Prostaglandins (misoprostol, dinoprostone) - cannot be reduced once administered
- Spontaneous - can occur in sensitized uteri (e.g. abruption, infection)
- Prior uterine scar (reduces uterine compliance)
Management of Hyperstimulation
Step-wise approach:
-
Stop or reduce the causative agent:
- Turn off / reduce oxytocin infusion rate
- Remove Cervidil insert (using retrieval string)
- If misoprostol/Prepidil gel: cannot remove - proceed to pharmacological management
-
Lateral (left-lateral) positioning of the mother
- Relieves aortocaval compression
- Improves uteroplacental blood flow
-
IV fluid bolus - 1000 mL lactated Ringer's or normal saline
- Treats hypotension, improves placental perfusion
-
Oxygen 10 L/min via non-rebreather face mask
- Increases maternal pO2, improving fetal oxygenation
-
Tocolysis if contractions do not settle:
- Terbutaline 0.25 mg subcutaneously (β2-agonist - relaxes uterine smooth muscle)
- This is why terbutaline must be pre-stocked before any prostaglandin use
-
Continuous EFM assessment throughout
- If FHR remains non-reassuring after resuscitation → immediate delivery (vaginal or caesarean section)
Prevention
- Use correct doses of oxytocin and prostaglandins
- Never give oxytocin within 2 hours of last misoprostol dose
- Close monitoring with EFM during all inductions
- Have terbutaline available at bedside before starting prostaglandins
- If using oxytocin: titrate to the minimum effective dose
3. Adequate Contractions
Clinical Definition (CTG/External Monitoring)
For labour to progress effectively, contractions should be:
| Parameter | Adequate Contraction Pattern |
|---|---|
| Frequency | 3 contractions per 10 minutes (range: 3-5 per 10 min) |
| Duration | 45-60 seconds each |
| Intensity | Moderate to strong (uterus firms on palpation) |
| Resting tone | Uterus relaxes completely between contractions |
With external tocometry (CTG), only frequency and duration can be measured. Intensity cannot be measured externally because factors like abdominal wall thickness and tocometer placement affect the pressure sensor.
Quantitative Definition - Montevideo Units (MvU)
When adequacy of contractions needs to be objectively measured (especially when labour is not progressing), an Intrauterine Pressure Catheter (IUPC) is inserted to measure actual intrauterine pressure.
Montevideo Units = Number of contractions in 10 minutes × Mean amplitude (mmHg) of each contraction
| Montevideo Units | Interpretation |
|---|---|
| ≥ 200 MvU | Adequate - increasing oxytocin is of no further benefit |
| 180-220 MvU | Active labour - normal range |
| Individual contraction amplitude | 30-80 mmHg each |
| < 200 MvU | Inadequate - increase oxytocin until 200 MvU reached or labour progresses |
Example:
- 4 contractions in 10 minutes, each with mean amplitude 55 mmHg
- MvU = 4 × 55 = 220 MvU → Adequate
Clinical Significance
When labour is not progressing (arrested active phase / failure to progress), you must first determine whether the cause is inadequate contractions (power) or obstruction (passageway/passenger):
- If MvU < 200 → contractions inadequate → increase oxytocin
- If MvU ≥ 200 for 2+ hours with no cervical change → arrest of active phase → consider operative delivery
The diagnosis of active-phase arrest (arrest of dilation) requires:
- No cervical change for 4 hours with adequate contractions (≥200 MvU measured by IUPC), OR
- No cervical change for 6 hours with oxytocin and inadequate uterine activity
This is why IUPC insertion is indicated in cases of protracted or arrested labour - external monitoring cannot give this critical information.
Oxytocin Goal Parameters
When using oxytocin for induction/augmentation, the target contraction pattern is:
- Frequency: 2-3 minutes apart (3-5 per 10 min)
- Duration: 45-60 seconds
- Intensity: 50-75 mmHg on IUPC
- Resting tone: Normal (uterus completely relaxed between contractions)
~90% of patients achieve adequate labour at ≤16 mU/min oxytocin. Doses above 20 mU/min carry risk of water intoxication (antidiuretic effect of oxytocin).
Sources: Pfenninger & Fowler's Procedures for Primary Care, Chapters 163 & 171 | Textbook of Family Medicine 9e | Swanson's Family Medicine Review
This is a shared conversation. Sign in to Orris to start your own chat.